Article Text

Abstract
Non-motor symptoms are a key component of Parkinson's disease, possibly representing a clinical biomarker of its premotor phase. The burden of non-motor symptoms can define a patient's health-related quality of life. Non-motor symptoms substantially increase the cost of care—requiring increased hospitalisation and treatment—and pose a major challenge to healthcare professionals. However, clinicians often regard non-motor symptoms and their management as peripheral to that of the motor symptoms. Here, we address the clinical issues and unmet needs of non-motor symptoms in Parkinson's disease.
- PARKINSON'S DISEASE
- NON MOTOR SYMPTOMS
- NMSQuest
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
Statistics from Altmetric.com
Introduction
I have Parkinson's. I would like you to address the following symptoms that bother me the most: sleep, pain and then my movement disorder.
A patient with Parkinson's disease, 10 October 2013
James Parkinson recognised the implications and importance of motor Parkinson's disease (PD) in 1817 and highlighted key non-motor symptoms, such as sleep dysfunction, dysautonomia, cognitive and neuropsychiatric issues. However, it was almost 150 years before the importance of the burden of non-motor symptoms on the lives of the people with Parkinson's and the carers became apparent. Many studies have addressed cognition, dementia, sleep disorders and depression in PD. More recently, holistic tools, such as the self-rated Non-Motor Symptoms Questionnaire (NMSQuest)1 and the Non-Motor Symptoms Scale (NMSS)2 ,3 have allowed clinicians to quantify the overall burden of these additional symptoms in PD and their impact on quality of life.
The problems
Clinicians frequently overlook non-motor symptoms and do not discuss important symptoms like depression, anxiety, fatigue and sleep disturbance.4 The UK's National Institute for Health and Care Excellence—a non-departmental public body of the Department of Health—has recognised non-motor symptoms and their management as an important area of unmet need in PD.5 However, despite their 2006 guidance, an international survey in 2010 showed that up to 62% of PD patients do not declare symptoms such as apathy, pain, sexual difficulty, bowel incontinence or sleep disorder, either through embarrassment or being unaware that their symptoms link to PD.6 Furthermore, clinicians themselves may not realise that these symptoms need addressing. Non-motor symptoms are common even at first presentation. In 2013, a German study assessed them (by the NMSQuest) in untreated PD patients at presentation: these symptoms presented a significant burden—even at this early untreated stage—compared with age-matched controls.7 A UK-based study reported similar findings, highlighting the important need for an awareness of non-motor symptoms right at the onset of ‘motor’ PD.8 Their under-reporting has important therapeutic and societal implications as most are treatable. Left untreated, non-motor symptoms detrimentally affect quality of life and frequently cause hospitalisation and institutionalisation,9 ,10 increasing the cost of PD care by fourfold.6
Initiatives to address management of non-motor symptoms
Parkinson's UK—the major UK-based patient charity—commissions an annual audit of Parkinson services. The 2011 report showed non-motor symptoms recorded in only 21% of elderly care and 9% of neurology services in the UK. This deficiency mainly relates to lack of time during consultation and also to not using self-declaration tools, which would allow patients to ‘flag’ symptoms. This outcome led to a national policy for data collection (motor and non-motor) of patients being referred to hospital.11
The neuropathological basis of non-motor Parkinson's
For the nigrostriatal dopaminergic disorder of PD, one pathological process clearly does not fit all! Jellinger stated that Parkinson's can no longer be considered a complex motor disorder characterised by extrapyramidal symptoms, but as a progressive multisystem disease—or more correctly, multiorgan disease—with variegated neurological and non-motor deficiencies.12
The traditional concept that the first neuropathological insult leading to PD is the degeneration of neuromelanin-containing neurones in the pars compacta of the substantia nigra (resulting in depleted levels of the dopamine) has been challenged. Many studies, spearheaded by the Braak theory, suggest that a non-dopaminergic process is key to the non-motor symptoms of PD, many of which start well before the motor Parkinson's features emerge.12–14 Interestingly, Friedrich Lewy (1913) first described Lewy bodies in the dorsal motor nucleus of the vagus, a site implicated in Braak stage 2.15
Table 1 summarises the growing evidence that in PD the degeneration of non-dopaminergic neurones occurs well before dopaminergic motor symptoms start. There is also clear evidence of differential neuronal degeneration involving several neuropeptide pathways in the brain in PD.13 ,14 Furthermore, there is neuropathological heterogeneity between early-onset and late-onset PD,13 which manifests clinically as subtypes within both motor PD and (more recently recognised) non-motor PD.16
Animal models addressing non-motor symptoms of PD are important. We discuss these in online supplementary material, and box 1 shows a snapshot of existing animal models.
Non-dopaminergic involvement in PD
Parkinsonian animal models with possible expression of non-motor symptoms and exploration of pathophysiology
6-OHDA lesioned rodents24
-
Sensorimotor
-
Olfaction
-
Sensory/pain threshold
-
Sleep/wakefulness
-
Circadian rhythms
-
Cognitive function
-
Also possible to study:
-
Altered cardiovascular function
-
Bladder hyperactivity
-
Altered motility of gastro-intestinal tract
-
α-Synuclein overexpressor (ASO=Thy1-aSYN) mice25
-
Olfaction
-
Autonomic
-
Constipation
-
Sleep
-
Cognition
MPTP-treated primates24
-
Bladder hyper-reflexia
-
Constipation
-
Drooling
-
Altered cardiovascular function
-
Sleep disturbance
-
Cognitive disturbance
Mice model of intragastric rotenone administration26
-
α-Synuclein accumulation in dorsal vagal nucleus
-
Potential for investigating autonomic symptoms such as constipation
Göttingen minipigs (Ellegaard Minipigs ApS)27
-
Cognition/sleep
OHDA, hydroxydopamine; MPTP, 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine.
What are the non-motor symptoms of PD?
