Article Text

Abstract
Aims: To investigate the diagnoses made for children referred to a “fits, faints, and funny turns” clinic.
Methods: Prospective study of 380 children referred to a dedicated secondary care clinic over an eight year period.
Results: Twenty three per cent of children were given a final diagnosis of one of the childhood epilepsies, with 48% of these having a specific epilepsy syndrome. Syncope was the commonest cause of a non-epileptic event (syncope and reflex anoxic seizures comprised 100/238, 42%) but there were a wide variety of other causes. Fifty three events (14%) were unclassified and managed without a diagnostic label or treatment.
Conclusions: In children with funny turns referred to secondary care, the diagnostic possibilities are numerous; among non-epileptic events, syncopes predominate. The majority do not have epilepsy. Unclassifiable events with no clear epileptic or non-epileptic cause are common and can be safely managed expectantly.
- AED, antiepileptic drug
- CT, computed tomography
- ECG, electrocardiogram
- EEG, electroencephalogram
- FFAFT, fits, faints, and funny turns
- MRI, magnetic resonance imaging
- diagnosis
- epilepsy
- non-epileptic events
Statistics from Altmetric.com
- AED, antiepileptic drug
- CT, computed tomography
- ECG, electrocardiogram
- EEG, electroencephalogram
- FFAFT, fits, faints, and funny turns
- MRI, magnetic resonance imaging
Epilepsies of childhood can be confused with other intermittent unusual behaviours of varied cause. This contributes to the misdiagnosis of epilepsy, particularly its over-diagnosis.1–5 This paper describes the diagnoses reached for children referred with “fits, faints, and funny turns” (FFAFT) to a dedicated secondary care clinic in a district general hospital over an eight year period (1995–2003).
