Article Text

Abstract
Benign paroxysmal positional vertigo (BPPV) is the commonest cause of dizziness. It is characterised by brief episodes of vertigo and imbalance with nystagmus. The direction of nystagmus allows the identification of the culprit semicircular canal. As it is readily treatable—and often curable—BPPV should not be missed. Although recurrent episodes of vertigo triggered by movement suggest BPPV, the diagnosis can only be confirmed with the Dix-Hallpike manoeuvre. Here we review the diagnostic manoeuvres required to diagnose BPPV, and the various repositioning manoeuvres for treating different types of BPPV.
- VERTIGO
- NEUROOTOLOGY
- EYE MOVEMENTS
- benign paroxysmal positional vertigo
Statistics from Altmetric.com
Introduction
Dizziness is a common neurological presentation; a good clinical long-term outcome depends on a correct initial diagnosis. Benign paroxysmal positional vertigo (BPPV) is the commonest cause of dizziness among the general population, accounting for one-fifth of referrals to specialised vertigo clinics. Its incidence is conservatively estimated at 64 per 100 000 population per year.1 The age at onset spans from childhood to old age, but most are aged over 40 years; it may even be more common among the elderly population (prevalence approaching 9%).2 BPPV is rare in children, where migraine or malignancy should first be excluded (Saka, 2012). Women are affected twice as often as men. BPPV was first described by Róbert Bárány in 19213; Charles Hallpike and Margaret Dix later detailed the brief episodes of vertigo and imbalance associated with nystagmus in 1952.4 The direction of the nystagmus identifies the culprit semicircular canal.
BPPV should not be missed, or even fleetingly dismissed, given that it can be so easily treated. Patients often attend ‘dizzy clinics’ with vertigo spanning months, even years, yet leave the clinic cured and relieved, though wondering why it took so long for a doctor to diagnose their BPPV!
Pathophysiology
BPPV is probably caused by calcium carbonate crystals (otoconia, or canaliths) settling within the endolymphatic fluid of one or more semicircular canal, although this has been shown only for the posterior canal.5 Posterior canal BPPV pathophysiology is inferred from the provocative position and the resulting torsional–vertical nystagmus, reflecting the excitatory connections between the posterior semicircular canals and specific extraocular muscles. Although it remains conjecture rather than established fact, BPPV's clinical features are consistent with otoconia in the posterior canal that are denser (heavier) than the surrounding endolymph.6 Thus, after the head is moved in the plane of the canal, the otoconia slowly fall to the canal's lowermost portion, generating endolymph movement7; this deflects the cupula and activates the vestibular nerve, causing nystagmus. There is often a short lag between changing the head position and the nystagmus and vertigo, attributed to the time taken for the otoconia to be displaced within the fluid and also the otoconia's adherence to the membranous wall of the canal. This adherence may explain why a brisk head movement is often needed to trigger vertigo. The vertigo and nystagmus last only as long as the otoconia take to settle again, typically 5–10 s, but sometimes longer.
Further support for this mechanism comes from labyrinthine surgery and autopsy reports of agglomerated masses within the posterior semicircular canal,8 displaced from the utricular macula and confirmed as otoconia on electron microscopy.
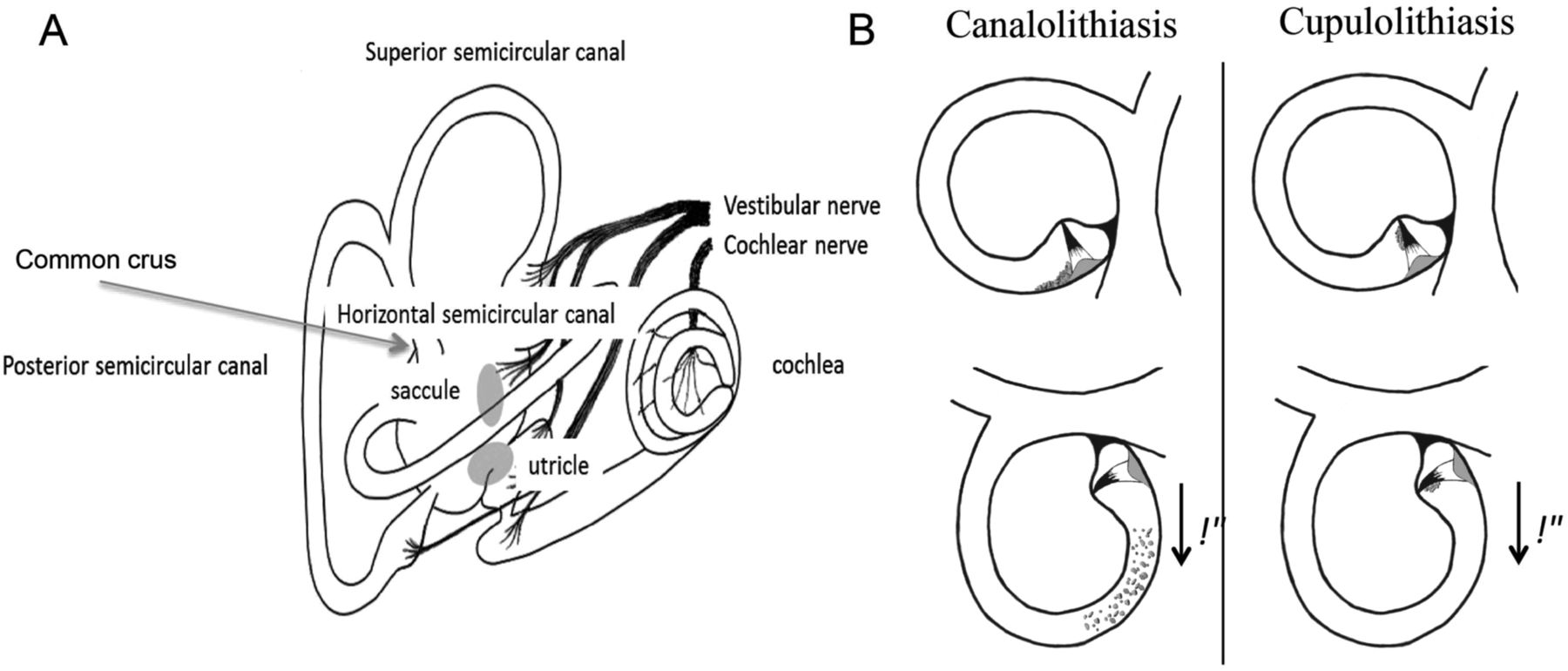
Otoconia causing BPPV originate from the otolith organs—the linear acceleration detectors in the inner ear (figure 1A). However, these can become dislodged—spontaneously or, for example, during head trauma—and find their way into the opening of the semicircular canals, leading to BPPV. Otoconia commonly end up in the posterior semicircular canal—the lowermost canal—due to gravity. Horizontal canal BPPV is much less common, causing 10–20% of cases,9–11 and anterior canal BPPV comprises only 5%.12–14 BPPV following head trauma is often bilateral.

