Article Text

Abstract
Objective A significant proportion (15–30%) of patients with mild traumatic brain injury (MTBI) are at risk of developing postconcussional syndrome (PCS). The aim of this study was to investigate the contributions of cognitive, emotional, behavioural and social factors to the development of PCS and identify early predictors.
Methods A prospective cohort design was employed. 126 MTBI patients completed baseline questionnaire assessments within 2 weeks of the injury and 107 completed follow-up questionnaire assessments at 3 and 6 months. A series of self-report measures were used to assess cognitive, behavioural and emotional responses to MTBI. The primary outcome was the ICD-10 diagnosis for PCS. Demographic and clinical characteristic variables were compared between PCS cases and non-cases using independent sample t tests and χ2 tests. Individual and multivariate logistic regression analyses were used to detect predictors of PCS.
Results Of 107 MTBI patients, 24 (22%) met the criteria for PCS at 3 months and 22 (21%) at 6 months. Individual logistic regression analysis indicated that negative MTBI perceptions, stress, anxiety, depression and all-or-nothing behaviour were associated with the risk of PCS. Multivariate analysis revealed that all-or-nothing behaviour was the key predictor for the onset of PCS at 3 months while negative MTBI perceptions predicted PCS at 6 months.
Conclusions The study provides good support for the proposed cognitive behavioural model. Patients' perceptions of their head injury and their behavioural responses play important roles in the development of PCS, indicating that cognitive and behavioural factors may be potential targets for early preventive interventions.
Statistics from Altmetric.com
Introduction
Traumatic brain injury is one of the most common neurological conditions. Each year in the UK at least 1 million cases present to hospital emergency departments, of which 90% are actually mild traumatic brain injury (MTBI).1 Although the initial injury is mild, a significant proportion (about 15–30%) of MTBI patients are at risk of developing postconcussional syndrome (PCS).2–4 PCS is a term used to describe a constellation of ongoing physical, cognitive and emotional symptoms associated with MTBI. Because MTBI is associated with substantial ongoing disability and distress for patients, and high healthcare costs, identifying individuals who are at risk for developing long term sequelae post MTBI is important to both patients and healthcare professionals.5 There has been substantial interest in prognosis after MTBI but due to misclassification of MTBI, lack of control for confounding factors, non-representative samples and cross sectional study designs, identification of prognostic factors remains a priority for research. A call for better research in this area has been made by the WHO Collaborating Centre for Neurotrauma Task Force.5 6
Despite the research limitations, there is increasing recognition that PCS is best understood in terms of an interaction between biological, psychological and social factors.3 7 8 The evidence to date regarding psychosocial factors in the development of PCS suggests that premorbid psychopathology, comorbidity of anxiety and depression,7 9 negative illness perceptions,10 expectation11 and compensation/litigation12 are all potential risk factors. However, previous research is limited in that it has investigated either an individual risk factor in isolation or at best a limited subset of risk factors.
To provide theoretical guidance for our prospective design, we developed a model for PCS (illustrated in figure 1) which subsumes and integrates risk factors identified in previous studies and models of PCS.9 13–15 In accordance with models of other functional somatic syndromes such as chronic fatigue syndrome and irritable bowel syndrome,16 17 risk factors are characterised as: (1) predisposing factors: for example, people who have a premorbid personality trait of anxiety proneness and/or a history of somatic complaints are more vulnerable to develop PCS after MTBI; (2) precipitating factors: a brain injury, regarded as a double insult to both mind and body, triggers initial symptoms; and (3) perpetuating factors: cognitive, behavioural and emotional reactions to the injury may contribute to the persistence of symptoms. For instance, MTBI may provide a basis for the patients' beliefs/conviction (cognition) that they have a physical condition outside of their control. Some patients may tend to attribute their non-specific pre-existing complaints to the injury, misinterpreting these as negative consequences of the brain injury. Previous research has shown that this attributional style is associated with an all-or-nothing behavioural response to symptoms where patients overdo things when they believe symptoms are abating and then spend prolonged periods recovering when symptoms reappear. Both negative interpretations and all-or-nothing behaviour have been shown to be predictors of chronic ongoing symptoms.16 17 Emotional (eg, anxiety and depression) and social factors (eg, litigation and compensation) may also contribute to the persistence of PCS. We investigated PCS from this perspective which may provide new early intervention targets.