METHODS
The clinic received referrals from the local borough of Bury and some from surrounding districts. Referrals came from GPs, paediatricians, child psychiatrists, paediatric neurologists (usually for ongoing care), and acute hospital admissions. Referrals included those presenting for the first time with events, and those where a diagnosis of epilepsy had already been made but where further classification and management were required. The clinic did not care for all children with epilepsy in the district (for example, some of those with straightforward diagnoses or stable epilepsy); the data presented therefore cannot be compared directly with population based studies.
Clinics were held weekly. The same clinician saw all the children (all age <16 years) and made or confirmed most of the diagnoses. A record of the diagnoses was kept prospectively. Where diagnosis was unclear, further opinions from visiting paediatric neurologists were sought. Electroencephalograms (EEGs) were done at a tertiary centre (Royal Manchester Children’s Hospital) and reported by paediatric neurologists.
Diagnoses were made primarily on clinical information, sometimes augmented by home videos of events using a camcorder loaned by the clinic to families. Families were primed by a letter sent with the appointment asking them to bring a direct witnessed account of a typical event to the first consultation and details of any relevant family history.
RESULTS
Figure 1 present categories of diagnoses.
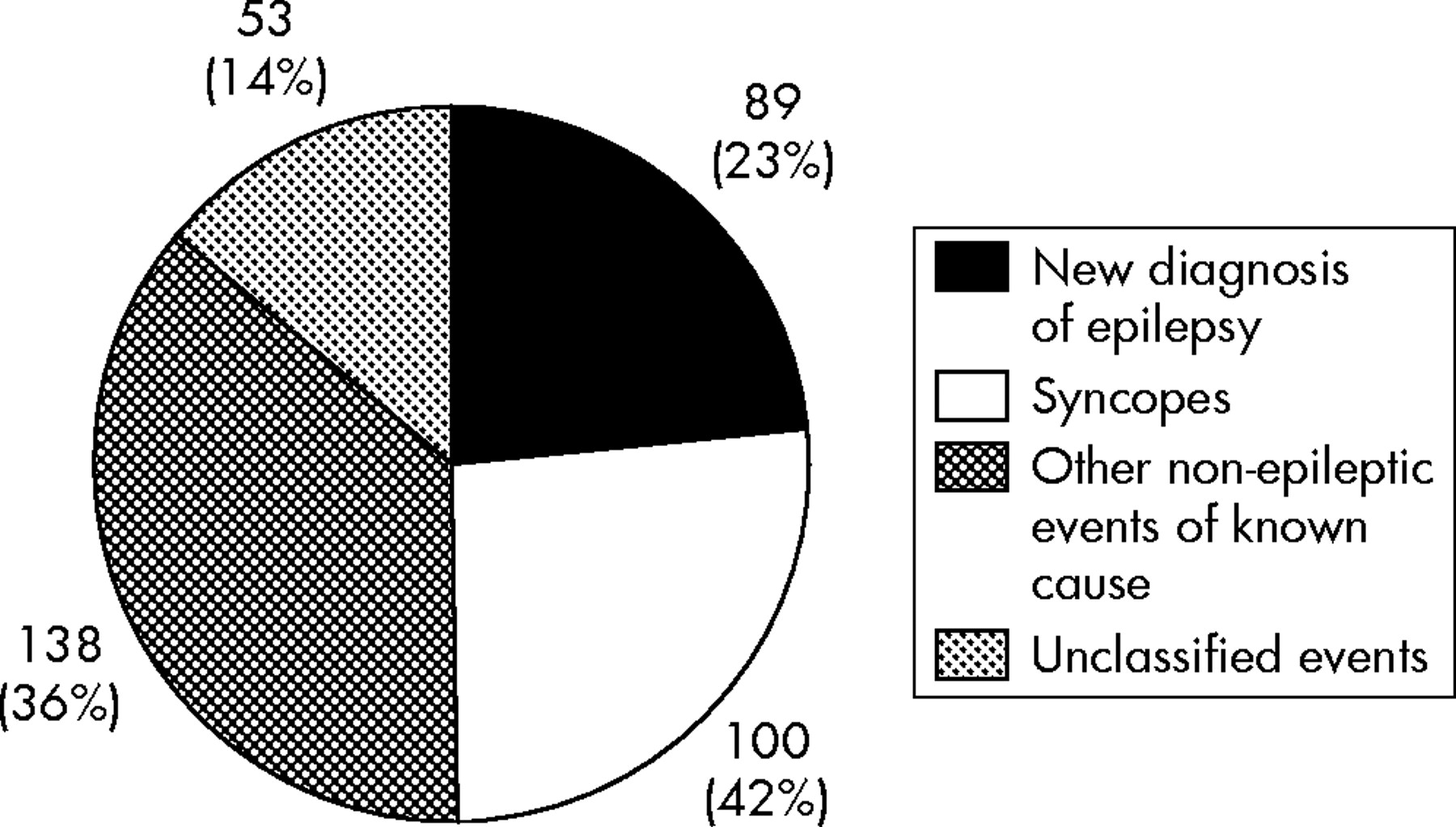
Categories of diagnoses (n = 380).
New diagnosis of epilepsy
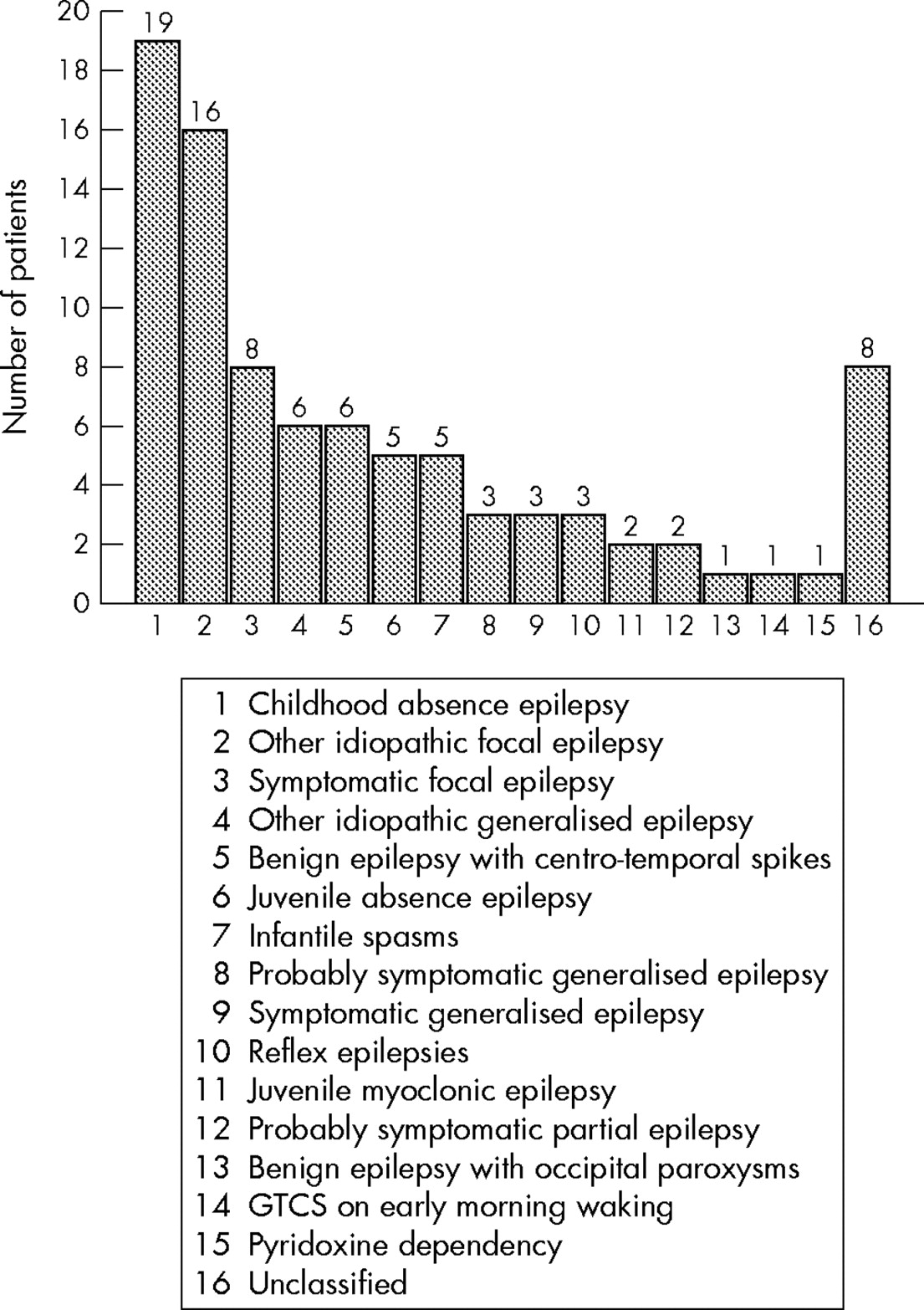
