Article Text

Statistics from Altmetric.com
Introduction
Acute relapses in multiple sclerosis (MS) represent foci of acute inflammation and demyelination within clinically eloquent areas of the central nervous system (CNS).1 It is important to recognise and to assess people with MS relapses to establish their clinical diagnosis,2 optimise short-term ability,3 guide longer-term treatment decisions4 and inform on the natural history of disease.5 Historically, neurology services have been poorly organised to meet the needs of patients with an acute deterioration in MS symptoms. However, a dedicated service for patients with symptoms suggesting MS relapse shortens the delay in accessing specialist care and receiving treatment, reduces inpatient admissions and minimises the psychological impact of MS relapses.6 As a result, UK national recommendations now suggest that patients experiencing relapse should have rapid access to outpatient specialist MS care.7–9 Thus many specialist centres have developed open, rapid-access services that may vary in design, but which allow people with MS and acute neurological dysfunction to receive prompt expert assessment.
Service model considerations
In a typical rapid-access service model, patients self-refer; however, the service should also incorporate referrals from multiple sources, including general practitioners and hospital subspecialties (figure 1). Patients need signposting to self-referral routes at the time of their diagnosis, and reinforcing at subsequent points of contact. Methods of informing patients or general practitioners about referral routes include verbal or written reminders (eg, leaflet) provided at specialist clinic appointments, adding emergency contact details to the standard clinic letter header, or including emergency MS contact details within the hospital website. Referral routes might include telephone, text message or email, checked each working day. Telephone triage can efficiently deal with referrals promptly and identify those patients who might be best served by a face-to-face evaluation. Patient calls are best returned by an MS specialist nurse or an appropriately experienced clinician in order to plan management (box 1). Because of the wide range of symptoms reported within such a system, it is also worth considering at an early stage whether the service will be dedicated only to patients with symptoms suggesting a relapse or open to other uses. These might include acute symptom control problems, medication side effects, review during pregnancy or for timely conception and pregnancy planning advice. Depending on details acquired from telephone triage, patients could either be invited to attend a rapid-access MS appointment, be offered a telemedicine option or be referred to an alternative service.

Suggested algorithm for managing patients with acute symptoms of multiple sclerosis (MS).
Aims of the telephone consultation in multiple sclerosis relapse
Establish the clinical history
Review the impact of new symptoms on the patient and their family
Assess any medical or psychological comorbidity
Determine the medication history including previous corticosteroid use
Check the patient's ability to attend for outpatient review
Patients invited to attend a specialist MS appointment may visit either a dedicated rapid-access clinic, a routine clinic with rapid-access capacity, or a ward with facilities for day-case assessment or via a telemedicine. Telemedicine or telecare uses information or communication technology to provide clinical care.10 Telemedicine can adopt several formats; perhaps the simplest and most applicable in this context is the telephone consultation. Alternatively, video consultations can be run using a patient's own computer/smart-device or by using clinic space in a local health centre with videoconferencing facilities. Telephone or video consultations may be well suited to patients who are less able to attend hospital, due to geographical or disease factors, or who do not need to be reviewed in person, for example, mild sensory symptoms, resolving symptoms, medication queries or pregnancy or conception counselling.
The rapid-access consultation may be led by one of several personnel including a specialist MS nurse, neurology consultant or neurology trainee. MS specialist nurses can offer continuity of outpatient and community care and provide detailed personal knowledge of individual patients. Several factors suggest that the clinic should be overseen by an individual clinician with expertise in MS: these include the practical challenge of accurately diagnosing an MS relapse,11 the wide ranging differential diagnosis encountered in the clinic,12 the need to prescribe acute treatment and potentially the need to make modifications to longer-term treatment.6
A physiotherapist or occupational therapist in the rapid-access setting allows such acute interventions as falls risk assessment and provision of walking aids or equipment, increases the rate of onward referral within their discipline12 and promotes interdisciplinary learning within the MS team. We have found that around a quarter of patients are referred for ongoing therapy intervention following rapid-access clinic (including physio- occupational, speech or continence therapy).12 However, the value of having a therapist in clinic must be weighed up against the cost to the service and disinvestment in other duties. An alternative model, working well in other centres, is rapid access to multidisciplinary neurorehabilitation service for the assessment of newly acquired disability.