(A) Anatomy of the labyrinth showing the three semicircular canals orientated orthogonally to each other, and the utricle and saccule (constituting the otolith organs). (B) Pathophysiology of canalolithiasis (left panel) and cupulolithiasis (right panel).
The chemical composition of otoconial debris is unclear. One study found patients with BPPV had higher serum uric acid levels than controls15: hyperuricaemia-associated crystal formation in the semicircular canals makes an attractive hypothesis, and although not universally reproduced16 is certainly a potential mechanism.17 ,18
Canalolithiasis versus cupololithiasis
Crystals within the canal are usually freely moving (canalolithiasis-type BPPV). However, they sometimes accumulate and adhere to the cupula (cupulolithiasis-type BPPV; figure 1B). They have similar presentations but different examination findings.
Clinical presentation
BPPV is usually of the ‘canalolithiasis posterior canal’ type; hence, most BPPV cases present with violent but brief attacks of vertigo (seeing the room spin) triggered by a change in head position. These last only seconds but, particularly in the first attack, patients may report that they are spinning continuously, such is its severity and the inaccuracy of subjective recall of time. Attacks abate if the head is kept completely still, but a change of position—often in an attempt to stop the vertigo—might provoke a further attack. Thus, patients may report multiple brief attacks as a single prolonged episode. Nausea is common but vomiting is rare given the brevity of each attack. Prominent positional vomiting hints at an alternative more sinister cause affecting the periaqueductal grey matter, floor of the fourth ventricle, or the deep cerebellar nuclei.19 ,20 BPPV patients commonly develop anxiety and avoidance behaviour, for fear of triggering or exacerbating symptoms. If untreated, vertigo episodes can persist for weeks, months or even years. Occasionally, nausea and imbalance alone persist beyond the episodes of vertigo, and may be more bothersome than the positional vertigo.
The common triggers in BPPV are bending forwards (brushing teeth over a sink, or looking down from screen to keyboard), looking up (hanging washing, or reaching up to a shelf), and turning over in bed. Indeed, vertigo triggered by turning in bed is almost always BPPV.
Making the diagnosis
A history of recurrent vertigo episodes triggered by movement suggests BPPV, but the diagnosis can only be confirmed with the Dix–Hallpike manoeuvre4 (figure 2 and see online supplementary video 1). This should be performed on every patient presenting with dizziness because: BPPV is common, it carries an excellent treatment success rate, and dizzy symptoms are difficult for patients to describe (making history alone often insufficient to give a confident diagnosis). The difficulty is that there are six canals (three in each ear) where crystals may potentially lodge. One practical approach is to perform a Dix–Hallpike manoeuvre for right and left posterior semicircular canals—these are the most commonly involved—and then to assess the horizontal canals if the symptoms suggest BPPV but Dix–Hallpike is negative, or if there is horizontal nystagmus during a posterior semicircular canal Dix–Hallpike manoeuvre. Figure 2 shows a traditional Dix–Hallpike manoeuvre. A modified sideways manoeuvre (figure 3 and see online supplementary video 2) is easier to perform clinically, and allows a treatment (Semont manoeuvre21 figure 8 and see online supplementary video 5).

Dix–Hallpike manoeuvre exploring the right ear. The patient begins seated in the couch, with the feet longitudinally. The head is then turned towards the ear being explored (right ear in this case). With a rapid motion, the patient is tipped backwards such that the head is hyperextended by approximately 30°, and overhangs the end of the couch. In the presence of BPPV, there is upbeat and torsional nystagmus beating towards the ground (see online supplementary Nystagmus video 1), with vertigo, usually lasting only 5–10 s. It is important to warn the patient about this, and ask him/her to keep the eyes open. It may be necessary to open the eyes lightly using your thumb and index fingers.