Epilepsy was newly diagnosed in 89 children (50 boys and 39 girls) (fig 2). The median age of onset was 5 years (range 0–15 years). Fifty four per cent were classified as having a generalised epilepsy, 37% a localisation related epilepsy, and 9% had unclassified epilepsies. Specific epilepsy syndrome was diagnosed in 43/89 (48%). A cause was found in 17%; 53% were thought idiopathic and the remainder were probably symptomatic.

Epilepsy diagnoses (n = 89).
Antiepileptic drug (AED) treatment, when prescribed, was started within 3 months of presentation in 54% of cases, between 3 and 20 months in 41%, and beyond 20 months after presentation in 5%. Twenty one children (24%) were seen by a paediatric neurologist.
EEGs were performed before starting AEDs in 67/89 cases. Abnormalities were reported in 75/89 (84%); of these, 64/75 were abnormal at the first EEG, but for 11/75, repeat EEG, sleep EEG, or prolonged EEG were required. Neuroimaging was performed in 59/89 (66%): 47 had computed tomography (CT) scans (11 showed abnormality); 46 had magnetic resonance imaging (MRI) scans (19 showed abnormality); and 28 had both. Seven children had a normal CT followed by an abnormal MRI scan.
Other diagnoses
Figure 3 presents non-epileptic diagnoses.

Non-epileptic diagnoses (n = 238).
Syncope
The commonest cause of a non-epileptic spell was syncope, accounting for approximately 42% of all diagnoses. Syncopes are events caused by “a sudden reduction in cerebral perfusion by oxygenated blood, either from a reduction in cerebral blood flow itself or from a drop in the oxygen content (or a combination of the two)”.8 One hundred children had a final clinical diagnosis of syncope (median age 9 years, range 8 months to 16 years), with girls (n = 55) represented more than boys (n = 45). Twenty two were seen after a single event and 78 after recurring events.