Relapse rates vary according to season,13 with peaks in early winter and summer; thus rapid-access clinic demand may fluctuate throughout the year and capacity should allow for this. Clinicians require adequate time to cover the wide range of issues arising in the context of an acute deterioration in MS (see below); our own rapid access has 40-min clinic slots. Our experience suggests that approximately 27 people per 100 000 use the rapid-access MS service annually, averaging 1.2 occasions each. The capacity of any planned service could be geared accordingly.
Considerations during the clinic
History
Detailed history taking during the clinic serves several aims, the main one usually being to establish the cause of the acute deterioration. There has been much work to refine the definition of a clinical relapse in MS, largely to facilitate objective outcome measures during MS treatment trials. The most recent consensus definition of an MS relapse is ‘patient-reported symptoms and/or objectively observed signs typical of an acute inflammatory demyelinating event in the CNS, current or historical, with duration of at least 24 h’.2 In reality, the accurate diagnosis of MS relapses may be obscured by pre-existing deficits, disease progression, psychosocial influences and short-term factors including infection and heat. The recognition of new symptoms during a period of stability helps to rule out secondary progression but there is not always an available reliable assessment of baseline function. Similarly, patients often develop sequential symptoms in different neurological systems. Some clinical trial protocols consider sequential symptoms that occur within 30 days of