James Parkinson referred to sleep disturbance, constipation, dysarthria, dysphonia, dysphagia, sialorrhoea, urinary incontinence and ‘at the last, constant sleepiness with slight delirium’ in his essay.28 The widespread neuropathology of PD gives a wide range of symptoms from gastrointestinal to sleep disorders, from cognitive to apathy and depression. In addition, some symptoms relate to drug therapy. It is thus difficult to ‘lump’ non-motor symptoms into a single category, and we suggest the following classification:
-
Related to the disease process or pathophysiology
-
Dopaminergic origin
-
Non-dopaminergic origin
-
-
Related to a partial non-motor origin (usually brainstem autonomic impairment with motor end result, such as constipation or diplopia)
-
Related to non-motor fluctuations (cognitive, autonomic and sensory subtypes)
-
Fluctuating
-
Constant
-
-
Related to PD drug therapy
-
Specific symptoms (eg, hallucinations, delirium)
-
Syndromes—impulse control disorders, dopamine agonist withdrawal syndrome, Parkinson's hyperpyrexia syndrome (thermoregulatory failure, delirium)
-
-
Possibly genetically determined
-
Dementia in cases with glucocerebrosidase mutation
-
Depression and sleep disorders in cases with leucine-rich repeat kinase-2 mutation
-
Some symptoms may overlap: for instance, hallucination as part of the advancing disease, or non-motor fluctuations in PD.
While some non-motor symptoms dominate in the early or even in the ‘premotor’ phase of PD, others complicate the clinical picture throughout the disease (pain, fatigue) and especially in its advanced stages (dementia, apathy, dysautonomia), as shown in the Sydney multicentre study report at 20 years.29 The ‘Parkinson's at risk syndrome’ study tries to identify the premotor non-motor risk factors for developing the motor syndrome of PD. There is now also an attempt to redefine PD, moving away from the typical brain bank-defined motor diagnostic criteria.30–32
PD can be divided into a preclinical phase (supported by molecular or imaging markers), a premotor phase (with non-motor symptoms, table 2) and the motor phase, the ‘tip of the iceberg’. The key is to develop robust biomarkers and also to define the specific predictive value of the premotor non-motor symptoms. Table 2 shows examples of non-motor symptoms reported in the premotor stage.
Non-motor symptoms in the premotor PD
Epidemiology
The NMSQuest and the NMSS each assesses their global burden in PD. Table 3 lists the studies that have used them to assess non-motor symptoms in unselected PD populations across the world and shows the importance of these symptoms in PD irrespective of cultural background, racial origin and hospital settings. Three controlled studies compared NMSQuest data in PD with age-matched healthy controls: all show that while some symptoms, such as insomnia, urinary difficulties and memory issues, are common in ‘normal’ subjects, the severity and frequency of these non-motor symptoms are more severe in PD. Furthermore, some symptoms, such as fatigue, dribbling of saliva and excessive daytime sleepiness, are highly significantly more common in PD.1 ,7 ,8
Biomarkers
There are several suggested biomarkers, both tissue and imaging, but all remain investigational. A controlled study from Germany comparing untreated PD with age-matched controls suggested that clinical tools such as the NMSQuest and a validated bedside autonomic scale (SCOPA-autonomic), combined with laboratory tests such as the smell-identification test, reach the sensitivity and specificity (>0.9) for a biological marker of PD at presentation.7 Table 4 lists other possible biomarkers in PD.
Some reported possible biomarkers in the early diagnosis of PD
Some probable biomarker tests and kits
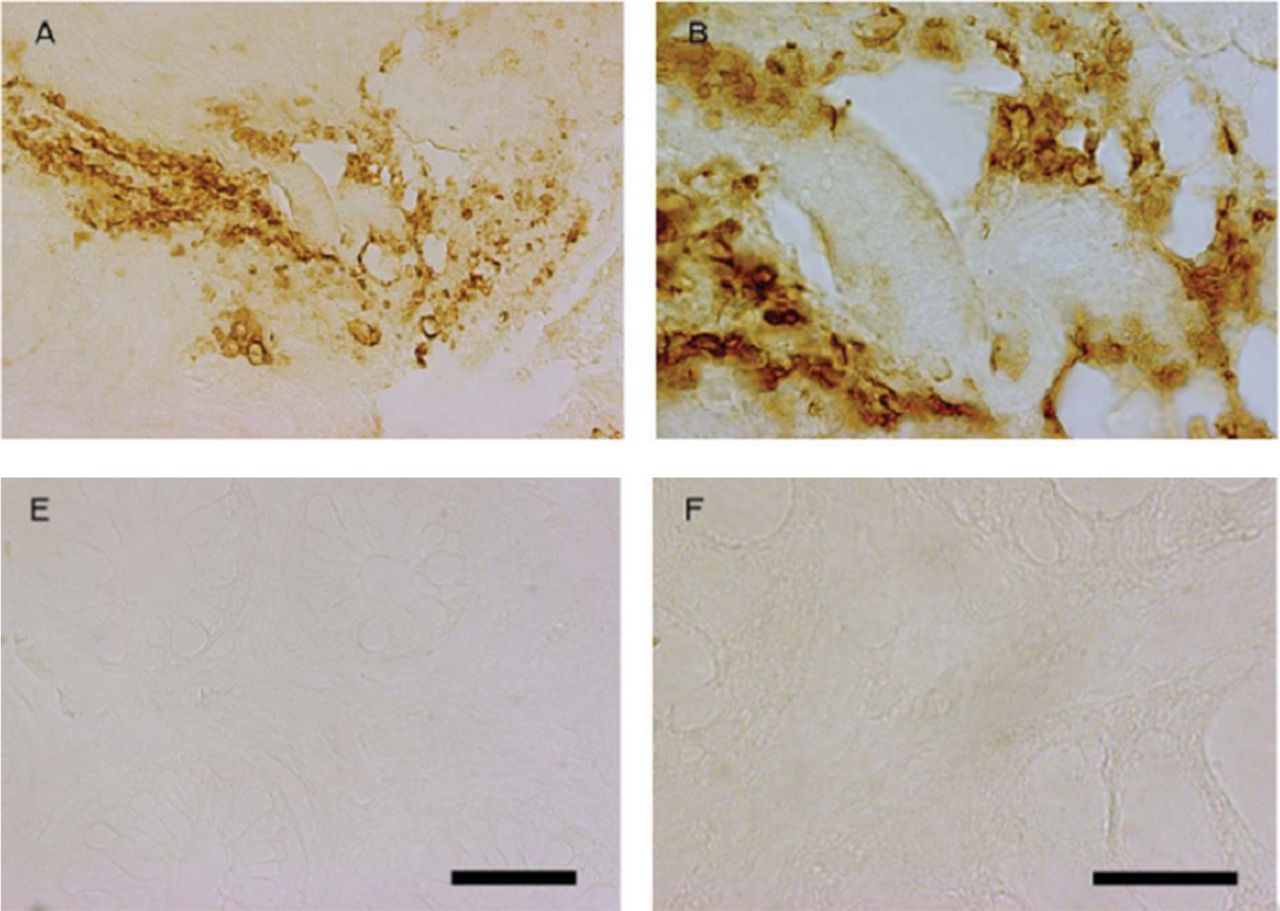
(A) Showing 10 untreated Parkinson patients; all positive for α-synuclein and 3-nitro-tyrosin (a marker for mitochondrial stress) on sigmoidoscopy and rectal biopsy (A,B). From Shannon et al.45 Copyright 2011 Movement Disorder Society. Reproduced with permission from John Wiley and Sons, Inc. (B) Controls show no relevant staining (E,F). From Shannon et al.45 Copyright 2011 Movement Disorder Society. Reproduced with permission from John Wiley and Sons, Inc.