The proposed postconcussional syndrome (PCS) model.
The aim of this study was to identify the optimal early predictors for PCS following MTBI by investigating the contribution of cognitive, emotional, behavioural and social perpetuating factors in the development of PCS at 3 months and 6 months post MTBI. We hypothesised that patients with negative perceptions about their head injury, high anxiety and all-or-nothing behaviour may be at heightened risk of developing PCS. We also hypothesised that patients with low social support and those engaged in litigation would be at greater risk of PCS. While the WHO cautions against the use of PCS, it remains accepted in both International Classification of Disease, 10th revision (ICD-10) and Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV),18 and it is commonly used in clinical practice. Therefore, we have continued to use it in this study.
Methods
Study design and procedure
A prospective cohort design was employed. All participants were approached by research assistants in the emergency department at Southampton General Hospital in three blocks of 4 months between November 2008 and March 2010 and at different times of day to avoid selection bias. Those who provided written informed consent were either invited to the laboratory within 2 weeks after injury to complete a baseline questionnaire assessment or asked to return the completed questionnaire to researchers by post. Follow-ups to determine the incidence of PCS were conducted 3 and 6 months later via telephone assessment by researchers. This study was reviewed and approved by the Southampton and South West Hampshire Research Ethics Committee (B) (reference No: 08/H0504/106).
Participants
Potential MTBI patients aged between 18 and 60 years were initially identified by the emergency department. Eligibility criteria were checked via reference to their medical notes and verified via direct questioning by our research team based in the emergency department. Patients who met the MTBI criteria were recruited. The criteria used in the study were: a traumatically induced physiological disruption of brain function, as manifested by at least one of the following: (1) any loss of consciousness; (2) any loss of memory for events immediately before or after the accident; (3) any alteration in mental state at the time of the accident (eg, feeling dazed, disoriented or confused); and (4) lack of focal neurological deficit(s), but where the severity of the injury did not exceed the following: (1) loss of consciousness not more than 15 min; (2) an initial Glasgow Coma Scale (GCS) score of 13–15; and (3) post-traumatic amnesia not more than 60 min. These criteria were based on those defined by the Head Injury Interdisciplinary Special Interest Group of the American Congress of Rehabilitation Medicine.19 Participants were excluded if they suffered from multi-trauma requiring hospitalisation, major neurological or psychiatric disorders. Two hundred and ten patients were identified, of whom 126 completed the baseline assessment. Of these, 108 patients (86%) completed both follow-up assessments. One participant was excluded due to comorbid neurological conditions. Therefore, data from 107 patients were entered into the final data analysis (see figure 2).

Recruitment flow chart.
Baseline questionnaire measures
Demographic and clinical characteristics
A structured general information questionnaire determining the sociodemographic and clinical features of participants was administered at baseline.
Predictor variables operationalised from the model
Cognitive factors
The Brief Illness Perception Questionnaire (BIPQ) is a short measure of the key components of patients' perceptions of their illness, including consequences, timeline, personal control, treatment control, identity, coherence, concern, emotional response and causes.20 We adapted the BIPQ by replacing ‘illness’ with ‘head injury’. The treatment control item was omitted as treatment was not involved in most cases. The remaining seven items demonstrated satisfactory internal reliability in this study (Cronbach's α was 0.85), so the total BIPQ was used in the multiple logistic regression analysis. Higher scores represent more negative perceptions of head injury.
