Article Text

Abstract
Posterior reversible encephalopathy syndrome (PRES) may present with diverse clinical symptoms including visual disturbance, headache, seizures and impaired consciousness. MRI shows oedema, usually involving the posterior subcortical regions. Triggering factors include hypertension, pre-eclampsia/eclampsia, renal failure, cytotoxic agents and autoimmune conditions. The mechanism underlying PRES is not certain, but endothelial dysfunction is implicated. Treatment is supportive and involves correcting the underlying cause and managing associated complications, such as seizures. Although most patients recover, PRES is not always reversible and may be associated with considerable morbidity and even mortality.
- stroke
Statistics from Altmetric.com
Introduction
Posterior reversible encephalopathy syndrome (PRES) is a clinicoradiological diagnosis that is based on a combination of typical clinical features and risk factors, and supported by magnetic resonance (MR) brain scan findings. Neurological symptoms can be multiple or occur in isolation and may evolve over the course of the acute phase of the disease. Its classical presentation is a combination of visual loss, headache, altered mental function, seizures and nausea, but may include other focal deficits including weakness, sensory disturbance or speech disturbance. The syndrome of PRES has many underlying causes and may result from medical treatments (eg, antineoplastic therapy) or may develop as part of a PRES-associated medical condition (eg, autoimmune disorders or eclampsia) (box 1).1 2
Conditions associated with the development of PRES
General conditions
Hypertension
Sepsis
Solid organ transplantation
Eclampsia and pre-eclampsia
Renal failure
Malignancy (solid organ and haematological)
Bone marrow transplantation
Stem cell transplantation
Hypomagnesaemia
Hypercalcaemia
Hypercholesterolaemia
Late radiation-associated encephalopathy, for example, SMART
Autoimmune disorders
Rheumatoid arthritis
Crohn’s disease
Systemic lupus erythematosus
Scleroderma
Vasculitis
Neuromyelitis spectrum disorder
Toxins
Scorpion poison
LSD intoxication
Ephedra overdose
Alcohol intoxication
Cocaine
Cytotoxic and immunosuppressive medications
Hydroxydaunorubicin/adriamycin
Vinblastine/vincristine
Gemcitabine
Platinum-containing drugs: cisplatin, oxaliplatin and carboplatin
Bortezomib
Cyclophosphamide
Daunorubicin
Interferon therapy
Capecitabine, 5-fluorouracil
Cytarabine
Etoposide
Corticosteroids
Rituximab
Ciclosporin
Tacrolimus
Sirolimus
Mycophenolate mofetil
Methotrexate
Azathioprine
Other medications
Lithium
Linezolid
Intravenous contrast
Intravenous immunoglobulin
Tyrosine kinase inhibitors
PRES may develop at any age from infants to the elderly, but most frequently affects young or middle-aged adults, with a mean age of 45 years.1 3 There appears to be a female predominance, even after excluding patients with eclampsia.2 4 5 Among adults, PRES is present in up to 98% of patients with eclampsia6; in 2.7%–25% of patients following bone marrow transplantation7 8; in 0.4%–6% of patients following solid organ transplantation9; and less commonly (0.4%–0.8%) in end-stage renal disease or systemic lupus erythematosus.10–12
PRES is in the differential diagnosis of many acute neurological presentations; the key to its diagnosis is to have a high index of suspicion in several scenarios when there are consistent findings on MR brain scan. The following sections deal with a clinical approach to the diagnosis and management of PRES.
Acute evaluation
Early on, what information do I need and what should I look for?
PRES often presents non-specifically with symptoms manifesting over several hours or days.1 Encephalopathy develops in 28%–94% of patients and ranges from mild confusion and cognitive deficits to stupor and sometimes coma.1–3 Seizures affecting up to 74%–87% of patients1 2 and typically occur within 24–48 hours of presentation13 14; in a minority (3%–17%), seizures may evolve into status epilepticus, and rarely this is the presenting symptom.