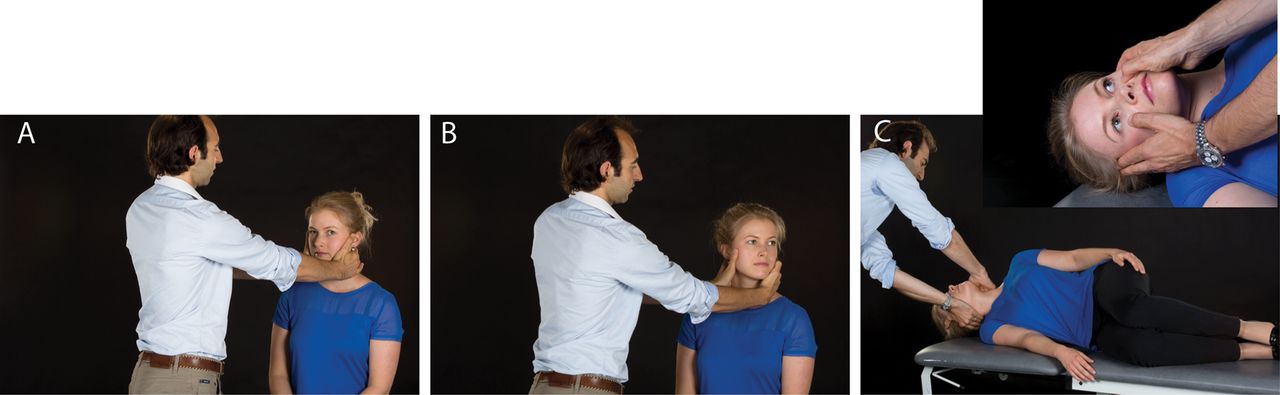
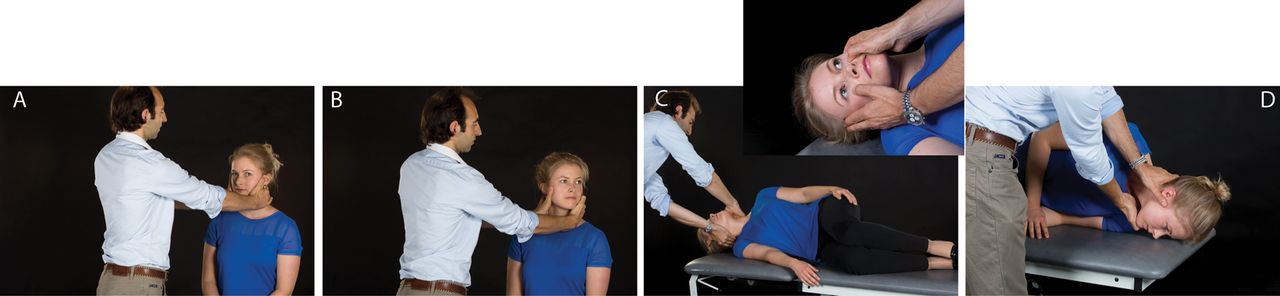
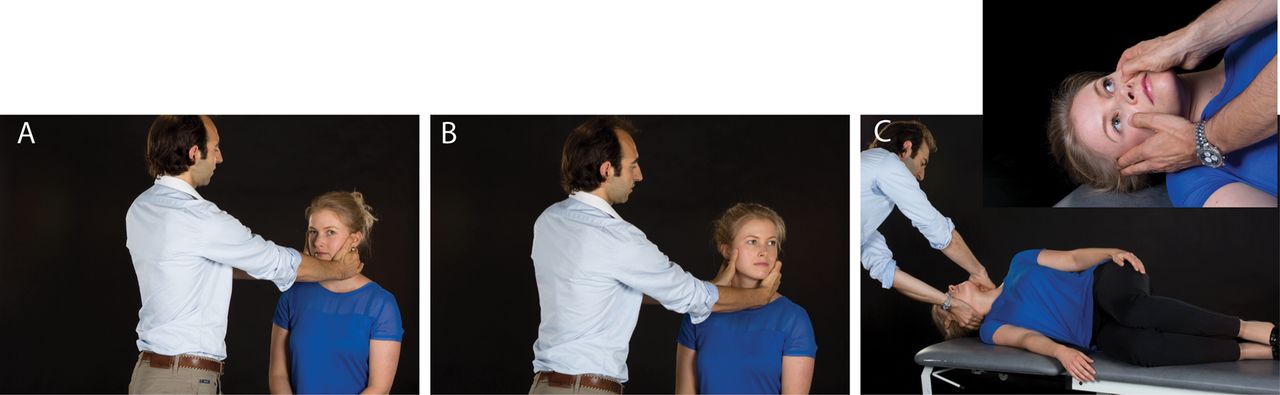
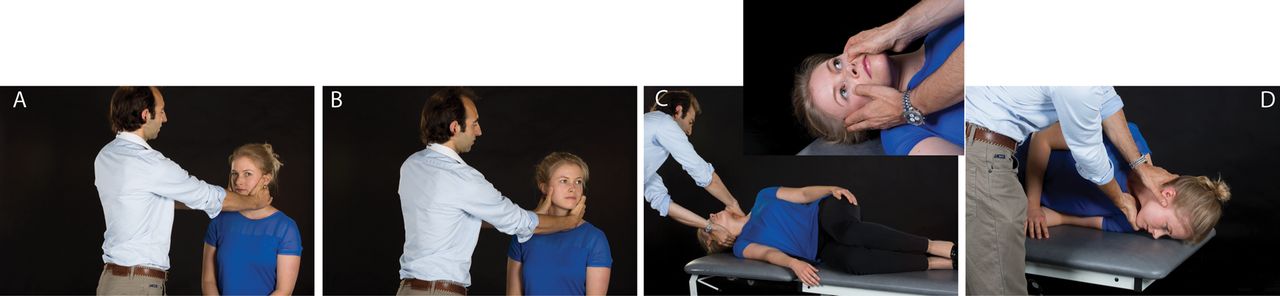
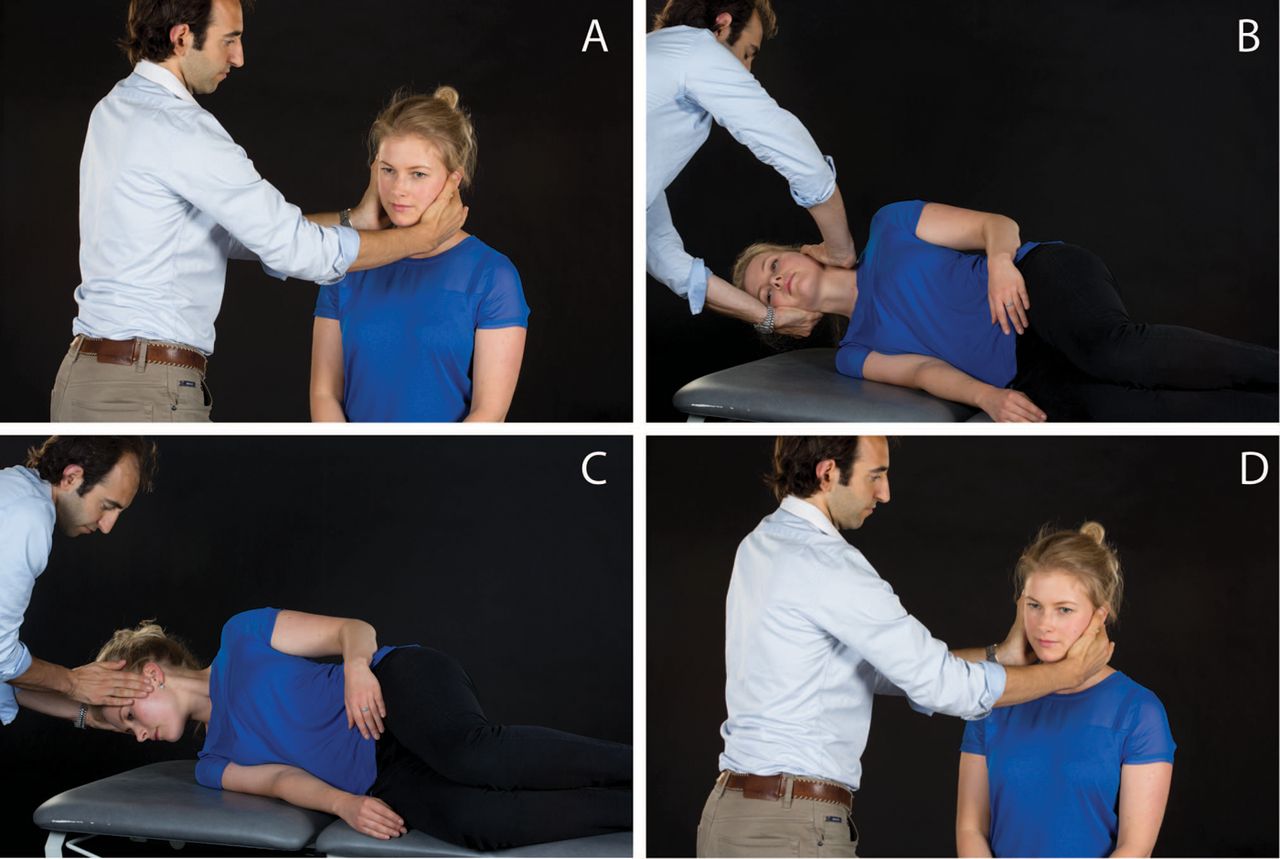
Modified ‘sideways’ Dix–Hallpike exploring the right ear. Here, the patient begins seated in the centre of the couch, with the legs hanging down the side (A). The patient's head is then turned away from the ear being explored (right ear in this case, (B)). The patient is then rapidly tipped sideways, making sure that the head does not change position (C). Note that the nose should point upwards, in which case it will be easy to see the eyes (inset). Again, in the presence of BPPV, there is upbeat and torsional nystagmus beating towards the ground.
Brain imaging (ideally MRI) is needed only if the Dix–Hallpike provokes unusual features suggesting a central problem (Box), or if the BPPV is resistant to treatment.
Dix–Hallpike features that indicate neuroimaging
-
Central positional nystagmus
-
Typically downbeat
-
No latency
-
No fatigability
-
No habituation
-
Stereotyped
Other indications for neuroimaging
-
Prolonged or severe vomiting
-
Associated neurological symptoms or signs
-
Headache
-
Hearing loss
Posterior semicircular canal BPPV
The Dix–Hallpike manoeuvre (figure 2 and see online supplementary video 1) is used to diagnose posterior canal BPPV. The patient is seated on the couch longitudinally, and the head turned by 45° towards the ear being tested (ie, head turn to the left tests the left posterior canal). The patient is quickly placed in the supine position, with the head overhanging the couch by 30°, ensuring that the head remains at 45° to the side throughout. The patient should keep the eyes open at all times and fixate on the examiner's nose, to see any nystagmus. In a patient with BPPV, the examiner sees alternating quick eye rotations towards the lowermost ear (ie, beating towards the ground), and slow rotations in the opposite direction, comprising a torsional nystagmus (see online supplementary Nystagmus video 1). Torsional or ‘rotatory’ nystagmus is best seen by focussing on the scleral vessels, rather than the pupil or the iris. The nystagmus often has a vertical upward-beating component, giving a torsional-vertical eye movement, characteristic of posterior semicircular canal-BPPV. The nystagmus usually begins about 5 s after positioning—but sometimes as late as 30 s. It then lasts a few seconds to a minute—but typically 10 s—and often parallels the sensation of vertigo. During the episode, patients with BPPV attempt to close the eyes, and may wriggle around to abate the symptoms. It is therefore worth spending time to warn the patient that the manoeuvre may induce symptoms before attempting the manoeuvre, and stress the importance of keeping the eyes open. Sometimes, the clinician has to open them gently to see the scleral vessels adequately. It is easier to see and characterise the nystagmus using video Frenzel glasses, but most practising clinicians do not have these available.
The direction of the nystagmus typically reverses on sitting up again, as the otoconia return to their original position in the canal. The intensity of the nystagmus and vertigo typically reduces on repeating the manoeuvre (fatiguability or habituation).
Canalolithiasis versus cupulolithiasis
Cupololithiasis of the posterior semicircular canal is rare, presumably related to the anatomy of the canal and our ‘upright’ posture, such that otoconia rarely accumulate near the cupula (figure 1B). When the crystals adhere to the cupula, a provocation manoeuvre causes immediate gravity-induced deflection of the cupula, activating vestibular afferents, without delay; such activation lasts for as long as the patient remains in that position, with little decay in nystagmus intensity. Thus, during the Dix–Hallpike manoeuvre, the nystagmus of cupulolithiasis-type BPPV appears immediately without latency, and does not fatigue, but the nystagmus type is the same as for canalolithiasis.