University of Pennsylvania smell-identification test for testing olfaction in the clinic.
The clinical scenario: a possible solution to the neglect of non-motor symptoms in clinic
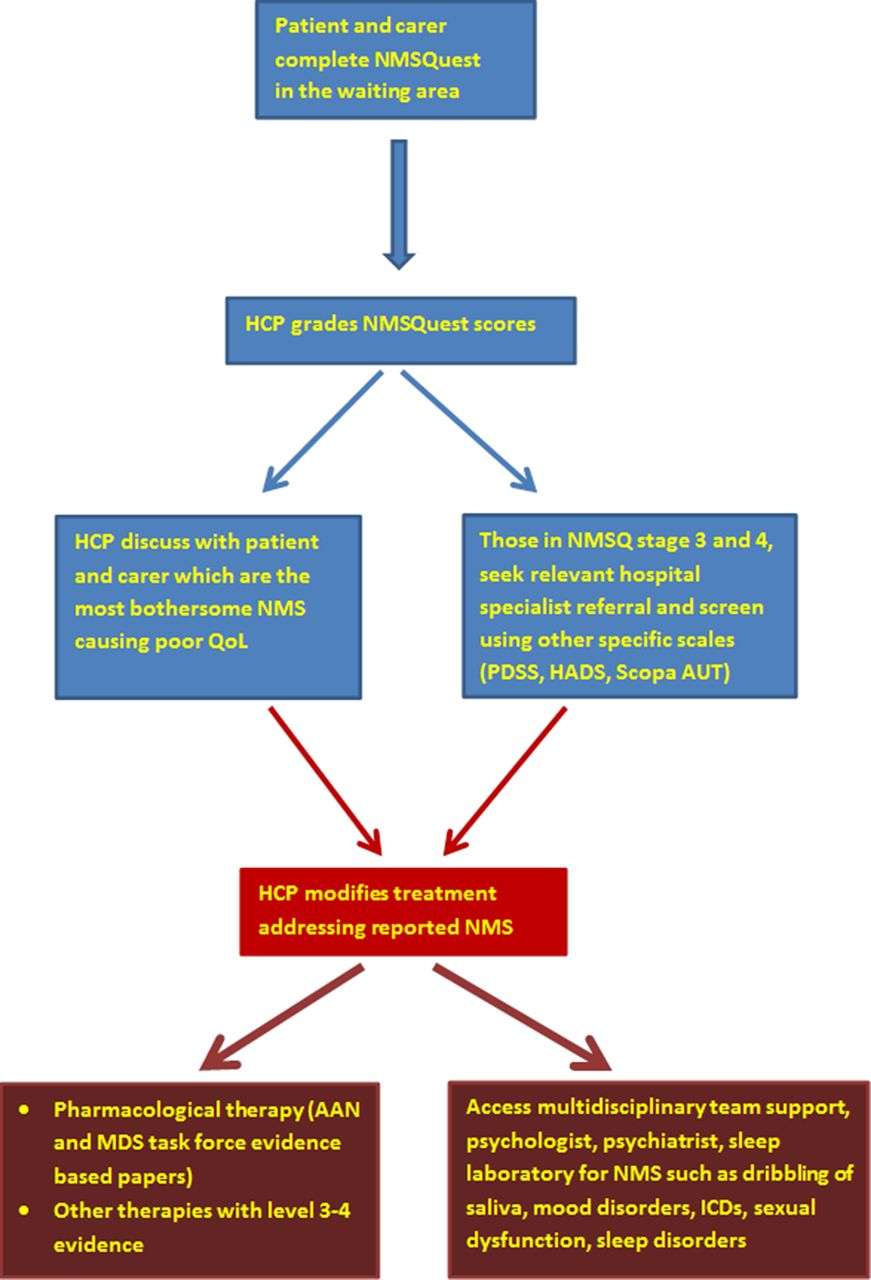
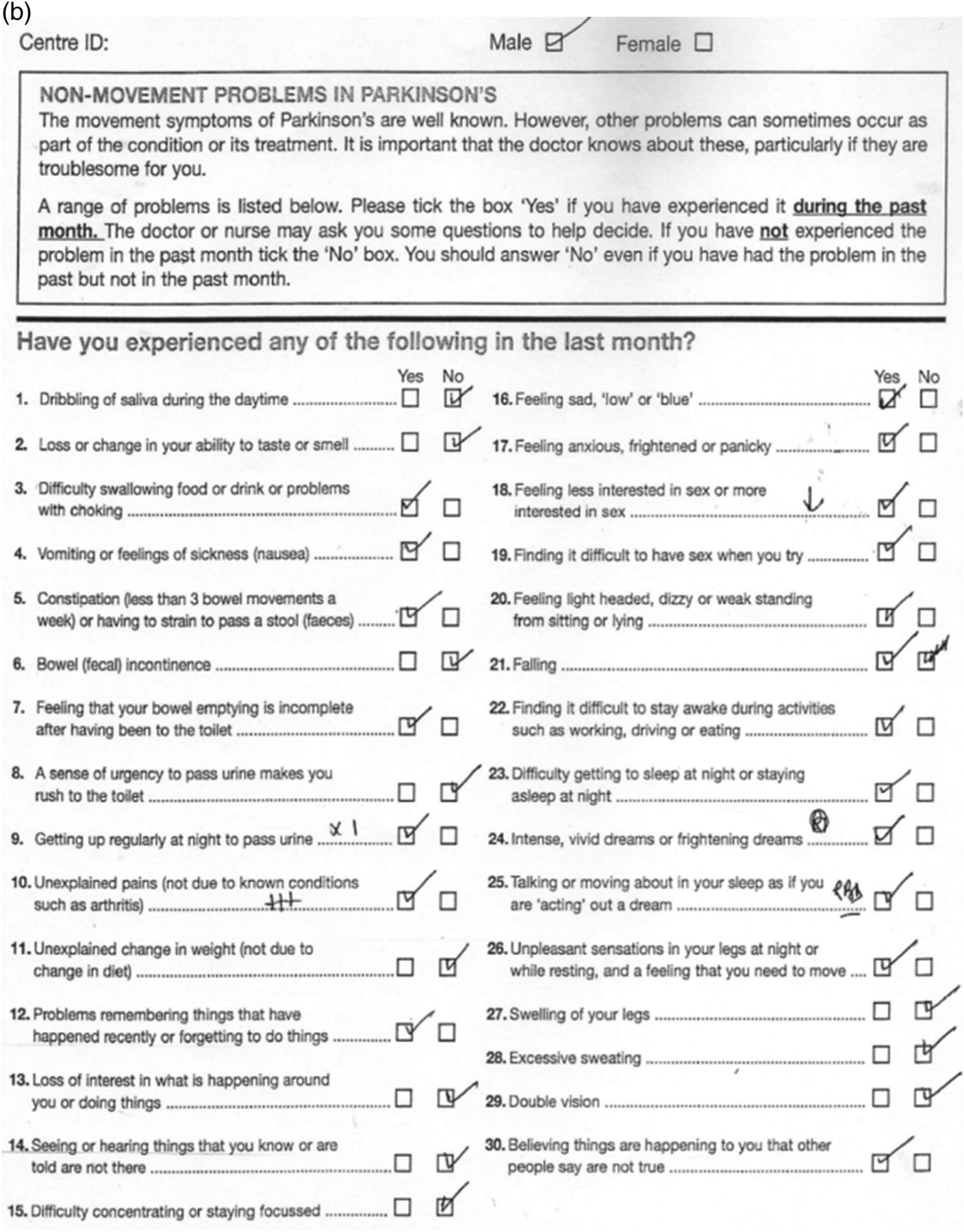
First, tools such as NMSQuest do not consume clinical interactions; the patient completes them and they help direct the consultation with nurse specialist or consultant. The clinician can then grade the non-motor symptoms burden numerically (box 2). Patients are then usually asked to flag the most bothersome symptoms. These are then addressed either through pharmacological, allied health specialist therapies, neuropsychological or neuropsychiatric input (figure 3). A yearly documentation of non-motor symptoms score helps to chart the progress of these symptoms. Pharmaceutical companies have developed and distributed alternative self-completed tools—such as the Parkinson well-being map—but have not been validated in PD. Figure 4 shows the importance of using such tools in the clinic. Two newly diagnosed patients, untreated and with similar motor disability, completed NMSQuests (figure 4A,B). The first patient reports only five non-motor symptoms: mainly problems with dribbling of saliva at night, urgency to pass urine, unexplained pain and dizziness. The second patient reports a wider range of non-motor symptoms (19/30): problems related to sleep, dribbling of saliva and other autonomic symptoms. Each of them needs a different management plan for their non-motor symptoms, as well as the treatment of the motor symptoms. These observations have been confirmed by two recent studies in untreated PD7 and early PD8 (compared with controls).
Non-motor Parkinson's disease burden grading using Non-Motor Symptoms Scale (NMSS) and Non-Motor Symptoms Questionnaire (NMSQ) (Kings ISCIII grading)
Kings-ISCIII grading by NMSQuest (can be performed by healthcare professional and based on patient responses using NMSQ)46
-
Stage 0 NMSQ—0 no non-motor symptoms
-
Stage 1 NMSQ—1–5 mild
-
Stage 2 NMSQ—6–12 moderate
-
Stage 3 NMSQ—13–20 severe
-
Stage 4 NMSQ—21–30 very severe
Grading by NMSS (to be used for clinical and research based studies)47
-
Non-motor symptoms burden level 0 NMSS—0
-
Non-motor symptoms burden level 1 NMSS—1–20
-
Non-motor symptoms burden level 2 NMSS—21–40
-
Non-motor symptoms burden level 3 NMSS—41–70
-
Non-motor symptoms burden level 4 NMSS—≥71

Suggested algorithm of addressing non-motor symptoms in clinic (modified from Chaudhuri et al).48 HCP, healthcare professional; QoL, quality of life; PDSS, Parkinson's Disease Sleep Scale; HADS, Hospital Anxiety and Depression Scale; Scopa AUT, Scales for Outcomes in Parkinson’s disease—Autonomic; ICD, impulse control disorders.
