Article Text

Statistics from Altmetric.com
Introduction
There are many options for treating convulsive status epilepticus but one thing is clear: success is closely associated with timely intervention and adherence to a treatment protocol.1 Delayed intervention leads to treatment resistance and refractory status. There is little evidence from randomised controlled trials, especially for agents used after benzodiazepines.2 Therefore, for now, the choices are mostly based not on Class 1 evidence but on accumulated and published experience.
Management protocols are mandatory if patients with status epilepticus are to receive prompt and appropriate treatment. Yet many hospitals do not have these or do not review them regularly. This protocol is adapted from that of King's College Hospital, London, UK, and is in line with the European consensus workshop.2 We aim to provide sufficient detail to satisfy the treating physician's practical requirements, while keeping the protocol simple and easily accessible. It should be used with precalculated dose/weight charts.
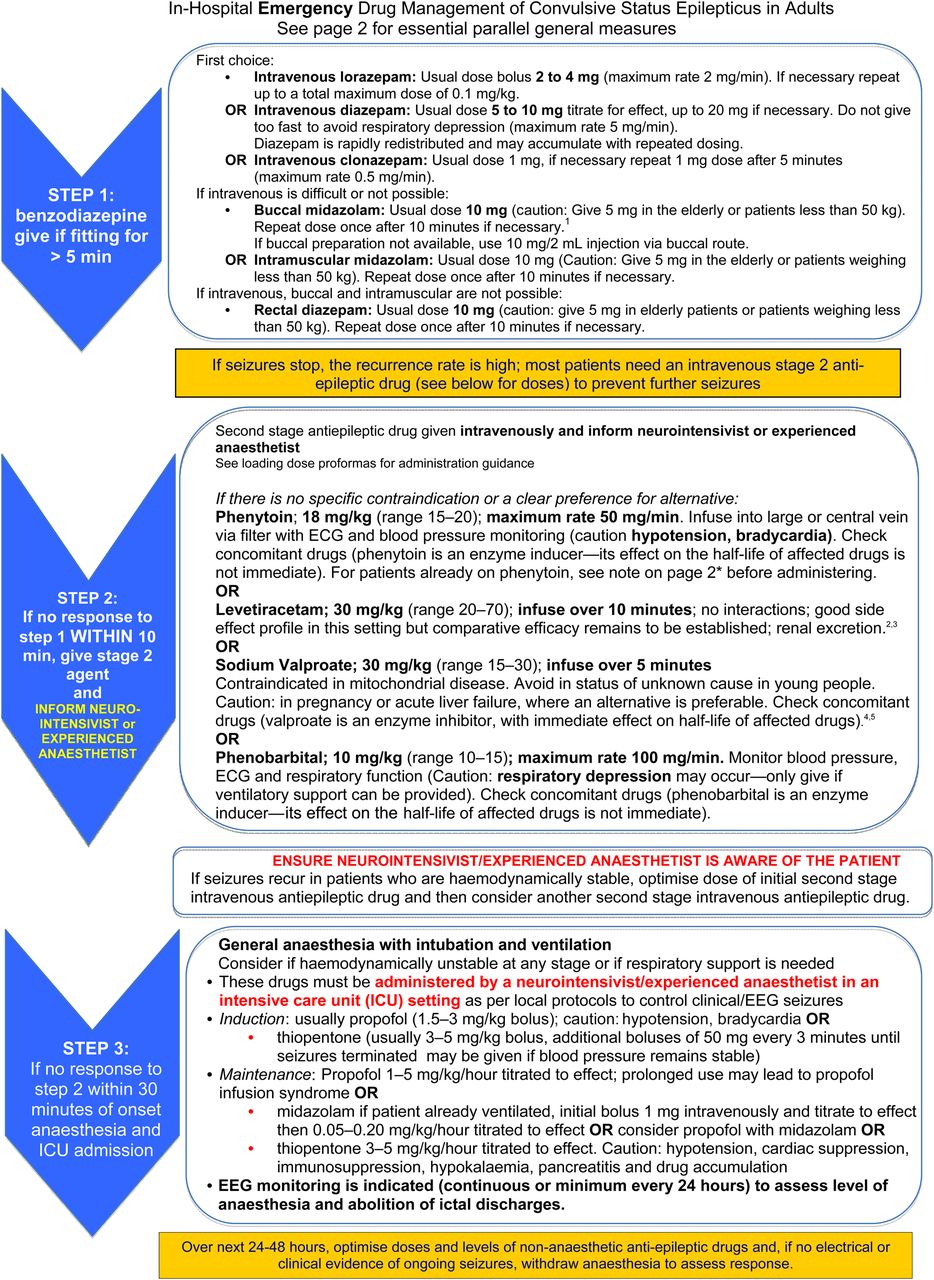
The treatment pathway comprises first benzodiazepine (first line), then an intravenous antiepileptic agent (second line) followed by, where necessary, general anaesthesia (third line). The choice of benzodiazepine and the route used remains open to discussion. While intravenous lorazepam remains the first choice in hospital, it is not always available and intravenous access is not always possible. Furthermore, the choice of benzodiazepine and its route of administration need revising as new evidence emerges, particularly given the success of intramuscular midazolam in the prehospital setting.3 To allow for different circumstances, drug availability and access, we list several options for stage 1 treatment with benzodiazepines.