Horizontal semicircular canal BPPV
Horizontal (or lateral) canal BPPV accounts for 5–20% of BPPV.12 The lower incidence reflects the fact that it is usually self-remitting because of ‘curative’ side-to-side head movements during everyday activity. It has a lower treatment success rate than classical posterior canal-BPPV, perhaps partly because of difficulty in defining the culprit canal correctly. Horizontal canal-BPPV can be diagnosed on a traditional Dix–Hallpike manoeuvre, with the observation of pure horizontal nystagmus on laying the patient supine (see online supplementary Nystagmus video 2). However, this does not allow the examiner to identify the culprit canal, or whether it represents canalolithiasis or cupulolithiasis. To explore the cause, the patient is placed supine and the head rapidly rotated by 90° towards the explored ear22 (figure 4). A horizontal nystagmus appears, with no vertical component, in most cases with the fast phase beating towards the explored, lowermost ear (ie, leftwards if the head has been rotated to the left). Next, the head is turned towards the other side by 180°, whereby the direction of the fast phase of the nystagmus reverses (and beats towards the ground—geotropic), and is less intense. This follows Ewald's second law, stating that ampulopetal stimulation is stronger than ampulofugal stimulation for the horizontal semicircular canal, and implies the presence of canalolithiasis (see online supplementary Nystagmus video 2). A second positional manoeuvre, the ‘Bow and Lean Test’23 can identify further whether the affected canal is on the right or left side (figures 5 and 6, and see online supplementary video 3). For canalolithiasis, the right ear is affected if there is right-beating nystagmus on bowing, and left-beating nystagmus on leaning the head backwards. For cupulolithiasis, the right ear is affected if there is left-beating nystagmus on bowing, and left-beating nystagmus on leaning. Using these techniques, the clinicians who developed the test reported a higher success rate for horizontal canal-BPPV treatment using this diagnostic manoeuvre, than by using Ewald's second law to determine the affected side.24 Nevertheless, this manoeuvre requires specialist equipment (oculography) to determine the nystagmus direction correctly, since it is difficult to see in the head-down (bow) position.

Pagnini–McClure manoeuvre (‘head roll test’) to differentiate between canalolithiasis and cupulolithiasis-type horizontal canal BPPV. The patient lies on the couch with the head elevated to 30°, such that the horizontal canals are orientated in the true vertical plane. The head is then rolled in one direction, by 90° (A), and the intensity and direction of nystagmus noted. After 30 s, the head is returned to the centre. The head is subsequently rapidly rotated by 90° in the opposite direction, again noting the direction and intensity of the nystagmus (B). The causative site is determined by applying Ewald's second law—which states that ampulopetal stimulation is stronger than ampulofugal stimulation. The affected ear is determined as the side showing more intense nystagmus in the canalolithiasis-type BPPV. In cupulolithiasis BPPV, the affected ear has less intense nystagmus.

‘Lean and Bow’ test for localising the affected ear in horizontal canal BPPV. The patient begins seated in the centre of the couch with the legs hanging down (A). The head is then rapidly tipped upwards (‘lean’, (B)), and any nystagmus observed and recorded. The patient's head is then brought rapidly down into the ‘bow’ position, and nystagmus again observed and recorded (C).

Interpretation of ‘Lean and Bow’ test (adapted from Choung et al23). (A) In canalolithiasis-type horizontal canal BPPV, the affected ear is determined by the direction of the fast-phase nystagmus during bowing (ie, right-beating nystagmus during bowing implies right-sided horizontal canal-BPPV, left side of panel). (B) In cupulolithiasis-type BPPV of the horizontal canal, the affected ear is determined by the direction of the fast-phase nystagmus during the leaning (ie, right-beating nystagmus during leaning implies right horizontal canal-BPPV, left side of panel).
The nystagmus of horizontal canal-BPPV is purely horizontal, it typically has a shorter latency, may last longer than 1 min, is more intense, and less fatiguable on repeated testing than classical posterior canal-BPPV.
Anterior semicircular canal BPPV
The anterior canal variation of BPPV is the least common type of positional vertigo, with frequency ranging from 1% to 24%25 most likely because its posterior arm opens vertically down directly into the common crus and particles trapped here are easily eliminated during normal head movements before they cause symptoms. Anterior canal BPPV presents with brief attacks of vertigo triggered by changes in head position, but the nystagmus is predominantly downwards, with a torsional (rightwards or leftwards) component. The diagnosis is confirmed with the Dix-Hallpike manoeuvre (figures 2, 3 and 14, see online supplementary video 1, and Nystagmus video 3) which stimulates both (posterior and anterior) semicircular canals. Positioning the patient in the straight back or head-hanging position can help in this situation to show downbeat nystagmus, not seen in posterior canal BPPV. Positional downbeat nystagmus, however, is also a feature of posterior fossa lesions, in particular, cerebellar degeneration, including multiple system atrophy.26 Therefore, it is important to rule out a central aetiology in patients with positional downbeat nystagmus before attributing the nystagmus to anterior canal BPPV, ideally with MRI of the brain. Anterior canal BPPV may also result from particles entering this canal during repositioning manoeuvres for posterior canal BPPV,14 ,27 which can be treated with several additional manoeuvres (see below).
BPPV of multiple canals
BPPV can coexist in several canals, making the diagnosis and subsequent treatment more challenging. A positive Hallpike manoeuvre with upwards and torsional nystagmus on both sides strongly suggests bilateral BPPV of the posterior canals (commonly post-traumatic). However, one must ensure that during the manoeuvre the head is orientated in the plane of the canal being explored; inappropriate head orientation may lead to an incorrect diagnosis of bilateral BPPV.28 In one series of patients with BPPV diagnosed using video-oculography (more sensitive at picking up subtle nystagmus than the naked eye), 20% had multiple canal involvement on positional testing. We would encourage clinicians to carry out the positional manoeuvre in patients with postconcussional syndromes, as BPPV can cause much of such patient's dizziness.