each other to constitute a single polysymptomatic relapse, but this system may falsely reduce multiple discrete inflammatory events into a single clinical attack.11 Some clinical trials require objective confirmation of reported symptoms, including changes in the Expanded Disability Status Scale (EDSS) or the Kurtzke Functional System Scores;14 however, this also probably underestimates the relapse rate since: for example, relapses predominantly affecting cognition would be under-recognised.15 Strict definitions of relapse also do not capture patients who have multiple minor, short-lived new symptoms with very active MR scans. It is challenging to distinguish transient neurological deteriorations arising in the context of fever (pseudorelapses) from genuine relapses caused by concurrent infection; this may be possible only retrospectively, after treating infective symptoms.
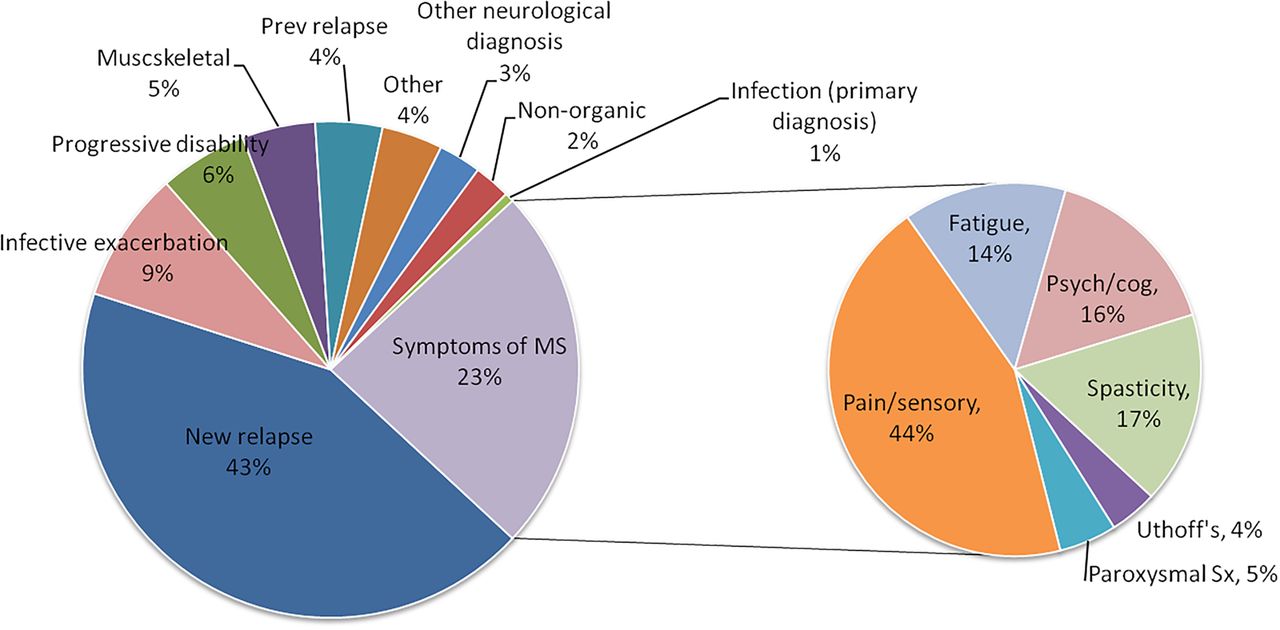
Most (58%) rapid-access clinic presentations are new relapses but non-relapse symptoms of MS include pain, spasticity, cognitive symptoms or fatigue; common differential diagnoses are progressive disability and infective exacerbations of pre-existing symptoms (figure 2). A significant minority of presentations arise from conditions other than MS, for example, musculoskeletal conditions, other neurological conditions such as migraine, ophthalmological conditions or medical conditions such as thyrotoxicosis.12
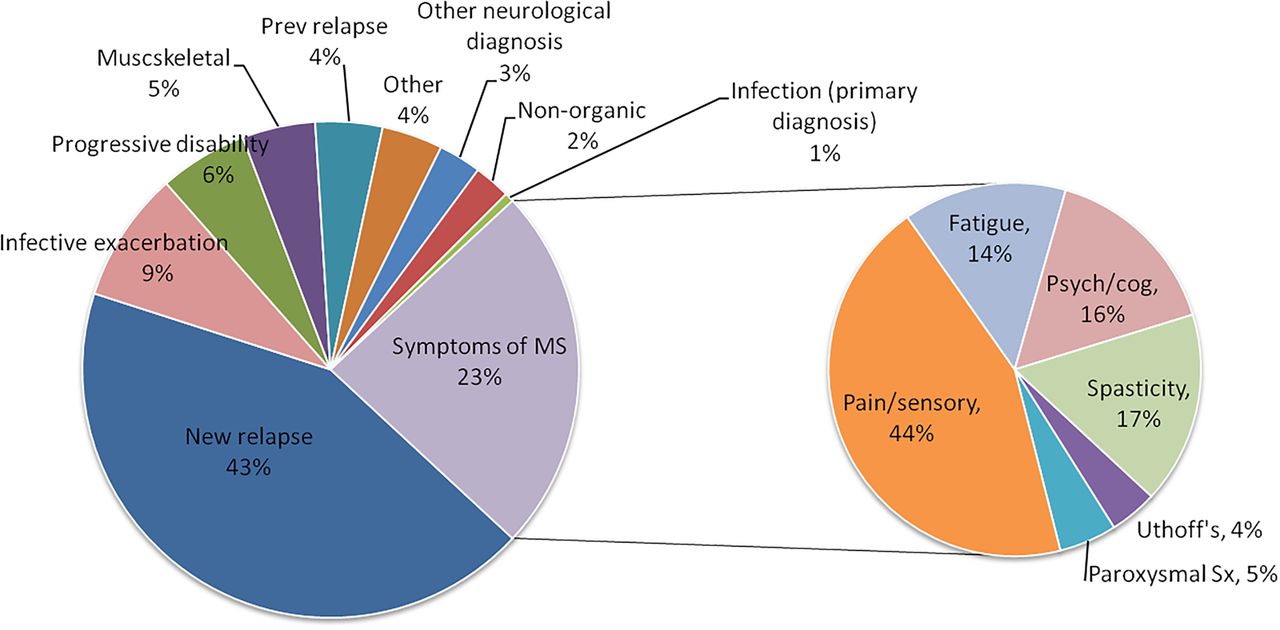
Differential diagnoses of 371 sequential patients, triaged for the presence of symptoms suggesting relapse, attending the University Hospital of Wales rapid-access multiple sclerosis (MS) Clinic during 2010–2013.