Headaches develop in up to half of patients with PRES3 and are usually dull, diffuse and gradual in onset. A thunderclap headache can occur in the context of PRES but should raise the suspicion of reversible cerebral vasoconstriction syndrome (RCVS). This condition occurs in the context of similar risk factors to PRES but is distinguished mainly by thunderclap headache, cerebral vasculopathy, infarction, and subarachnoid or intracranial haemorrhage.15–21
Despite PRES often affecting the occipital regions, only 39% of patients have visual symptoms.1 3 These include reduced visual acuity, diplopia, visual field deficits, cortical blindness, colour vision abnormality and visual hallucinations. Focal neurological deficits such as aphasia and hemiparesis occur in 19% of patients.3
Because the symptoms linked to PRES commonly occur in other conditions, its diagnosis is challenging and requires clear communication among clinicians and with radiologists. It is essential to review the patient’s current and medical history, medication charts and examination findings, including blood pressure and level of consciousness. Despite PRES being associated with accelerated hypertension, about 20%–30% of patients are normotensive or hypotensive during initial evaluation, especially when PRES is due to medications or systemic conditions other than hypertension or eclampsia.4 21
PRES is associated with numerous conditions and iatrogenic causes (box 1), though most frequently with hypertension, renal failure, eclampsia, transplant and immunosuppressive use, sepsis, autoimmune disorders and exposure to cytotoxic medications.22–24 Rarer iatrogenic causes include linezolid,25 intravenous immunoglobulin26 and intoxication with LSD,27 cocaine,28 and even scorpion poisoning.29
What baseline tests should I perform?
MR scan of the brain assists with confirming the diagnosis of PRES and in showing its extent. It is therefore preferred to CT scanning due to its superior resolution, especially of posterior fossa structures. Nevertheless, CT scanning is usually the first form of imaging acutely and PRES is often diagnosed using CT scan alone. The typical CT and MRI features of PRES include almost symmetrical hemispheric vasogenic oedema affecting subcortical white matter and often extending to the overlying cortex, best seen on MRI with fluid-attenuation inversion recovery (FLAIR) sequences.22 MRI diffusion-weighted imaging usually confirms vasogenic oedema with absence of restricted diffusion. Postcontrast enhancement occurs in 38%–50% of patients23 30 31 in one of three patterns: a leptomeningeal pattern, a cortical pattern within regions of altered FLAIR signal or a combined pattern (figure 1).4 31

Imaging findings in typical PRES. MR scan of the brain of a 39-year-old woman with PRES who presented with visual disturbance, seizure and fever. (A–C) Prominent cortical and subcortical white matter signal hyperintensity on T2 FLAIR involving bilateral occipital and left anterior parietal lobe, left frontal lobe, and the splenium of the corpus callosum with additional foci involving both the anterior left thalamus and posterior left putamen. There are also patchy hyperintense T2 FLAIR signal foci within the right cerebellar hemisphere. (D,E) Areas of diffusion-weighted imaging hyperintensity and hyperintense apparent diffusion coefficient signal involving the occipital cortex bilaterally consistent with vasogenic oedema, which corresponds to regions of high T2 signal on the FLAIR images. (F) There is a small focus of blooming within the left occipital lobe, in keeping with petechial haemorrhage. FLAIR, fluid-attenuated inversion recovery; PRES, posterior reversible encephalopathy syndrome.