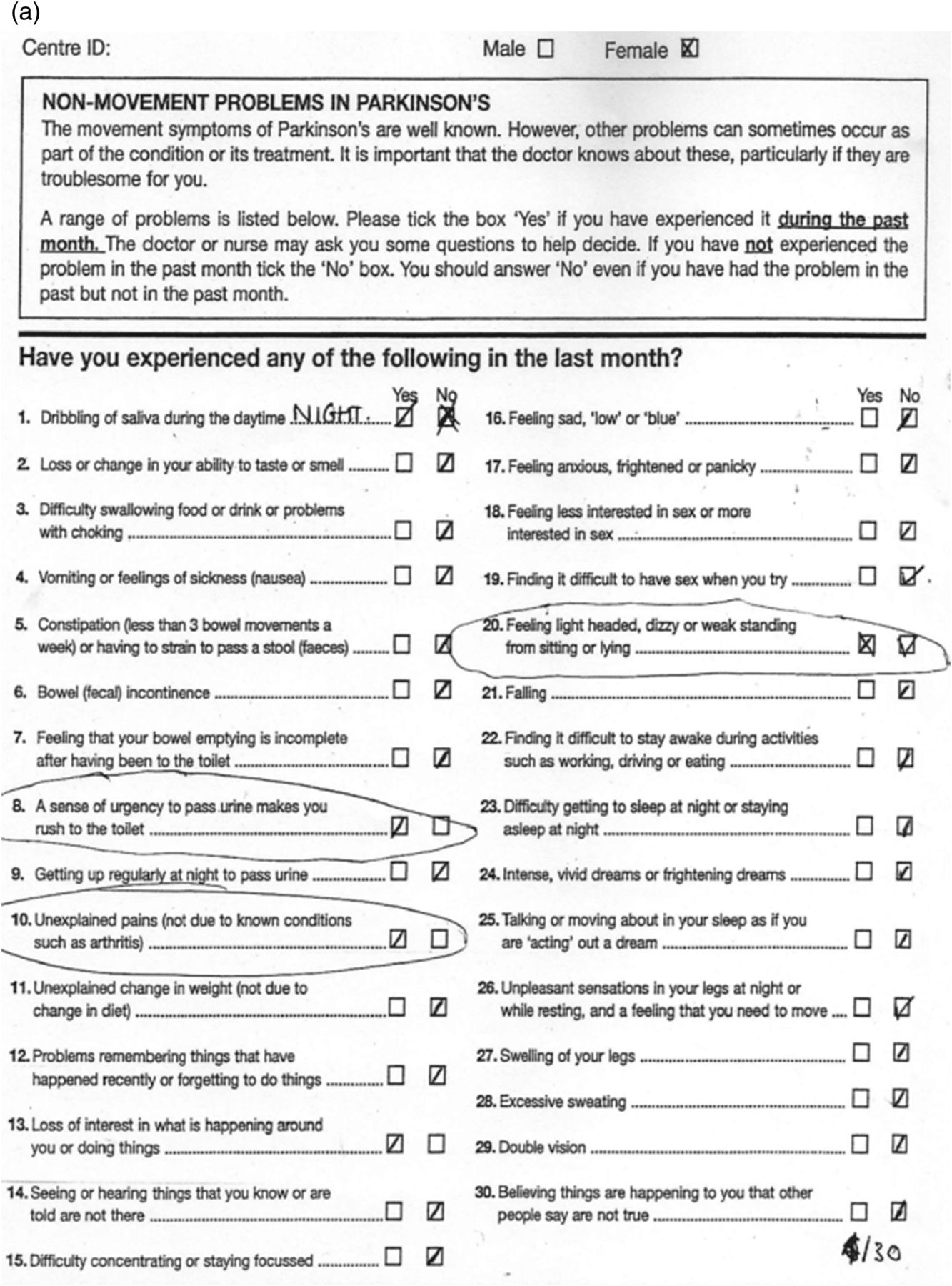
(A) Non-motor symptoms (NMS) Quest, drug-naïve patient, H&Y 1, 5/30.
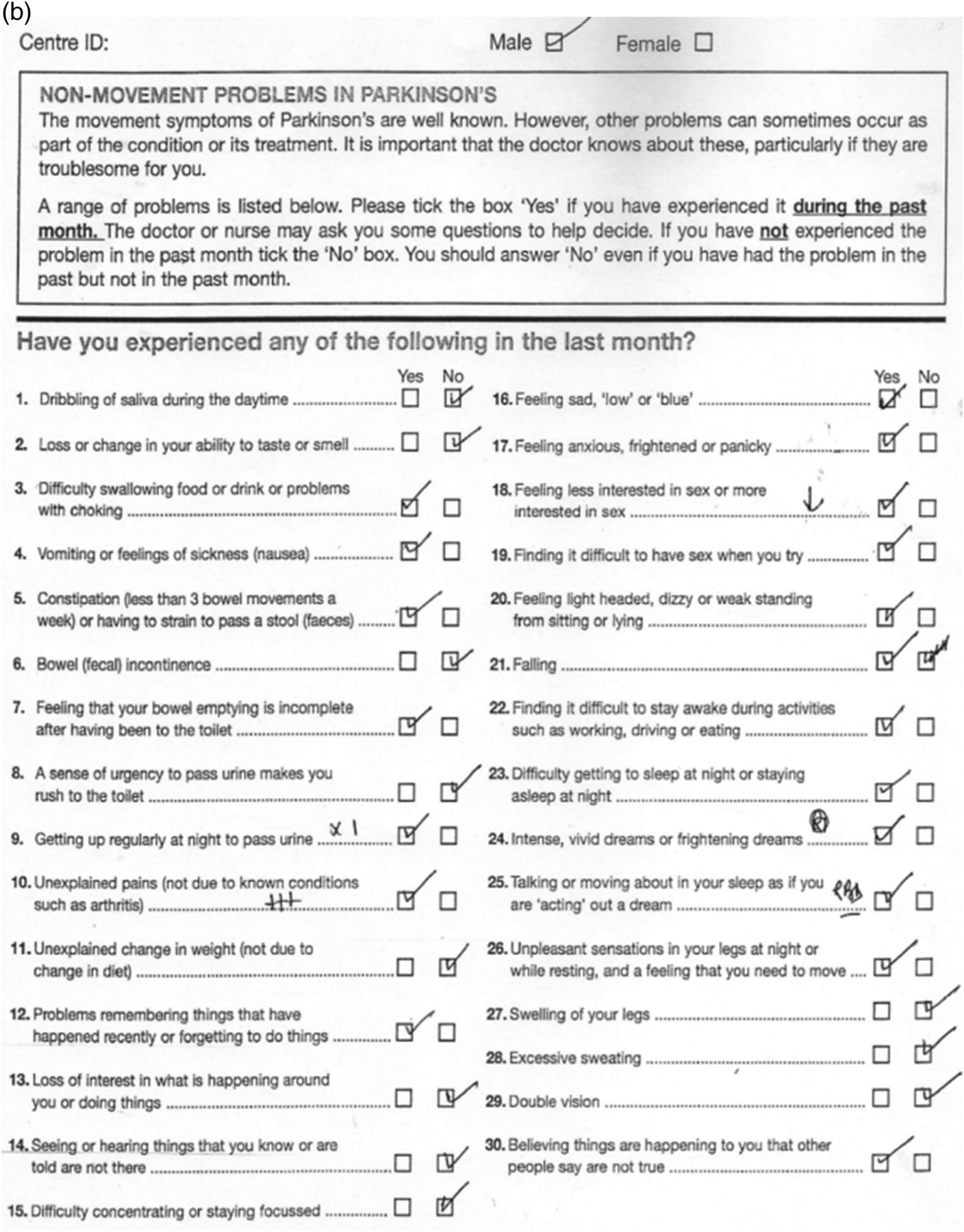
(B) NMS Quest, drug-naïve patient, H&Y 1, 19/30.