As well as diagnosing the cause of acute deterioration, it is important to explore the impact of new symptoms on daily function, employment,16 financial status and psychological well-being.17 In combination with a review of the services currently accessed by the patient in the community, this information can usefully guide appropriate intervention. A thorough medication history is useful to determine the timing and effect of previous courses of corticosteroids and the impact of current or previous symptomatic or disease-modifying therapy. Comorbid health problems should be explored, especially coexisting depression, alcohol excess or non-steroidal anti-inflammatory use, all of which are relative contraindications to high-dose corticosteroids.9 The history can also uncover covert symptoms of fatigue, continence problems or cognitive dysfunction.
Examination
Examination in the relapse clinic aims to clarify the presence and nature of any neurological deficit and to clarify the location of a relapse; most commonly the optic nerve, brainstem or spinal cord or, rarely, multifocal.2 Furthermore, examination allows detection of important neurological differential diagnoses, including neurological conditions such as functional disorder, musculoskeletal problems such as trochanteric bursitis, ophthalmological conditions including cataracts or uveitis and general medical conditions such as deep vein thrombosis. Examination also helps to guide appropriate interventions, for example, the degree of spasticity, and provides the opportunity for objective baseline measures to be recorded, against which to assess subsequent recovery (eg, visual acuity, MRC strength grade, 10 m timed walk, maximum walking distance and/or nine-hole peg test). Multidisciplinary support within the clinic can facilitate recording of some of these useful measures within the time available.
Clinical data collection
The general move towards developing innovative information technology services to benefit patients and clinicians is reflected in the recent national healthcare strategy in England.18 Considerations about clinical data collection are particularly relevant to MS rapid-access services. The assessment and management of patients presenting with an acute deterioration may be complicated by the limited availability of medical records at short notice. Such records are valuable in confirming diagnosis, reviewing investigation results, noting prior medication use and assessing the relapse history, potentially identifying patients needing different a different disease-modifying therapy. Systematic collection of clinical data can help to build a temporal map of each person's disease course (figure 3) and, on a population level, can generate valuable information on epidemiology and service delivery, support recruitment to research studies and influence local service design.
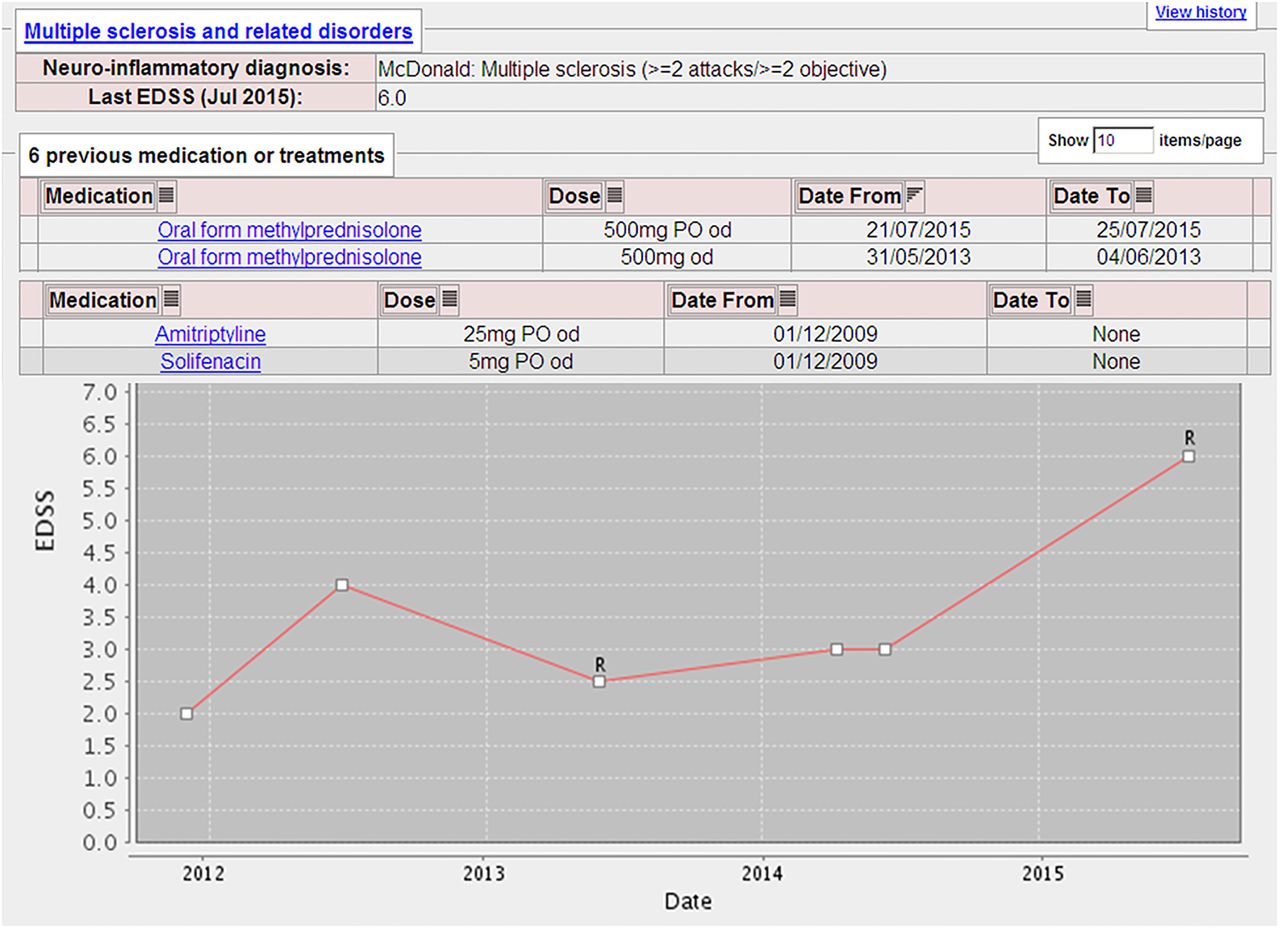