‘Subjective BPPV’
Some patients report vertigo and nausea during a positional manoeuvre, without there being the typical nystagmus. Repositioning manoeuvres are highly effective in patients with such ‘subjective BPPV’.29–31 Possible causes for the absence of typical nystagmus are: subtle nystagmus easily missed by the clinician, nystagmus fatiguability following repeated manoeuvres, or a milder form of positional nystagmus that is potentially suppressed by visual fixation.29 It is in these rare cases that either recording equipment (oculography) or Frenzel's glasses—removing visual fixation—may truly be needed for diagnosis. Another type of BPPV, with positional vertigo, no nystagmus on Dix–Hallpike, and a short vertigo spell on sitting up, may result from otoconia in the short arm of the semicircular canal.32
Repositioning treatment manoeuvres
BPPV treatment has shifted from vestibular sedatives and avoidance of triggering head positions through habituation exercises,33 to tackling the underlying cause by repositioning manoeuvres.4 These are designed to move the offending crystals from the semicircular canals into the utricle through the common crus (figure 1). Despite a wealth of evidence supporting particle repositioning manoeuvres for BPPV,34 many physicians still mistrust them, perhaps through not performing the manoeuvres frequently enough to feel confident.
The keys to successful treatment are correct positioning of the head (and therefore of the semicircular canals) and the speed of the manoeuvre. Although not essential, it can help to ask a colleague assist in performing the manoeuvre to ensure correct trajectory and adequate speed of movement, and avoid damaging your back!
Posterior semicircular canal BPPV
Once the diagnosis of posterior canal BPPV has been established (with a Hallpike manoeuvre), treatment options are either the traditional Epley manoeuvre35 (figure 7 and see online supplementary video 4) or Semont manoeuvre21 (figure 8 and see online supplementary video 5). These may trigger vertigo so many patients with active BPPV might be reticent to have them done. For all positioning manoeuvres, clinicians must spend a few seconds explaining what is done and why. Note that chronic drug administration has no role in BPPV management and prescription of vestibular sedatives—for prominent nausea or vomiting—should be for no more than 2–3 days.36

Epley manoeuvre for treating right ear posterior canal BPPV. The first stage of the manoeuvre is the Dix–Hallpike manoeuvre (A–C). After 30 s, the patient's head is rotated towards the other side (leftwards here, (D)), and held in this position for a further 30 s. During this time, the patient is asked to rotate the body so that he/she is lying on their left shoulder (E). It is important to hold onto the head while the patient is instructed to turn, so that it does not change position. The patient's head is rotated by a further 90° to the left, to face the ground (F), and held for 30 s. The patient is now sat up, with the head still looking over the right shoulder (G), for 30 s. Finally, the patient's head is brought towards the midline, and the neck flexed, chin down through 45° for a final 30 s (H). The procedure is reversed for left posterior canal-BPPV.
Semont (liberatory) manoeuvre for treating right posterior canal BPPV. The first stage of this manoeuvre is the same as the modified ‘sideways’ Hallpike (A–C). When nystagmus develops, the patient is held in that position for 30 s. The patient is then rapidly ‘swung’ from this position, by 180° to the opposite side, ensuring that the head is not moved (D). Note that in the starting position, the nose is facing upwards, but then faces downwards at the end of the manoeuvre. The manoeuvre is reversed for treatment of left-sided BPPV.
Epley
In the Epley manoeuvre (see online supplementary video 4), the patient is seated longitudinally on the couch, facing the examiner (figure 7A). The head is then turned 45° towards the side of the affected canal (figure 7B). The patient is then rapidly tipped backwards, such that the head overhangs the couch by a few centimetres, and the neck lies extended (figure 7C). The patient is held in this positioning for 30 s, during which there will be nystagmus (beating towards the lowermost ear in the case of posterior canal-BPPV). The patient's head is rapidly rotated by 90° (figure 7D), to face the other side. This position is held for another 30 s, during which time the patient should gently rotate his/her body to lie on their shoulder. The head must be held firmly during this, so that it does not change position. The patient's head is once again rotated 90° so that the nose faces the ground (figure 7F), and held for 30 s. The patient is now quickly sat up, and the head angled down (figure 7H). Note that it helps if the couch is separated from the wall when attempting the Epley manoeuvre, as you will need access to both sides of the couch. Indeed, during a correctly executed Epley manoeuvre, the patient gets on the couch on one side and off on the other. Figure 7 shows an Epley manoeuvre treating right posterior canal-BPPV (reversed for left posterior canal-BPPV).
Semont manoeuvre
The patient begins seated in the couch directly facing the examiner, with the legs hanging from the side (figure 8 and see online supplementary video 5). The nose is turned away from the affected canal (eg, for right posterior canal-BPPV, turn the head to the left), and the patient is quickly tipped on to the right shoulder. Note that the nose should be pointing upwards (and you should therefore be able to see the eyes clearly). In this position, you should see the typical torsional (‘rotatory’) nystagmus beating towards the lowermost ear in posterior canal-BPPV. The keys to successful treatment are the correct trajectory (the head must not rotate as the patient is ‘swung’) and speed of movement, which should produce sufficient force to overcome gravity.37
Which one to use?
The two manoeuvres are equally effective. Our personal experience suggests that the Semont manoeuvre is easier than the Epley in patients of slight to moderate size, and far easier to remember for the physician. Ultimately, the procedure chosen depends upon the practitioner's experience and preference. If one has been unsuccessful, it may be worth trying the other.
Horizontal semicircular canal BPPV
There are no formal clinical trials to evaluate the effectiveness of horizontal canal-BPPV repositioning manoeuvres. Because of their orientation, crystals in the horizontal canals are readily displaced during everyday head movements, resulting in spontaneous resolution. In patients with persistent symptoms, the most commonly used manoeuvre is the ‘barbecue roll’ (figure 9 and see online supplementary video 6) described by Lempert et al.38 Here, the patient begins in a supine position with the head turned by 90° towards the affected ear (usually the side evoking the most nystagmus). The head is rapidly turned by 90° to the opposite side, followed by a further 90° turn after 1 min, and a final 90° turn 1 min later (total 270° turn).