A simple grading using patient-completed NMSQuest has stages of severity burden of non-motor symptoms ranging between levels 1 and 4 (proposed as the Kings-ISCIII grading).46 This classification has been validated using the NMSS, the latter being particularly aimed towards research-based studies. NMSQ grading of the burden can influence treatment and screening in primary care is particularly recommended. For instance, for the patient cited in figure 4B, Hoehn and Yahr stage 1 would have NMSQ grade 4 and should be referred for treatment more promptly than the patient cited in figure 4A. Both NMSQ and NMSS burden grades have highly significant inverse correlations with HRQol of patients.47
Non-motor classification and subtypes
The classification based on NMSS has also given rise to the growing concept of non-motor dominant subtypes within PD. Just as in multiple sclerosis and motor neurone disease, clinical subtyping in PD is important (although some argue against this). Subtyping helps give a clearer definition of the clinical symptoms of PD as well as helping with inclusion criteria of patients for clinical trials. It also makes sense given the heterogeneity of neuropathological process underlying PD.
The groups of motor subtypes of PD include
-
tremor dominant
-
akinetic dominant
-
postural instability and gait disturbances
-
mixed.
Based on the dichotomy between non-motor symptom scores and motor scores in PD, non-motor classification of PD has been proposed, with five levels of non-motor symptoms burden47 (box 2), as well as non-motor subtyping.47 A recent study identified four distinct clusters within PD: two were non-motor-dominant and benign mixed motor/non-motor (with prominent clinical expression of non-motor symptoms); the other two groups were motor-dominant and benign pure motor.16 We have proposed specific PD subtypes based on the predominance of key symptoms relevant to the early stage of PD; in the advanced stages, many of these subtypes may merge, as with motor subtypes.47 However, the natural history of these proposed subtypes at the moment remains unknown.
Evidence that non-motor symptoms are a key determinant of quality of life
Several studies have shown that the non-motor symptoms burden is a key determinant of quality of life of PD and carers.42 ,49 Patient-related questionnaires also show a growing awareness that these symptoms need addressing since they may adversely affect the lives of patient and carer. Improvement in non-motor symptoms, particularly the dopaminergic therapy-responsive symptoms, translates to robust improvements in quality of life.50 ,51
Non-motor fluctuation in PD
Apart from motor fluctuation, patients with PD also experience ‘non-motor fluctuations’,52 ,53 which often develop in tandem with motor fluctuations. Some non-motor symptoms are accentuated during ‘off’ periods while others occur only in ‘off’ periods (below).
Non-motor symptoms that worsen during ‘off’ periods
-
fatigue
-
depression
-
anxiety
-
inner restlessness
-
impaired concentration/attention.
Non-motor symptoms occurring only/exclusively during ‘off’ periods
-
fatigue
-
depression
-
anxiety
-
impaired concentration
-
inner restlessness.
Anxiety, depression, fatigue and pain had a negative impact on health-related quality of life.52
Treatment
There are diverse treatments to address non-motor symptoms in PD. Both the American Academy of Neurology and the Movement Disorders Society have issued task force documents for managing non-motor symptoms in PD.54 ,55 Also, several open-label or comparative studies have addressed the effect of advanced therapies in PD on non-motor symptoms (apomorphine, intrajejunal levodopa infusion and rotigotine transdermal patch).56–58 However, the evidence base is poor, with few level 1 studies supporting any specific therapy. However, there was a recent randomised double-blind controlled study providing class I evidence that paroxetine and venlafaxine XR treat depression effectively in PD.59 A few randomised clinical trials have addressed key non-motor symptoms in PD, such as pain (oxycodone with naloxone: the PANDA study) and excessive daytime sleepiness (caffeine, pitolisant, adenosine receptor antagonists). Several novel non-dopaminergic targets using non-dopaminergic agents have been described for managing some motor (mainly dyskinesias) and non-motor (excessive daytime sleepiness, pain, constipation, depression and cognition) symptoms (table 5). At present, these remain investigational.60 We still await robust evidence for treatment of non-motor symptoms in PD; this remains a key unmet need.
Treatment suggestions for some non-motor symptoms
For some non-motor symptoms, such as anxiety, depression, pain and fatigue, clinicians must ascertain as far as possible whether these are part of non-motor fluctuations. If so, and if they are exclusively present in the ‘off’ period, then treatment may need to focus on alleviation of motor ‘off’ period with relevant anti-parkinsonian medication, rather than using antidepressants or antianxiety medications.