Personalised e-medicine: a screen-shot from the South Wales Registry web-based software showing prospectively acquired clinical data from a patient with relapsing–remitting multiple sclerosis. EDSS, expanded disability status scale.
Some MS services with sufficient resources use electronic databases to address these issues but data input can be time-consuming. Others favour a standardised symptom questionnaire to capture the broad range of patients’ symptoms.19 This can be administered while patients are waiting to be seen and serve to focus what can otherwise be a time-consuming consultation. The use of mobile computing technologies is increasingly adding value to healthcare.20 Smart mobile devices such as tablets can now be used in this context, either remotely or in the waiting room, to collect patient-derived data on symptoms and their impact prior to consultation in the rapid-access clinic. This method carries the advantage that data could be readily uploaded to a local or national MS patient database.
Management
Key interventions in the rapid-access setting include patient education about the nature of relapses, treatment to accelerate recovery and also social support, therapy and equipment that may allow the patient to adapt to their acute neurological disability. Useful resources for patient-education about the acute symptoms of MS include the MS Trust21 and MS Society22 webpages.
Corticosteroids
Conventional management of MS relapse includes high-dose corticosteroids, which shorten the duration of symptoms but do not influence longer-term outcome.3 Current guidance from the UK National Institute for Health and Care Excellence (NICE) recommends treating patients who have an MS relapse sufficient to limit their ability to perform their usual activities.7 There is still uncertainty over the optimal dose and route of corticosteroid administration. Oral low-dose corticosteroids were ineffective during the Optic Neuritis Treatment Trial but high-dose oral methylprednisolone (500 mg per day for 5 days) significantly reduced the short-term disability associated with acute demyelinating events.23 ,24 The most recent Cochrane review suggested oral and intravenous high-dose corticosteroids have equivalent efficacy on short-term disability and imaging outcomes following an MS relapse but there is no consensus for the corticosteroid dose and regimen.25 A subsequent randomised controlled trial confirmed non-inferiority of oral methylprednisolone 1.25 g per day for 3 days compared with intravenous methylprednisolone 1 g/day for 3 days.26 There are two further head-to-head comparisons underway of oral versus intravenous corticosteroid for MS relapses: the Oral Megadose Corticosteroid Therapy of Acute Exacerbations of Multiple Sclerosis trial and the Efficacy and Safety of Methylprednisolone Per os Versus intravenous for the Treatment of MS Relapses trial.