Behavioural factors
The Behavioural Response to Illness Questionnaire (BRIQ) was used to determine the effect of specific behavioural responses at the time of head injury. It is a valid and reliable measure, and the all-or-nothing subscale has been shown to predict the onset of chronic fatigue syndrome and irritable bowel syndrome following acute infection.17 21 The all-or-nothing subscale measures a pattern of over activity and then rest and includes items such as “I find myself rushing to get everything done before I crash” and “I have pushed myself as hard as ever until I cannot push myself any more”; the limiting subscale measures the extent to which patients rest and reduce activity in response to injury and include items such as “I have gone to bed during the day” and “I have avoided my usual activities”. Cronbach's α in this study was 0.85 for the former and 0.86 for the latter.
Emotional factors
The Hospital Anxiety and Depression Scale (HADS) is a well validated measure for detecting symptoms of depression and anxiety in medical populations.22 The HADS was found to have predictive value and clinical utility for the development of PCS symptoms by King.13 Cronbach's α in this study was 0.87 for the anxiety subscale and 0.86 for the depression subscale.
The Impact of Event Scale (IES) was used to evaluate current subjective distress related to MTBI by reflecting the intensity of the post-traumatic phenomena.23 The IES has been shown to predict PCS in previous research.13 The Cronbach's α in this study was 0.92.
Social factors
The Brief Social Support Questionnaire (SSQ) measures the number of perceived providers of social support for six common support scenarios, yielding two subscales which are SSQ availability and SSQ satisfaction.24 Both scales demonstrated internal consistency (0.94 and 0.92, respectively) in this study.
A structured general information questionnaire recording treatment and litigation issues occurring after the injury was also administered at the two follow-ups.
Outcome measures at follow-ups
The Rivermead Postconcussion Symptoms Questionnaire (RPQ) was used to assess PCS symptoms.25 26 The RPQ presents 16 of the most common published PCS symptoms and measures the degree to which they are more of a problem compared with premorbid levels using values of 0–4.
The RPQ was used to identify patients who met diagnostic criteria for PCS. Cut-offs derived from the diagnostic criteria for research in the ICD-10 for PCS (code F07.2) were used to dichotomise participants into probable PCS and probable non-PCS patients at 3 and 6 months after injury according to their scores on the RPQ.27 The ICD-10 criteria of PCS included a history of traumatic brain injury and the presence of three or more of the following eight symptoms: (1) headache; (2) dizziness; (3) fatigue; (4) irritability; (5) insomnia; (6) concentration; (7) memory difficulty and (8) intolerance of stress, emotion or alcohol.28
Statistical analysis
All analyses were conducted with SPSS V.18 (SPSS Inc). Demographic and clinical characteristics were compared between PCS cases and non-cases using independent sample t tests and χ2 tests as appropriate. Each cognitive, emotional and behavioural variable measured at baseline was entered into a separate regression analysis as a covariate with gender and age to ensure that any significant effects were independent of these potentially confounding variables, with PCS outcome entered as the dependent variable (coded 0 for ‘non PCS’ and code 1 for ‘PCS’) at both 3 and 6 months. Significant variables from the individual regression analyses were subjected to multiple logistic regressions modelling with PCS outcome entered as the dependent variable. Two stepwise backward logistic regression procedures were conducted to derive the model at 3 and 6 months. The likelihood ratio test was used to select predictor variables. Fit of the model was assessed by the Hosmer–Lemeshow ‘goodness of fit statistic’ for significance.29
Results
Demographic and clinical characteristics
A total of 126 MTBI patients completed the baseline assessment. The majority were white (118, 93%), with 4% (n=5) Asian and 3% (n=3) black; 54% (n=68) of participants were single and 46% (n=58) were living with a partner or spouse. Sixty-four per cent (n=81) of participants obtained education above A level and 36% (n=45) under GCSE. The mean GCS score was 14.97 (SD 0.17). More demographic and clinical characteristics are shown in table 1. To assess the representativeness of the sample, we also compared the 126 participants who returned baseline questionnaires with 84 who consented to participate but did not return questionnaires (mean age 32.73, SD 12.61; n=55 men, 65%). The analysis revealed a significant age difference between the two groups (t=−2.73, p=0.007), indicating non-responders were younger than responders. However, there was no significant gender difference (p>0.05).