Multidisciplinary support
For symptoms such as dribbling of saliva, pain, sexual dysfunction, impulse control disorders and cognitive impairment, it is important and ideal to have the participation of a multidisciplinary team comprising PD nurse specialist, speech and language therapist, physiotherapist, occupational therapist, clinical psychologist and neuropsychiatrist. Speech and language therapy input in cases with disabling or severe dribbling of saliva is essential, for advice on swallow timers and head positioning. Experienced input from psychology and neuropsychiatry and a PD nurse specialist are essential in cases for managing severe depression, anxiety disorders and impulse control disorders. We also recommend, where possible, joint working with a member of the care of the elderly team with a special interest in PD with good access to multidisciplinary team support.
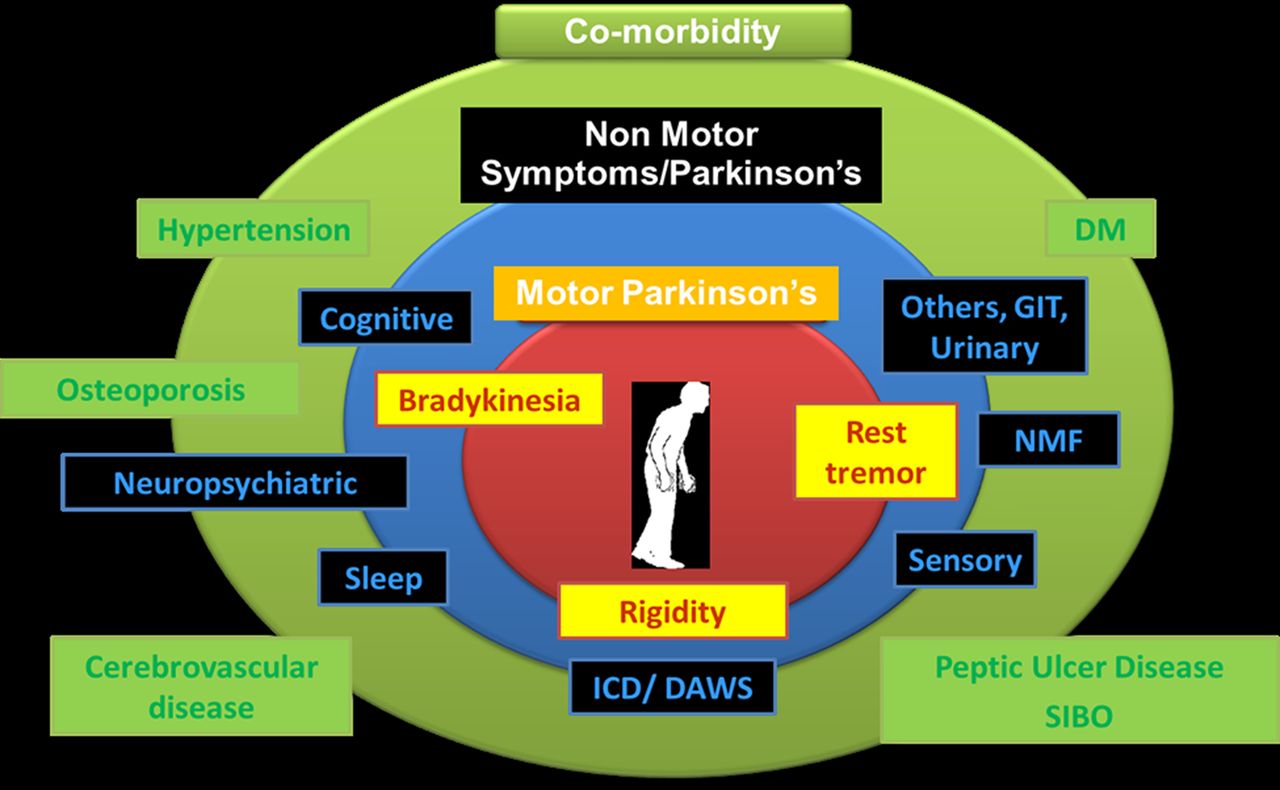
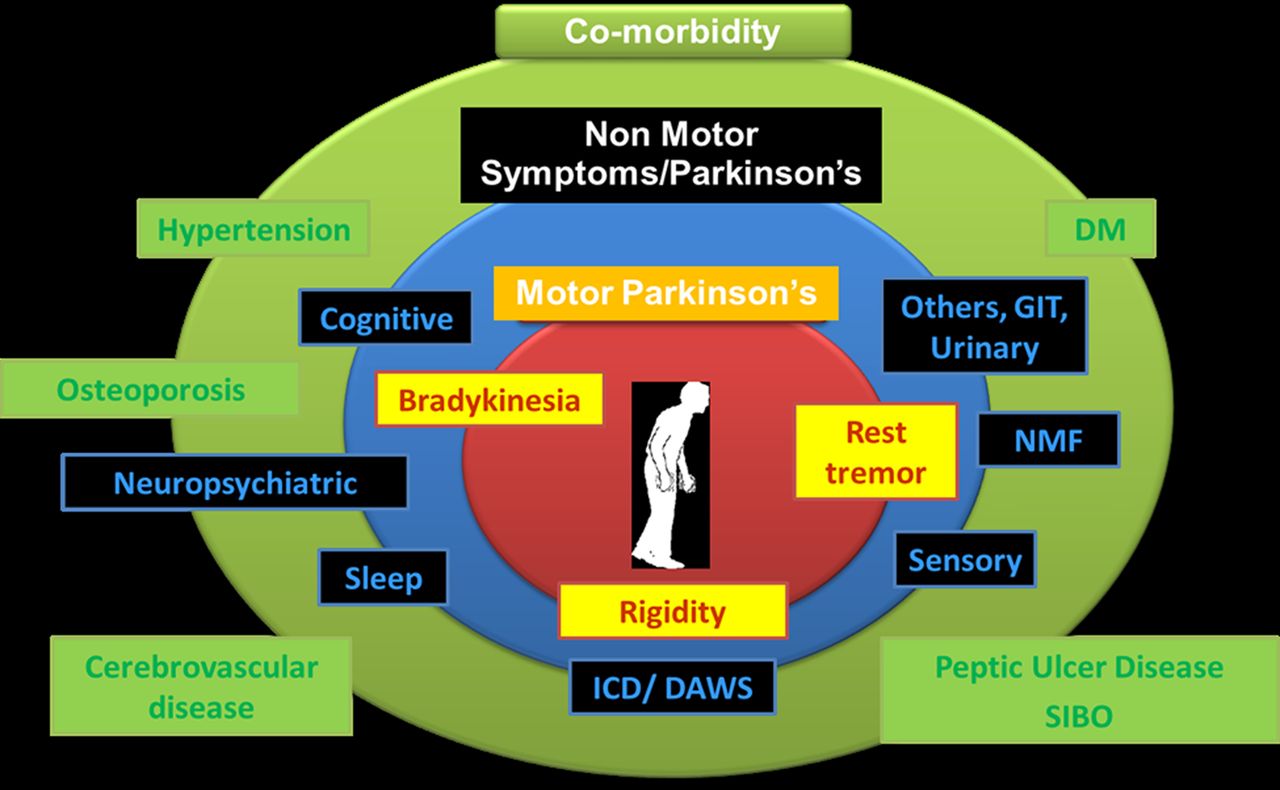
There is also increasing evidence suggesting that treating comorbidities, such as hypertension, diabetes mellitus, peptic ulcer disease, small intestinal bacterial overgrowth and osteoporosis, can ensure a complete treatment package for PD, in addition to monitoring for and managing drug-induced non-motor symptoms and non-motor syndromes (figure 5).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
The spectrum of the multimorbid Parkinson's disease. GIT, gastrointestinal; NMF, non-motor fluctuation; DM, diabetes mellitus; SIBO, small intestinal bacterial overgrowth; ICD, impulse control disorders; DAWS, dopamine agonist withdrawal syndrome.
The future and conclusions
Non-motor symptoms represent a huge challenge to the treating physicians and allied health colleagues and continue to be a key determinant of patients’ and carers’ quality of life at huge societal costs. Their diversity, their differential effects on quality of life and their possible progression patterns pose additional challenges. We need much more research to recognise and manage non-motor symptoms effectively in clinical practice.
Future biomarkers will probably define the premotor stages of PD as well as the clinical patterns of PD into specific endophenotypes. Classifications have hitherto focused on motor subtypes but will include specific non-motor subtypes with the potential for specific treatments. Extension of non-motor symptoms-based studies will also address hitherto unaddressed issues, such as the influence of ethnicity, and poorly explored issues, such as influence of genetics.
Greater awareness of non-motor PD symptoms and the development of validated rating scales have led to major advances in understanding their evolution and progression; experimental models to explore their pathogenesis and potential treatments have lagged behind. There are now opportunities using existing dopaminergic animal models, some of which are now gathering momentum but others, such as the investigation of dopamine dysregulation syndromes/compulsive behaviours and dopamine agonist withdrawal syndromes, are in their infancy. What would really help is a major push to solve the role of non-dopaminergic degenerative changes in the evolution of non-motor symptoms in PD. This is perfectly feasible as there are well-established tools to do this (eg, lesioning, toxin treatment), but so far there is no momentum for this.