Barbecue roll to treat left ear horizontal canal BPPV. (A) The patient's head is positioned with the head turned towards the affected side and then rapidly turned towards the unaffected side (A). The patient is asked to twist the body by 90° (B), and (C) the head is rapidly rotated through 90° towards the unaffected side (face up). (D–G) A series of 90° head rotations towards the unaffected side are performed, until the patient has turned through 360°, and the head is in the unaffected ear-down position. The head is then turned to the face-up position (H), and the patient is sat up on the couch; 20 s intervals should be applied between each step.
An alternative treatment is the barrel rotation, introduced by Epley,39 in which patients turn 180° on the examination couch in the direction of the healthy ear, starting in the supine position, and ending in the prone position (figure 10 and see online supplementary video 7).
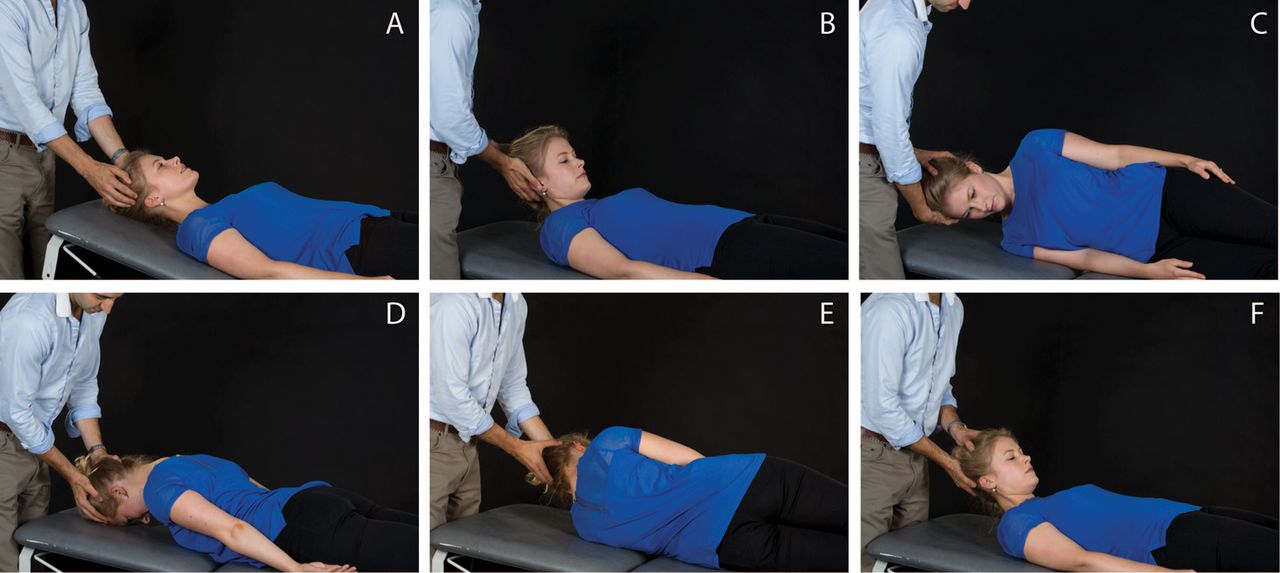
Barrel rotation for treatment of left horizontal canal BPPV. The patient begins by lying in the supine position (A), and the chin is brought down onto the chest (B). The head and body are then rotated together toward the unaffected side (C–E). One continues to roll the patient in this direction through 360° (F). Keeping the chin bent down will help prevent moving the particles into the posterior canal.
In the Gufoni manoeuvre40 (figure 11 and see online supplementary video 8) the patient begins seated with both legs hanging from the side of the couch. The patient is then made to lie down quickly towards the unaffected side, keeping this position for 2 min. There ensues a rapid 45° rotation of the head towards the ground (nose down), maintained for a further 2 min, before the patient is returned to the seated position. One of the advantages of this manoeuvre is that the patient is moved towards the side with the least nystagmus (and, therefore, fewest symptoms).

The Gufoni manoeuvre for treatment of left horizontal canal BPPV. The patient begins seated on the edge of the couch, arms held close to the body, and hands resting on the knees (A). The patient is then made to lie down towards the opposite side of the affected ear with a rapid sideways movement (B), and kept in this position for 2 min. There follows a rapid rotation of the head by 45° towards the floor (C), and this position is again held for 2 min. Finally, the patient is slowly returned to the starting position (D).
Finally, the Vannucchi manoeuvre, the prolonged positional manoeuvre,41 involves placing the patient in the lateral decubitus position with the affected ear facing upwards for 12 h. The authors reported a 90% efficacy with this technique, although in practice, compliance with such positioning is often very low. However, patients may spontaneously have adopted sleeping on the healthy side (the one with less vertigo and nystagmus), and this may partly explain the high rate of spontaneous resolution in horizontal canal-BPPV.
Anterior semicircular canal BPPV
There are several repositioning manoeuvres for anterior canal BPPV, but given its rarity, there is scant evidence to guide treatment. The most commonly used treatment manoeuvres are variants of posterior canal procedures, namely reversed Epley or Semont manoeuvres. Other procedures are those of Yacovino et al42 (figure 12 and see online supplementary video 9) and Kim et al,43 although the latter lacks a logical anatomical explanation for their perhaps overly enthusiastic reported outcome.

The Yacovino manoeuvre to treat right anterior canal BPPV. This repositioning manoeuvre comprises three steps: (A) from the head straight sitting position, (B) a head-hanging manoeuvre is performed with the head brought to at least 30° below the horizontal (neck hyperextended. (C) After 30 s, the patient's head is moved quickly forwards ‘chin to chest’, followed by a final manoeuvre to bring the patient to the starting sitting position.
Our preference is the reversed Semont manoeuvre (figure 13 and see online supplementary video 10), which is straightforward for practitioner and patient, and modelling37 confirms it as rational treatment.