Brain imaging shows bilateral cortical–subcortical vasogenic oedema that falls into three anatomical patterns seen in about 70% of patients: a dominant parieto-occipital pattern (22%), a holohemispheric watershed pattern (23%); and superior frontal sulcus pattern (27%).4 32 A central-variant (brainstem) pattern has also been identified, affecting the brainstem, basal ganglia, posterior limb of the internal capsule, cerebellum and periventricular regions, but has no cortical or subcortical involvement.33 PRES may rarely even involve the spinal cord.34 Frontal and temporal lobe involvement can occur in up to 75% of cases,4 but in practice, these patterns are commonly mixed; PRES with such combined patterns is actually more common than PRES with isolated parieto-occipital involvement.4 35
Intracranial haemorrhages are found on imaging in 10%–25% of cases, mostly intraparenchymal or subarachnoid.31 36 Up to 65% of patients who undergo follow-up MRI with susceptibility-weighted imaging have microhaemorrhages.31 PRES-associated intracranial haemorrhage probably results either from reperfusion injury in the setting of vasoconstriction or from pial vessel rupture secondary to severe hypertension.37
PRES and RCVS are well known to overlap, and so cerebral CT or MR angiography is recommended to help to distinguish them.15 16 In RCVS, vessel wall MR angiography shows arterial wall thickening but without arterial wall enhancement, consistent with transient vasoconstriction.38 However, PRES occurs in 9%–38% of RCVS cases,15–18 and 87% of PRES cases have angiographic changes consistent with RCVS, such as diffuse vasoconstriction, focal vasculopathy or vessel pruning.39 Therefore, it is conceivable that PRES and RCVS are divergent phenotypical manifestations of a shared pathophysiology.20
Laboratory investigations should be guided by the clinical context. It is reasonable to take an initial blood panel of full blood count, renal function, electrolytes, liver function tests, ammonia and a urine toxicology screen. Patients with significant unexplained hypertension need specific testing for secondary causes of hypertension, such as a phaeochromocytoma, Conn’s syndrome or Cushing’s syndrome. If clinically indicated, and given the association of PRES with autoimmune disease, it is worth considering a serum vasculitis screen including antinuclear antibody, antineutrophil cytoplasmic antibody, extractable nuclear antigens, rheumatoid factor, complement, lupus anticoagulant, anticardiolipin antibodies, paraproteins, ACE, HIV serology, erythrocyte sedimentation rate and C reactive protein. Cerebrospinal fluid (CSF) examination is usually not necessary in clear cases of PRES, unless atypical MRI patterns make it important to exclude an alternative diagnosis such as encephalitis or demyelination (figure 2). Obviously a lumbar puncture should not be performed if there are signs of raised intracranial pressure.