Oral corticosteroids have the advantages of being more convenient for patients, less expensive and less demanding of healthcare resources. However, intravenous corticosteroids can be safely given in the home setting, reducing cost and improving patients’ experience of relapse management compared with treatment in hospital.27 Current NICE guidelines recommend treating acute relapses of MS with oral methylprednisolone 500 mg daily for 5 days and reserving intravenous methylprednisolone 1 g daily for 3–5 days for patients who have not tolerated or responded to oral methylprednisolone or those who require admission to hospital.
Patients receiving high-dose corticosteroids require counselling about the common side effects, including headache, mood disturbance, gastrointestinal upset, fatigue, insomnia, metallic taste and rash.26 Although pulsed methylprednisolone probably does not increase the risk of osteoporosis,28 it is worth considering the rare but serious complication of avascular osteonecrosis. The overall risk of this in patients receiving corticosteroid treatment is 3–25%.29 The risk varies with underlying disease and dosing regimen. Two large series documenting pulsed corticosteroid use in MS suggested that the short-term risk of symptomatic avascular osteonecrosis is less than 1%.30 ,31 However, the risk appears to be cumulative; a separate study found MRI evidence of avascular osteonecrosis in up to 15% of patients with MS who had frequent courses of pulsed corticosteroids.32 Patients with a clinical history of indigestion or peptic ulcer disease may benefit from a short course of proton-pump inhibitor, although the risk of peptic ulcer disease from corticosteroids is probably negligible unless the patient also takes non-steroidal anti-inflammatory drugs.33 ,34 Clinicians should also be cautious when treating patients with diabetes mellitus, hypertension and those with coexisting infection. There is no evidence regarding the most appropriate means to screen for infection,35 but guidance suggests that patients with MS relapse should have body temperature and urine dipstick routinely checked.9 Patients with symptoms of infection need a more focused examination and investigations and in most cases, their infection should be treated before they start corticosteroids. There is useful guidance for administering corticosteroids in patients with an isolated positive urine dipstick.36
Other interventions
Patients often need other symptomatic medications during a relapse, in addition to corticosteroids; recent guidance summarises the evidence-based treatments available for a wide range of MS symptoms.7 There is evidence that multidisciplinary therapy interventions improve short-term recovery from relapse,37 and improves the outcome of patients with incomplete recovery from relapses who have accumulated moderate-to-severe disability.38 Our experience indicates that 70% of patients with non-relapse related MS presentations receive either a medication change or a referral for therapy during their consultation.12 Having a physiotherapist and occupational therapist in the rapid-access clinic setting facilitates the use of brief interventions such as provision of a walking aid, prescribing exercises or providing advice on fatigue management, employment, financial aid or local therapy services. Therapists can make onward referrals, including to outpatient physiotherapy, group exercise or fatigue management classes, home or work visits and referrals to continence or orthotic services.
The relapse clinic also provides an opportunity to consider the indication for a disease-modifying therapy; either offering written information in preparation for starting this in the future, or prompting a discussion about switching, omitting or stopping an existing disease-modifying therapy. This discussion may start in the rapid-access clinic (either by patient or clinician), or be deferred until the follow-up MS clinic appointment, depending on expertise and to allow time for recovery, deliberation and any informative investigations.
Investigations
The diagnosis of relapse is largely clinical but clinicians often request investigations to explore differential diagnoses including infection, or to guide subsequent decisions about disease-modifying therapy. For example, NICE guidance (in the UK) stipulates MRI criteria for prescribing natalizumab (evidence of gadolinium enhancement or a significant increase in T2 lesion load on an MRI brain scan).4 Some clinicians choose to combine imaging data with clinical information to look for the overall level of inflammatory activity to guide treatment or measure its effect.39 In patients where there is a planned change in disease-modifying therapy, pretreatment investigations such as blood tests, ECG or optical coherence tomography can be requested from the rapid-access clinic.