Demographic and clinical characteristics of mild traumatic brain injury cases at baseline, postconcussional syndrome cases and non-cases at 3 and 6 months
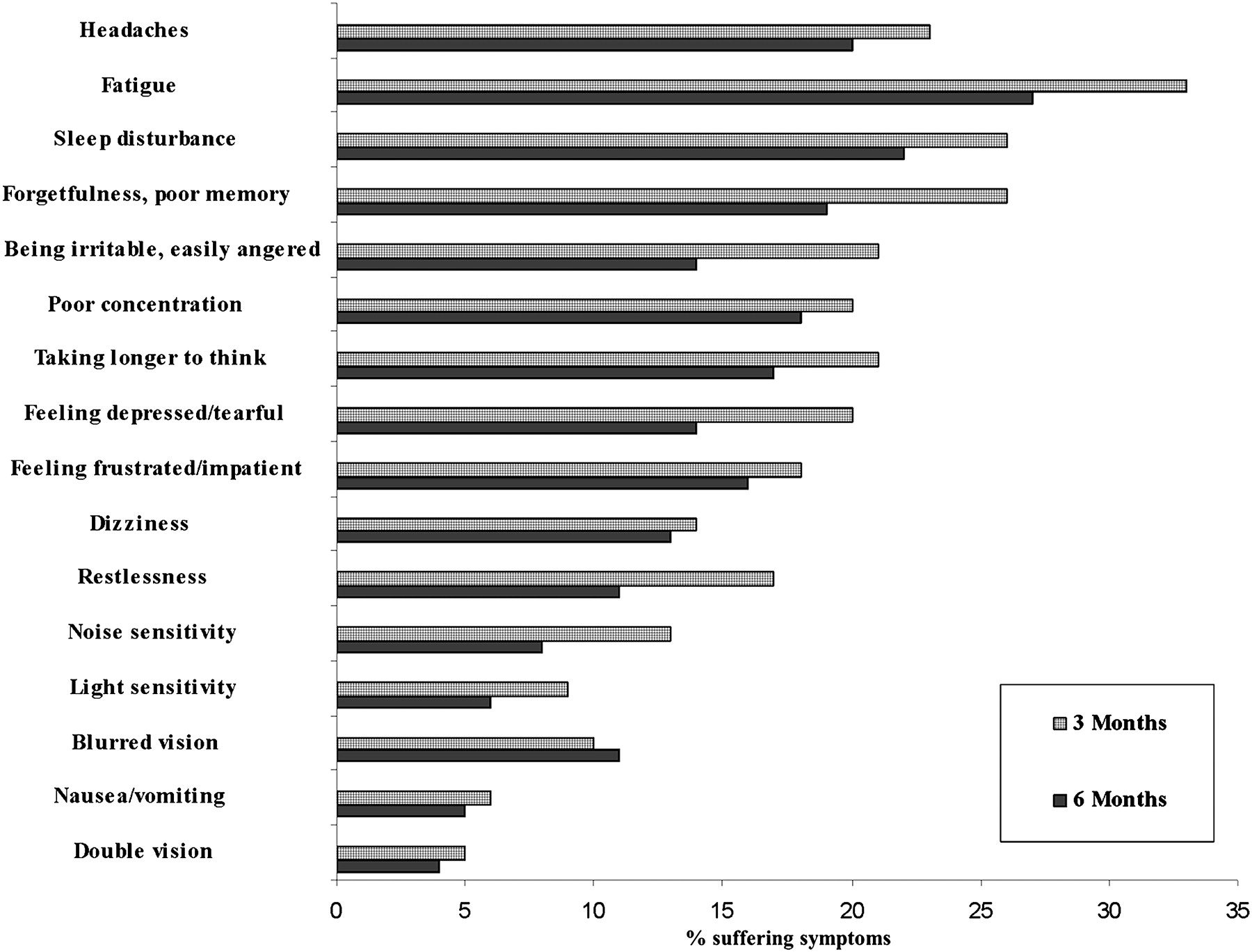
Data were available for analyses from 107 participants (85%) at both the 3 and 6 months follow-ups. The frequencies of PCS symptoms are presented in figure 3. A number of PCS symptoms were evident at both 3 and 6 months after MTBI. Headache, fatigue and sleep disturbance were the most commonly reported symptoms at 6 months whereas fatigue, forgetfulness and sleep disturbance were most commonly reported at 3 months. A total of 24 (22%) participants met the criteria for probable PCS caseness at 3 months and 22 (21%) of those remained probable PCS caseness at 6 months. The prevalence of PCS caseness at 3 months was very close to that at 6 months.