{kind=link}
{kind=link}
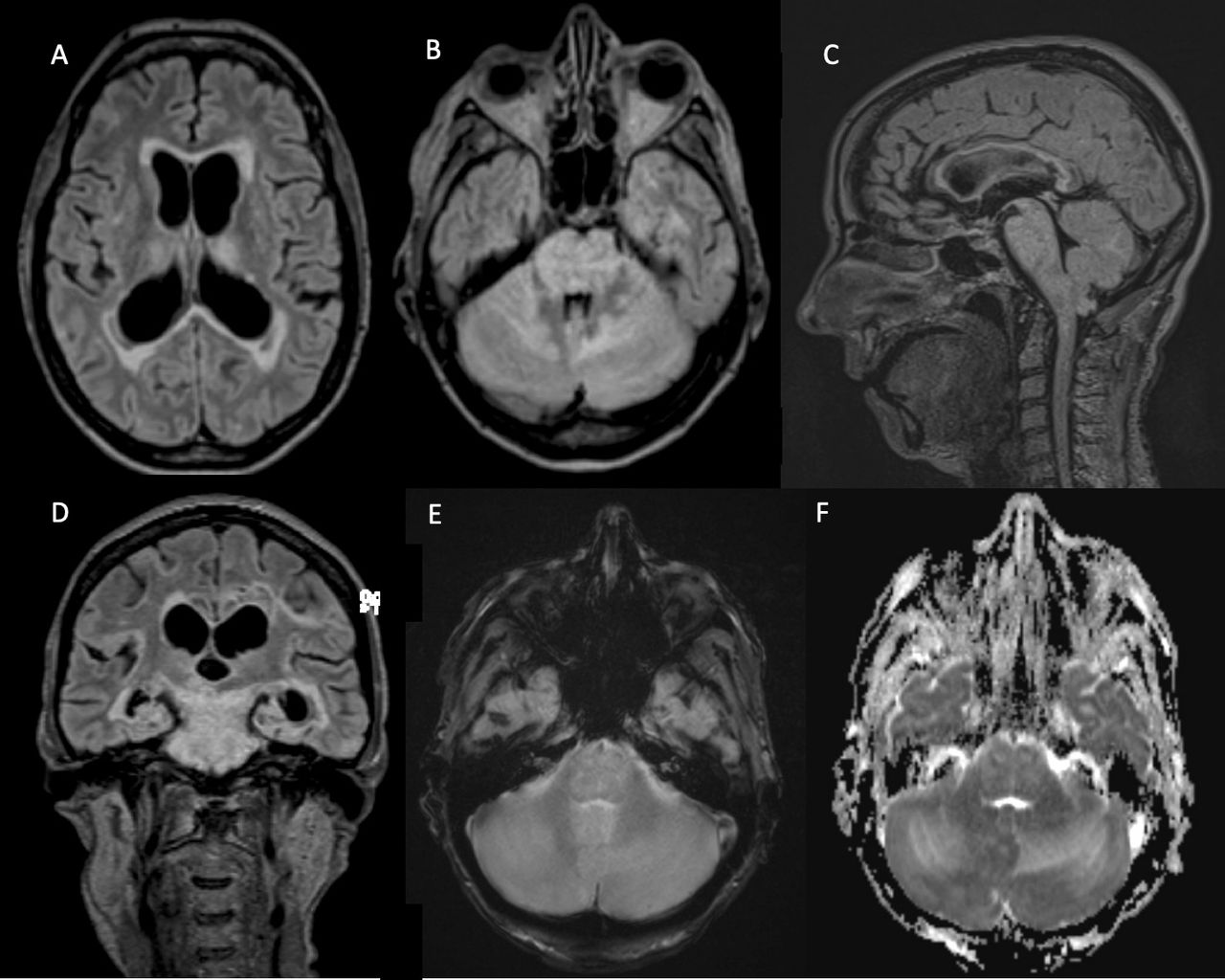
Imaging findings in atypical PRES. MR scan of the brain of a 45-year-old woman with PRES and a history of multiple sclerosis who presented with reduced level of consciousness. (A,B) Axial FLAIR sequence shows extensive brainstem, cerebellar, bilateral thalami, corpus callosum and bilateral anterior temporal lobe hyperintense signal change. (C) Sagittal FLAIR sequence shows extensive brainstem and corpus callosum hyperintensities. (D) Coronal FLAIR showing confluent brainstem, bilateral temporal lobe and left parietal lobe hyperintensities. (E,F) Areas of diffusion-weighted imaging hyperintensity and hyperintense apparent diffusion coefficient signal involving the midbrain and bilateral cerebellar hemispheres consistent with vasogenic oedema, which corresponds to regions of high T2 signal. FLAIR, fluid-attenuated inversion recovery; PRES, posterior reversible encephalopathy syndrome.
Do I need to request further imaging?
Most cases of PRES do not need formal digital subtraction angiography, but it is worth considering this in patients with possible RCVS or those in whom CT or MR angiography shows a possible intracranial arteriopathy. Digital subtraction angiography may identify typical features of RCVS or of cerebral vasculitis, leading to specific therapies for each, including calcium channel blockers for RCVS or immune therapy for cerebral vasculitis.
Differential diagnoses of PRES
Table 1 shows the numerous conditions that clinicians need to consider in the differential diagnosis of PRES. While not all of these would be mistaken for classic PRES, they share clinical and/or radiological features with PRES that could lead to diagnostic confusion. The most important differentials include viral and autoimmune encephalitis, demyelinating disease, toxic leucoencephalopathies, malignancy such as gliomatosis cerebri, CNS vasculitis, central/extrapontine myelinolysis and acute stroke, especially due to cerebral venous thrombosis.32 A history of prior radiation exposure might suggest stroke-like migraine attacks after radiation therapy syndrome. Differentiating PRES from these other conditions requires a thorough review of risk factors, additional targeted testing and follow-up imaging.32
Imaging and other key findings distinguishing between differential diagnoses
Management
How do I approach the acute management of PRES?