Prognostic counselling
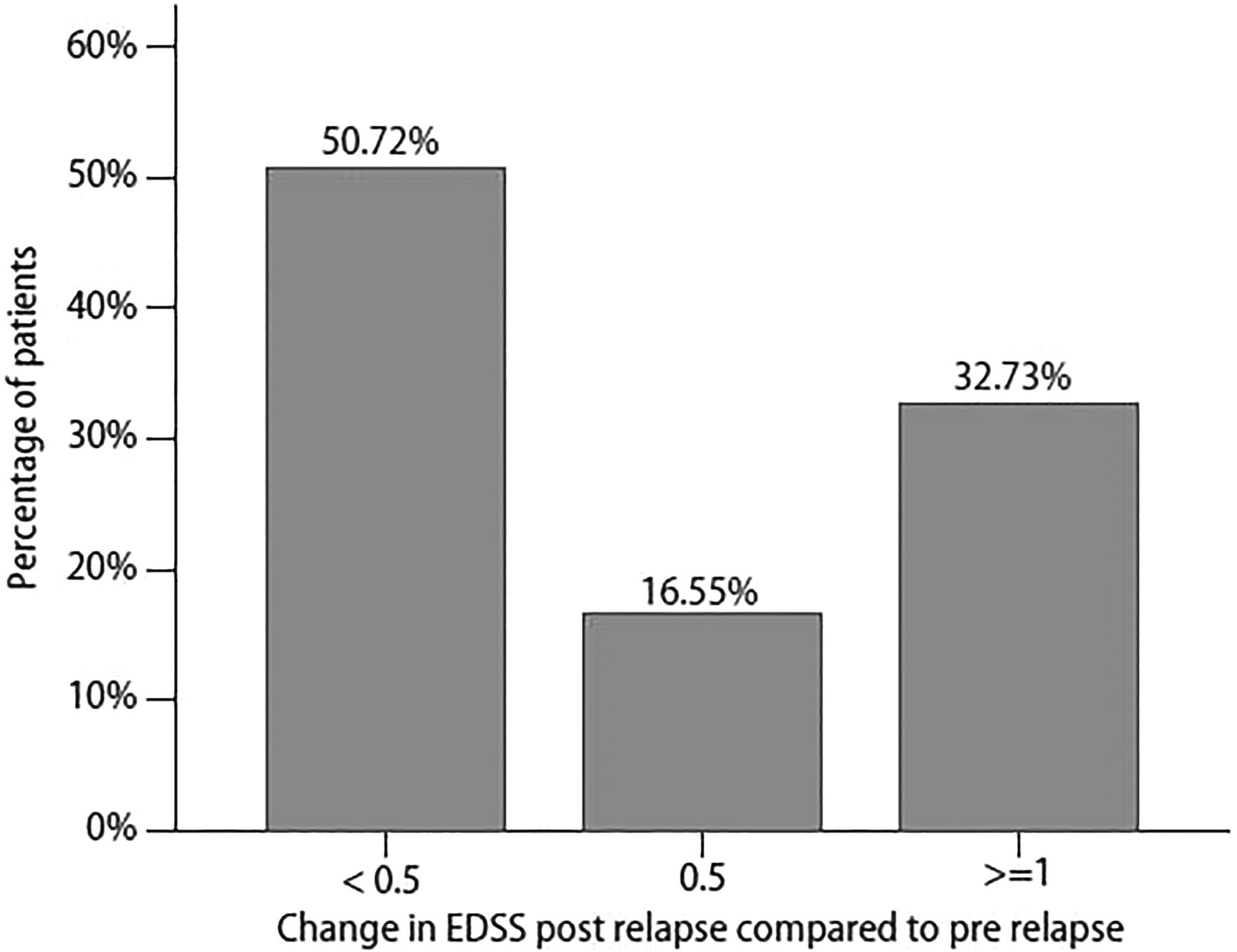
A further role of the rapid-access consultation is to offer prognostic information to patients in relapse. Most patients experience an increase in disability during an MS relapse that is measurable as a change in EDSS score, with a mean deterioration of 1.45 EDSS points. However, half of them fully regain their function (figure 4). In those who do accrue permanent disability as the result of a relapse, two-thirds develop residual disability ≥1 EDSS point above their baseline. The recovery from relapse does not seem to be predicted by age, sex, site of relapse or previous use of disease-modifying therapy. However, someone with a highly disabling relapse is likely to accrue a higher level of residual disability as a result.5

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Residual change in Expanded Disability Status Scale (EDSS) score post relapse. (Adapted from Hirst et al5).