Thirty five children had syncopal events in set situations; for example, getting out of bed or having hair care. Specific immediate triggers for syncope were common (77/100 children); 34 occurred after minor injury, including immunisation or blood tests; 26 with orthostatic stresses, for example, standing still or standing from sitting; 9 if wishes were thwarted; 9 with sudden surprises/shocks; 8 after seeing blood; 4 with exercise; and 2 with “semantic syncope”—that is, in response to a gory story or the word “testicles”. Twenty seven children had more than one trigger. Auras included light-headedness, visual disturbance, feeling hot and sweaty, and nausea. Eighty seven children followed auras with loss of consciousness. Forty five of these had at least one anoxic seizure (tonic posturing and/or clonic or myoclonic jerking), 32 of which were triggered (“reflex”); the age distribution for this subgroup was similar to that for the syncopal group as a whole (median 9 years, range 1–15 years). Post-syncopal symptoms varied from immediate or rapid recovery (n = 27) to combinations of nausea, vomiting, headache, confusion, and drowsiness for minutes or hours.
Clinically the mechanisms of syncope were prolonged expiratory apnoea (n = 8), vagally mediated (n = 54), orthostatic (n = 22), or unclear (n = 16).6 Most patients had an electrocardiogram (ECG) (n = 82); only one showed an abnormality (borderline prolonged QT interval). One MRI brain scan was performed because of a coincidental history of complicated migraine. Two children with recurring events were referred to a paediatric cardiologist.
Psychological
Episodic spells due to psychological causes were common (n = 31). The median age of onset was 12 years (range 2–16 years), with more girls (n = 18) than boys (n = 13). Pseudoseizures (non-epileptic events or illness behaviour presenting as seizures) occurred in five cases and indicated significant psychopathology. Other psychological causes included panic attacks, temper tantrums, and uncharacteristic unusual behaviours, for example, amnesia after thumping best friend.
Miscellaneous
Thirty one children had events with various causes (see fig 4). These included non-kinesogenic paroxysmal choreoathetosis, kinesogenic paroxysmal choreoathetosis, benign tonic up gaze of infancy, jitteriness, delirium, and Sandifer syndrome. Three babies had the characteristic features of benign neonatal sleep myoclonus. Three children with poorly controlled asthma presenting as dizziness and breathlessness on exertion were included in this group. Unusual causes such as a baby groaning in sleep and a baby with recurrent distress/colic due to milk intolerance were also included.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Miscellaneous diagnoses (n = 31).
Daydreams
Children who daydream are sometimes referred because of concern that they may have childhood absence epilepsy. In this series 20 children with daydreams were seen (median age 8 years, range 6 months to 13 years). In 16 of these children EEGs were performed, all of which were normal. Elements in the history suggesting daydreams rather than childhood absence epilepsy included male sex, situational events, lack of eyelid movements during events, and prolonged “absences” (more than a few seconds). Children who daydream were also more likely to have attentional problems, learning difficulties, or hearing impairment.
Night terrors
Seventeen children had a history of waking with a combination of fear, distress, confusion, and often somnambulism within two hours or so of going to sleep. Characteristically there was a single event only per night. Boys (n = 11) were affected more than girls (n = 6), the median age of onset was 7 years (range 1–11 years), and there was often a long history before presentation (average duration of symptoms 22.8 months). Four children had routine EEG and one had a sleep EEG. Chlorpheniramine was prescribed for one child and trimeprazine for another.
Migraine
Twelve children (median age 13 years, range 6–15 years) were seen with migraine, often involving symptoms including dizziness, nausea, paresthesiae, and visual disturbance. EEGs (n = 7) and CT brain scans (n = 7) were requested in children with suspected focal seizures or basilar migraine. Alice in Wonderland syndrome, a migraine variant involving intermittent micropsia or macropsia or other distortions of visual perception, was diagnosed in a further four children.