With regards to choice of intravenous antiepileptic drug in the second stage, the limited available evidence prevents us from categorically choosing one over another. We have, however, suggested an order of preference; this is influenced more by local availability and familiarity with use in the emergency department rather than evidence of superiority. The order should be reviewed as further evidence emerges. Irrespective of the drug chosen, we stress the importance of giving adequate loading doses. We have selected doses in the middle of the usual ranges, recognising that these may need to change with time. Where there is a clear response but not full control of seizures, in a stable patient, it may be appropriate to optimise the antiepileptic drug dose, as well as to consider another second stage agent. Otherwise, treatment should promptly move to the general anaesthesia stage. We have not listed lacosamide—available intravenously and occasionally used in status epilepticus—among the second-stage agents: this needs reassessing as more evidence emerges. It is uncertain whether the doses need capping, depending on weight. This need probably varies with different drugs and also depends on the doses per kg body weight used. There is limited information using loading doses above 2500 mg for phenytoin, 4000 mg for levetiracetam and 3000 mg for valproate: we suggest that their doses should be capped—as is usual clinical practice—though we acknowledge the lack of clear evidence.⇓⇓


{kind=link}
{kind=link}
This protocol will hopefully fulfil requirements for most cases of status epilepticus and readers are welcome to download and adapt it for local use along with the precalculated dose-weight charts. It does not address cases where seizures continue despite adequate and appropriate general anaesthesia (refractory status epilepticus),4 which need specialised input, with several other possible treatment options considered, including other antiepileptic drugs, ketamine, corticosteroids, magnesium, intravenous immunoglobulin, ketogenic diet, neurostimulation and, for lesional cases, surgery.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online supplement
Footnotes
See the next 2 pages for the Protocol.
-
Contributors LN conceived the protocol, and LN and SJ initiated the protocol design and content. CP provided expert information regarding neuroanaesthetic management of status epilepticus. ET provided expert review and comments during protocol development. LN produced the introductory manuscript presented with the protocol after discussion with ET. All authors contributed to refinement of the protocol and manuscript and approved the final copy.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Aiden Neligan, London, UK and Eelco Wijdicks, Rochester, USA.
Linked Articles
- Editors' choice
Other content recommended for you
- Compliance with status epilepticus management protocol and effect on clinical outcomes in children with status epilepticus
- The management of refractory generalised convulsive and complex partial status epilepticus in three European countries: a survey among epileptologists and critical care neurologists
- Question 1: Is there a role for the ketogenic diet in refractory status epilepticus?
- Multicentre observational status-epilepticus registry: protocol for ICTAL
- Generalised convulsive status epilepticus: an overview
- New-onset refractory status epilepticus (NORSE)
- Continuous EEG use and status epilepticus treatment in Australasia: a practice survey of Australian and New Zealand epileptologists
- Predictors and prognosis of refractory status epilepticus treated in a neurological intensive care unit
- Management of convulsive status epilepticus in children
- Continuous midazolam infusion as treatment of status epilepticus