Reversed Semont manoeuvre to treat right anterior canal BPPV.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Three-dimensional video-oculographic recording of a patient with suspected anterior canal BPPV. Eye movements following a right and left Dix–Hallpike manoeuvre show predominantly downbeat nystagmus, but there is a clear torsional component with both positional manoeuvres. Adapted from Bertholon et al.26
Instructions after a repositioning manoeuvre
Traditional advice for patients—to remain upright for 48 h following a liberatory manoeuvre, or to avoiding lying down on the affected side for 7 days—is not effective.44 ,45
Unusual types of BPPV
BPPV involving multiple canals is uncommon, but is a diagnostic and therapeutic challenge. It usually affects the same canal on both sides but may involve different canals on the same or both sides. When suspecting bilateral posterior canal-BPPV, the head-hanging manoeuvre can activate both posterior canals simultaneously. Finding only vertical (upbeating) nystagmus indicates bilateral posterior canal BPPV (the torsional components are in different directions and, so, cancel each other out). If there is a torsional component, pseudobilateral BPPV is more likely, usually from inappropriate head positioning during Hallpike testing.46
Occasional patients show clear positional nystagmus, which changes direction with repeated positional manoeuvres, suggesting multiple canal involvement.47 This is reassuring as it implies a peripheral aetiology; in our experience, it is best managed by treating the canal(s) that is (are) most symptomatic.
Finally, BPPV may occasionally be refractory to treatment. In our experience, with a confident diagnosis of BPPV on history and examination, repeated manoeuvres over several days, sometimes as many as 10 times, usually resolves the symptoms. It is not clear whether this relates to the actual manoeuvres or the natural course of the condition. Some patients with refractory BPPV have structural abnormalities of the canals, detectable on 3D reconstruction MR.48 A mastoid vibrator during the manoeuvres might help to loosen crystals adhering to the canal or cupula,49 although the evidence is mixed.50 Alternatively, the clinician may simply shake the patient's head vigorously to facilitate particle motion. Patients with refractory BPPV justify referral for MR brain imaging to exclude central nervous system (CNS) pathology and referral to a specialist centre. Surgical plugging of the canal (preventing movement of otoconia within the canal) can help truly refractory BPPV.8
Red flags
Positional vertigo may occasionally result from less benign lesions of the CNS. Headache, hearing loss, or other cranial nerve or neurological symptoms with vertigo are not part of positional vertigo, and warrant further investigation. Warning signs (box) include: absence of vertigo during positional nystagmus, marked vomiting, pure downbeat nystagmus, lack of latency (ie, nystagmus starts immediately on tipping sideways or back), lack of habituation (ie, nystagmus intensity does not diminish with repeated positioning), and lack of fatigability (ie, nystagmus persists when kept in the Hallpike position).
Acknowledgments
We thank Dr Eleanor King for consenting to appear in the figures, Annabel King for the photography, Yuliya Nigmatullina for consenting to appear in the videos, the Royal Free Hospital medical illustration department for leasing their facilities, and Mr David Buckwell for recording the videos. We also thank Mr Angel Batuecas for providing the ‘anterior canal BPPV video’.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online AC-BPPV
- Data supplement 2 - Online Horizontal_BPPV
- Data supplement 3 - Online PC-BPPV
- Data supplement 4 - Online video 1
- Data supplement 5 - Online video 10
- Data supplement 6 - Online video 2
- Data supplement 7 - Online video 3
- Data supplement 8 - Online video 4
- Data supplement 9 - Online video 5
- Data supplement 10 - Online video 6
- Data supplement 11 - Online video 7
- Data supplement 12 - Online video 8
- Data supplement 13 - Online video 9
Footnotes
-
Correction notice This paper has been amended since it was published Online First. The legends of figure 9 and figure 10 have been corrected. In the first sentence of the legend to figure 9, right ear has been changed to left ear. The next 2 sentences originally read: “(A) The patient's head is positioned with the head turned towards the affected side and the patient is asked to twist the body by 90 degrees, (B), and (C) the head is rapidly rotated through 90° towards the unaffected side (face up). (D–G) A series of 90° head rotations towards the unaffected side are performed, until the patient has turned through 360°, and the head is in the unaffected ear-down position.” This text now reads: “The patient's head is positioned with the head turned towards the affected side and then rapidly turned towards the unaffected side (A). The patient is asked to twist the body by 90 degrees (B), and (C) the head is rapidly rotated through 90° towards the unaffected side (face up). (D–G) A series of 90° head rotations towards the unaffected side are performed, until the patient has turned through 360°, and the head is in the unaffected ear-down position.” In the legend of figure 10, first sentence, “right horizontal canal BPPV” has been corrected to “left horizontal canal BPPV”.
-
Contributors DK compiled the manuscript, figures and videos, and approved the final version. AMB critically reviewed the manuscript, figures and videos, and approved the final versions.
-
Competing interests None.
-
Patient consent Obtained.
-
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Michael Halmagyi, Sydney, Australia.
Linked Articles
- Editors' choice
Other content recommended for you
- Resolution of atypical posterior semicircular canal BPPV: evidence for putative short-arm location
- Dizziness demystified
- Management of benign paroxysmal positional vertigo
- Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis
- Epley manoeuvre for posterior semicircular canal benign paroxysmal positional vertigo in people with multiple sclerosis: protocol of a randomised controlled trial
- Sitting-up vertigo and trunk retropulsion in patients with benign positional vertigo but without positional nystagmus
- Posterior semicircular canal cupulolithiasis during acute pontomedullary demyelination
- Effects of vestibular rehabilitation, with or without betahistine, on managing residual dizziness after successful repositioning manoeuvres in patients with benign paroxysmal positional vertigo: a protocol for a randomised controlled trial
- Vestibular reflexes and positional manoeuvres
- Treatment of anterior canal benign paroxysmal positional vertigo by a prolonged forced position procedure