Benign paroxysmal vertigo
Nine children (median age 3 years, range 1–11 years) presented with abrupt episodes of vertigo without loss of consciousness, which settled with time. The possibility of focal seizures warranted an EEG and ECG in two children. One child was referred to an audiologist with hyperacusis, and another to an ENT specialist with possible vestibular dysfunction associated with recurrent ear infection.
Ritualistic movements
Eight children (median age 2 years, range 1–6 years) presented with repetitive manneristic behaviours, often with a glazed, contented expression. Average duration of symptoms at presentation was 22 months. Included in this group were three girls with episodes involving rocking pelvic movements and a glazed expression thought to be gratification phenomena. Most children could be easily distracted out of these spells.
Exaggerated parental anxiety/fabricated illness
Six children were seen with factitious seizures. Parents either gave good descriptions of seizures, which could not be independently verified, or remained convinced of the diagnosis of epilepsy despite reassurance that this was not the case after full evaluation. In four cases parents eventually demurred and gave up the diagnosis, but two required social services intervention.
Unclassified events
An “unclassified event” was defined by the following criteria:
-
No clear epileptic or non-epileptic diagnosis made
-
No active treatment given
-
Child well between events
-
Normal physical examinations on repeated occasions
-
Follow up in clinic until events cease or become very infrequent
-
Family and doctor reassured about absence of significant pathology.
Unclassified events were seen in 53 children (26 boys, 27 girls; median age of onset 6 years, range 0.3–15 years).
We sent a follow up questionnaire to families of 28 children discharged after a diagnosis of “unclassified events”. The mean time from discharge for the 16 respondents was 32 months. Of the responders, eight had experienced further events (average 3, maximum 6). Events continued to decrease in frequency. None of the children had been seen by another doctor for further investigations of their events, acquired a diagnosis of epilepsy or other known cause, or received active treatment. No parent sought further advice or asked to be seen again in the clinic as a result of the questionnaire.
Case history
A 4 year old girl had two unusual “spells” in three months. On the first occasion, while running around the garden she suddenly started to scream, fell flat on her face, and became very frightened without obvious reason. She struggled as if pushing something away and said that she “did not want the lamp to fall on her”. She was dazed but not unconscious. She seemed to lose the use of her legs for a short while. She was sleepy for an hour afterwards. There was no obvious precipitating factor, no colour change, no incontinence, and no involuntary movements of eyes or limbs. Six weeks later she had a further event while running through sand dunes. She screamed, fell to the ground, and was frightened, this time of “monsters”. Again she was quiet for some time before returning to her normal self. Apart from these two events she was well. Physical examination was normal. EEG and ECG were normal. At review in clinic one month later no further events had occurred and she was discharged from clinic. Follow up after 58 months revealed that she had had no subsequent similar events.
DISCUSSION
Unusual mannerisms, perceptions, and behaviours in infants, children, and teenagers are common. Such events cause considerable concern, especially if they are dramatic, uncharacteristic, or repeated. Finding an explanation can be difficult.7,8,9,10,11,12,13 Causes may be epileptic or non-epileptic and medical evaluation hopes actively to make or refute a proposed diagnosis of epilepsy and to provide treatment and reassurance as necessary.
In this review 23% of new referrals eventually received a diagnosis of epilepsy. Our philosophy has been to avoid this diagnosis as much as possible unless it is clearly proven, or at least, with time, more likely than not. As has been said before, “if the cause of a ‘funny turn’ is unclear, it is better to err on the side of ‘not epilepsy’ and subsequently correct that decision than to give the label of ‘epilepsy’ and try to retract it”.14 Perhaps for this reason a final diagnosis was not reached and treatment begun for some months after presentation in many children. As early diagnosis and treatment does not affect long term outcome,15 parents can be reassured that most seizures do not cause brain injury and can be given first aid information about the management of events. Time is available if doubt remains.