Follow-up
Patients diagnosed with a new relapse in rapid-access clinic should be actively followed up in order to determine and record their extent of recovery and to consider further treatment interventions. There is evidence that most recovery from relapse-related disability occurs within 2 months.40 Follow-up at 2 months therefore allows identification of patients with incomplete recovery from relapse who may benefit from further intervention,38 ,41 ,42 and is timed appropriately to review patients who have recovered for alterations to their longer-term treatment plan. Follow-up may be by telephone consultation in the first instance if clinic waiting lists are prohibitive. Patients with coexisting infection require particular consideration, as infection-associated relapses appear more severe and sustained.43 ,44 Patients needing treatment of an underlying infection with antimicrobial treatment should be followed up afterwards in order to identify persistent neurological disability that may need subsequent corticosteroid treatment (figure 1).
Pitfalls
Self-referral of patients could expose the clinic to overuse by certain patients but this has not been our experience. In fact, the uptake of the rapid-access services in the case of suspected relapse seems lower than expected in our population. We also identified a considerable delay from relapse in some people self-referring to the clinic.12 This reduces the ability to provide relapse treatment within the recommended time window of 14 days,7 although there is evidence that the inflammatory activity underlying clinical relapses persists for up to 2 months.45 ,46 Some patients are probably having relapses managed in primary care, or are referred to the medical admissions units rather than to the rapid-access clinic. However, recent guidance suggests that MS specialists should be involved in treatment decisions for every patient experiencing an MS relapse.7 As well as raising awareness of the rapid-access service with our patients and general practice colleagues, we should strive for comprehensive integration of community and tertiary services to allow patients with reduced mobility or limited access to hospital to receive specialist care closer to home. Finally, although a relapse is the most likely diagnosis in rapid-access setting, we frequently find alternative explanations for acute symptoms in patients with MS (figure 2 and table 1).12
Commissioning data for setting up a rapid-access MS service*
Key points
▸ Multiple sclerosis (MS) relapses impact on physical ability, financial and social circumstances and also influence treatment decisions.
▸ National guidelines recommend rapid access to specialist care for patients experiencing acute symptoms of MS.
▸ Diagnosing MS relapse can be challenging and clinicians running the clinic should be aware of differential diagnoses and confounding factors.
▸ A multidisciplinary approach to rapid-access care is likely to benefit patients and allows most relapses to be managed in the outpatient setting.
▸ Planning of a rapid-access MS service can be guided by population characteristics.
References
Footnotes
Contributors NPR had the original idea for and edited the manuscript. ECT wrote the initial draft of the manuscript. MW edited the manuscript and produced the web-based database software shown in figure 3.
Funding This paper was written in part while ECT was a Biogen Idec Postdoctoral Fellow. Additional funding sources: National Institute for Social Care and Health Research (NISCHR), MS Society and The Wellcome Institute.
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Martin Duddy, Newcastle-upon-Tyne, UK.
Linked Articles
- Editors' commentary
Other content recommended for you
- Change in disability in patients with multiple sclerosis: a 20-year prospective population-based analysis
- Quantitative effect of sex on disease activity and disability accumulation in multiple sclerosis
- How common is truly benign MS in a UK population?
- Mycophenolate mofetil in multiple sclerosis: a multicentre retrospective study on 344 patients
- Consistent control of disease activity with fingolimod versus IFN β-1a in paediatric-onset multiple sclerosis: further insights from PARADIGMS
- Factors associated with and long-term outcome of benign multiple sclerosis: a nationwide cohort study
- UK multiple sclerosis risk-sharing scheme: a new natural history dataset and an improved Markov model
- Brain atrophy and lesion load predict long term disability in multiple sclerosis
- The Kurtzke EDSS rank stability increases 4 years after the onset of multiple sclerosis: results from the MSBase Registry
- Term pregnancies and the clinical characteristics of multiple sclerosis: a population based study