The acute management of PRES is supportive and includes removing or reversing any suspected cause, for example, correcting hypertension (table 2). There have been no randomised trials on the various interventions used to treat PRES, and treatment guidelines are generally by consensus opinion. It is essential to recognise the condition promptly and to remove or reverse the precipitating factor, including chemotherapy or an immunosuppressive agent.1 Patients need to be hydrated and to have any electrolyte disturbances corrected. Patients in whom cerebral oedema is causing raised intracranial pressure may require neurosurgical measures (see What about cases of malignant PRES? section)
Acute therapies for PRES
Patients with acute hypertension should have their blood pressure gradually reduced by no more 20%–25% in the first few hours to avoid the risk of cerebral, coronary and renal ischaemia.40 Clinicians should aim for a mean arterial pressure of between 105 and 125 mm Hg, and continuous intravenous infusions are often required. First-line antihypertensive agents include nicardipine (5–15 mg/hour), labetalol (2–3 mg/min) and nimodipine; second-line agents include sodium nitroprusside, hydralazine and diazoxide.41 Nitroglycerine is not recommended in patients with PRES as it may aggravate cerebral oedema.42 Table 1 details the antihypertensive agents recommended for managing PRES.
Once PRES is suspected, clinicians should consider transfer to an intensive care setting, as up to 70% of patients ultimately require intensive care for symptom management,43 and 35%–40% require mechanical ventilation for 3–7 days.1 44 Indications for transfer to an intensive care unit setting include encephalopathy, seizures, ventilatory depression and the need for invasive blood pressure support.43
Management of PRES in specific situations
It is crucial for neurological improvement that patients with intraparenchymal or subarachnoid haemorrhage should have their blood pressure gradually reduced.45 Those with marked renal failure need prompt dialysis. Pregnant women should be considered for early delivery46 and should best avoid ACE inhibitors.
Patients who develop status epilepticus require emergency management with benzodiazepines and loading doses of sodium valproate, levetiracetam or phenytoin (table 2). However, there are no standard guidelines for managing PRES-associated seizures without status epilepticus, and here treatment with antiseizure medications is decided on an individual basis. Epilepsy develops in only 1.0%–3.9% of patients who suffer a PRES-associated seizure,13 47 and so most patients do not need long-term antiseizure medications; clinicians should consider weaning and stopping these medications once the acute phase of PRES has resolved.
What about cases of malignant PRES?
Malignant PRES is defined based on clinical criteria consisting of a Glasgow Coma Scale (GCS) score of <8 and clinical decline despite standard medical management for elevated intracranial pressure. In addition, there must be radiological evidence of oedema or intracerebral haemorrhage exerting mass effect, such as effacement of basal cisterns, transtentorial, tonsillar or uncal herniation.48 Malignant PRES requires aggressive supportive care that may include mechanical ventilation, transfusion of blood products for reversal of coagulopathy and corticosteroids for those with autoimmune disorders. Patients with PRES whose GCS score is ≤8 should have intracranial pressure monitoring whenever possible.48 Various interventions undertaken in patients with raised intracranial pressure include osmotherapy, CSF drainage by external ventricular drain, craniectomy and evacuation of haematomas; these are reported to reduce mortality rates in comparison to historic reports.49 50 Patients with acute obstructive hydrocephalus may require an external ventricular drain.51
Long-term management of PRES
Retrospective studies suggest that recurrent PRES occurs in 4% of patients,52 especially in those with persistent risk factors such as sickle cell crises, autoimmune conditions, hypertensive crises, renal failure and mitochondrial disorders.53
Although PRES was initially described as benign, wholly reversible and with a good prognosis, its mortality is around 19%, and about 44% of patients are left with varying degrees of functional impairments.3 54 Follow-up imaging may find residual structural lesions in 40% of cases.5
Factors associated with poor outcomes include severe encephalopathy, a hypertensive cause, hyperglycaemia, a neoplastic cause, a longer time to control the causative factor, the presence of multiple comorbidities, elevated C reactive protein, low CSF glucose and coagulopathy.3 54–56 Various imaging features associated with poor outcome include corpus callosum involvement, extensive cerebral oedema or worsening imaging severity, intracerebral haemorrhage, subarachnoid haemorrhage and restrictive diffusion on imaging.30 55 57 58
It is difficult to identify a single predictor of outcome in PRES. Several studies have found a correlation between the degree of hypertension and both the clinical outcome and severity of oedema on imaging, but the presence or patterns of gadolinium-based contrast enhancement does not correlate with functional outcomes.30
The occurrence of seizures during the acute phase is not associated with increased length of hospital stay, morbidity, mortality or nursing home placement on discharge.13 14 43 Despite a high frequency of seizures during the acute phase, patients have only a low risk of long-term unprovoked seizures, and epilepsy is rare.13
What do I need to know about the pathophysiology of PRES?