What is already known on this topic
-
There is a wide differential diagnosis of paroxysmal events in infancy and childhood
-
The misdiagnosis of epilepsy is common
Comparing the current study with the series reported by Shinnar and colleagues,16 the proportion of children with generalised (54% in current study v 12% in Shinnar et al) and focal (37% v 63%) epilepsies differ markedly, and the proportions that were idiopathic (53% v 25%), probably symptomatic (30% v 49%), and symptomatic (17% v 26%) may reflect this. The number of children assigned a specific epilepsy syndrome diagnosis was more than for a recent series17 of children referred to a tertiary epilepsy centre (48% current study v 21% Kellinghaus et al). These disparities are likely to be due to demographic and referral pattern differences between the study populations.
EEGs were requested in accordance with regional guidelines that seek to halt the propensity for indiscriminate EEG requests for all “funny turns”. Perhaps as a result most children (84%) with a final diagnosis of epilepsy eventually had EEG corroboration. This has similarities with findings in adults in which interictal epileptiform abnormalities were detected in 50% of patients with epilepsy on the first recording, in 84% by the third, and 94% by the fourth,18 and suggests that repeated normal EEG should be a marker for re-evaluation of the diagnosis of epilepsy. MRI scanning showed significant advantages over CT in detecting underlying brain lesions. The high number of children having CT scans despite widespread acknowledgement that MRI scanning is the investigation of choice reflects a continued difficulty in obtaining MRI scans for children locally.
Non-epileptic events were most often syncopal, occurring in specific situations or after specific triggers. “When approaching the patient who has had a spell of unknown cause, the most important differential to make is between a syncopal episode and a seizure”.19 During syncope with loss of consciousness, multifocal or generalised myoclonus occurs in 90% of patients, and head aversion, oral automatism, upward eye deviation, and visual and auditory hallucinations are common.20 Our data illustrate that “reflex anoxic seizures” are not limited to the preschool age group. No cases of cardiac syncope were seen.
Unclassified events were common (14% of total). Some of the unclassified events in this study may have been benign epileptic seizures or non-epileptic events, but were not recognised as such either because of atypical presentation or lack of knowledge by the assessing clinician of all the minutiae of the differential diagnostic possibilities. Others may have been behavioural in origin—one mother acknowledged that after her child had been discharged from clinic she observed a few episodes but ignored them and they “went away”.
If the flawed but widely perceived dictum of treatment after one or two seizures was adhered to, some of these children may have been given a diagnosis of epilepsy and treatment with antiepileptic drugs. Such treatment would appear highly successful because the natural history of many of these events is for them to resolve spontaneously, irrespective of treatment. Paediatricians are used to not having all the answers and frequently give reassurance to parents about phenomena that they recognise to be benign and self-limiting but for which a cause is poorly understood, for example, infant colic, toddlers’ diarrhoea, growing pains. Unclassified events can be managed expectantly as long as a full initial assessment is performed, follow up is continued until the benign nature of the events is apparent, and there are agreed channels for parents to seek reassessment if the situation changes.
What this study adds
-
In this secondary care setting faints and other funny turns present more often than epilepsy by three to one
-
Unclassified events can safely be managed expectantly
Other non-epileptic events were common. The following were useful features in the evaluation of these events as opposed to epileptic events:
-
Events which were situational (i.e. occurred following specific triggers or during certain activities)
-
Events which could be interrupted
-
Events where the parents seemed to be seeking a diagnosis of epilepsy
-
Repeated EEGs (especially ictal) were all normal
-
There was continuing clinical doubt (watch and wait).
Improved local services for children with epilepsy have been recommended by a number of recent publications,21–23 and dedicated district epilepsy clinics, which concentrate care of children with epilepsy under a trained and interested team, are seen as one way of achieving this goal. According to a recent questionnaire (results unpublished), 77% of secondary paediatric services in the northwest of England now hold dedicated children’s epilepsy clinics; 30% of districts employ epilepsy specialist nurses to support these services. The consequences of a misdiagnosis of epilepsy are significant;24 improving dedicated care for children with “funny turns” is happening slowly and will reduce the potential for this misdiagnosis.
Acknowledgments
We acknowledge Fiona Ingham, full time volunteer Epilepsy Liaison Worker, for advice and support; Louise Dakin for secretarial help; and Margaret Roscoe, Senior Nurse, FFAFT clinic, for organisation and enthusiasm.
REFERENCES
Footnotes
-
Competing interests: none declared
Linked Articles
- Atoms
- Perspectives