Acknowledgments
This paper presents independent research funded by the National Institute for Health Research (NIHR) Mental Health Biomedical Research Centre and Dementia Unit at South London and Maudsley NHS Foundation Trust and King's College London. We acknowledge the help and support of the international Parkinson's non-motor group and in particular Professor Pablo Martinez-Martin and his team in the Institute of Neuroepidemiology, Madrid, for co-leading all studies related to NMSQuest and NMSS described in this paper. NMSQuest can be downloaded from the websites of the following: Parkinson's UK: NMSQuest: (http://www.parkinsons.org.uk/PDF/nms_questionnaire.pdf), The Movement Disorders Society: (http://www.movementdisorders.org/publications/rating_scales/). European Parkinson's Disease Association. Life With Parkinson's: (http://www.epda.eu.com/en/parkinsons/life-with-parkinsons/part-2/introduction/).
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Contributors KRC conceived the idea of the paper. The first draft was prepared by KRC, PJ and AT, and then circulated repeatedly among all authors for critical revision. AT produced the tables and figures and formatted the manuscript according to the requirements.
-
Funding Aspects of research described in the review (NMSQuest studies, PD endophenotyping) have been supported by NIHR Biomedical Research Centre grants to Kings College, London.
-
Competing interests None.
-
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Simon Lewis, Sydney, Australia, and by Nick Fletcher, Liverpool, UK.
Linked Articles
- Editors' choice
Other content recommended for you
- Baseline prevalence and longitudinal evolution of non-motor symptoms in early Parkinson’s disease: the PPMI cohort
- ON/OFF non-motor evaluation: a new way to evaluate non-motor fluctuations in Parkinson’s disease
- Open questions on the nature of Parkinson’s disease: from triggers to spreading pathology
- Predictors of short-term impulsive and compulsive behaviour after subthalamic stimulation in Parkinson disease
- ICARUS study: prevalence and clinical features of impulse control disorders in Parkinson’s disease
- Impact of sleep-related symptoms on clinical motor subtypes and disability in Parkinson’s disease: a multicentre cross-sectional study
- Neuroendocrine abnormalities in Parkinson's disease
- Efficacy of acupuncture (Jin’s three-needle) on motor symptoms and anxiety in patients with Parkinson’s disease: protocol for a multicentre, randomised, assessor-blinded clinical trial
- A prospective, controlled study of non-motor effects of subthalamic stimulation in Parkinson’s disease: results at the 36-month follow-up
- Parkinson’s disease: etiopathogenesis and treatment