The mechanism underlying the development of PRES is poorly understood. PRES is a disorder of dysregulated perfusion of the brain, typically resulting in reversible vasogenic oedema. There are several theories regarding the cerebral vasculature dysregulation in PRES, but no single mechanism explains the development of PRES in all cases.59 Thus, multiple non-exclusive mechanisms probably contribute, including excessive hypertension, impaired cerebral autoregulation causing cerebral hyperperfusion and endothelial dysfunction.32 The posterior circulation may be more vulnerable to hyperperfusion as it has less sympathetic innervation to counter reflex parasympathetic vasodilation.60 Patients with PRES commonly have acute fluctuations in blood pressure, but it is not known whether these are the cause or a secondary effect of the syndrome.32 61 Endothelial dysfunction may result, either directly or as a downstream effect, from the secretion of cytokines, including tumour necrosis factor alpha, interleukin-1, interferon gamma and vascular endothelial growth factor.62
Conclusion
PRES is a neurological condition that commonly presents with visual disturbance, seizures and encephalopathy, and has a wide range of causes including hypertension, pre-eclampsia, renal failure and immunosuppression. Its diagnosis is facilitated by the characteristic MR brain scan changes of posterior subcortical oedema. Its treatment involves correcting identifiable triggers and supporting patients through the acute phase of the illness. The prognosis is generally favourable but more severely affected patients require intensive care support and may be left with residual neurological deficits. Key areas for further research are to gain a better understanding of its pathophysiology and to obtain better data regarding the need for long-term treatment of seizures with antiseizure medications.
Key points
Posterior reversible encephalopathy syndrome (PRES) most commonly presents with visual disturbance, seizures and altered consciousness.
PRES can occur in the context of hypertension, renal failure, autoimmune disease and with the use of immunosuppressive therapy or chemotherapy.
MR scan of the brain confirms the oedema, which is often, but not exclusively, in posterior cortical and subcortical structures.
The treatment of PRES can be challenging but should be implemented early to minimise the potential for significant morbidity and mortality that can occur in more severe cases.
Further reading
Bartynski WS, Boardman JF. Distinct imaging patterns and lesion distribution in posterior reversible encephalopathy syndrome. AJNR Am J Neuroradiol. (2007) 28:1320–7.
Singhal AB, Hajj-Ali RA, Topcuoglu MA, et al. Reversible cerebral vasoconstriction syndromes: analysis of 139 cases. Arch Neurol 2011;68:1005–12.
Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions.Lancet Neurol.(2015) 14:914–25.
Ethics statements
Patient consent for publication
Ethics approval
This study does not involve human participants.
References
Footnotes
Contributors JDT, AGK and TH undertook design of the article, drafting of the article and critical review of the article. MAK undertook drafting of the article and critical review of the article.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Commissioned. Externally peer reviewed by Aaron Berkowitz, Pasadena, California, USA.
Linked Articles
- Editors’ commentary
Other content recommended for you
- The posterior reversible encephalopathy syndrome: what's certain, what's new?
- Reversible cerebral vasoconstriction syndrome
- Pharmacovigilance during treatment of multiple sclerosis: early recognition of CNS complications
- Thunderclap headache
- Cerebral-autoregulatory dysfunction syndrome
- Controversy of posterior reversible encephalopathy syndrome: what have we learnt in the last 20 years?
- Convexity subarachnoid haemorrhage: a practical guide
- Reversible cerebral vasoconstriction syndrome (RCVS) caused by over-the-counter calcium supplement ingestion
- Postpartum headache: diagnostic considerations
- Postpartum vertebral artery dissection with posterior reversible encephalopathy syndrome