{kind=link}
{kind=link}
{kind=link}
The frequencies of postconcussional syndrome symptoms.
Table 1 shows key demographic and clinical characteristics of PCS cases and non-cases at 3 and 6 months. Data analysis showed no significant differences between PCS cases and non-cases with regard to gender (Pearson χ2(1, 107)=0.217, p=0.642) and age (t(106)=−1.186, p=0.238) at 3 months, and gender (Pearson χ2(1, 107)=0.366, p=0.545) and age (t(106)=−1.087, p=0.280) at 6 months. There were no significant differences between the PCS cases and non-cases at each time point on other demographic characteristics, such as education, occupation or marital status. Neither were there significant differences with regard to GCS score, amnesia or loss of consciousness (p>0.05 in all cases).
Contribution of cognitive, emotional, behavioural and social factors to the development of PCS
The individual binary logistic regression analyses used to examine the role of each of the cognitive, emotional, behavioural and social variables measured at baseline as risk factors in the development of PCS are presented in table 2. Three out of the eight variables were significant predictors at 3 months: negative head injury perceptions measured by the total BIPQ, anxiety by HADS anxiety and all-or-nothing behaviour by BRIQ. At 6 months, five of the eight predictors were significant predictors of PCS. These included the three predictors found to be significant at 3 months as well as stress measured by the IES and HADS depression. Social support and litigation did not predict the onset of PCS at either time point and nor did limiting behaviour.
Individual logistic regression analyses of cognitive, emotional, behavioural and social variables for the development of postconcussional syndrome at 3 months and at 6 months
When individual items of the BIPQ were investigated (see table 3), people who viewed their head injury as having a number of symptoms (illness identity), out of their control (personal control), lasting a long time (timeline) and having a serious impact on their life (consequences) were likely to develop PCS 3 months later. The pattern was similar for PCS at 6 months but emotional representations and concern were also significant predictors.
Individual logistic regression analyses of Brief Illness Perception Questionnaire for the development of postconcussional syndrome at 3 months and at 6 months
The significant predictors from the univariate regressions were entered as covariates into two separate logistic regression models using the backward stepwise method, with PCS outcomes at 3 and 6 months as the dependent variable (see tables 4 and 5). When negative head injury perceptions, anxiety and all-or-nothing behaviour were entered into the 3 month regression equation, all-or-nothing behaviour was the only predictor which remained significant in the resultant model. When negative head injury perceptions, anxiety, depression, stress and all-or-nothing behaviour were entered into the 6 month regression equation, only negative head injury perceptions and all-or-nothing behaviour were included in the resultant model, with negative illness perceptions being the only significant predictor and all-or-nothing behaviour a trend for significance. Overall, the 3 month model successfully predicted 76.4% of cases whereas the 6 month model successfully predicted 82.9% of cases.
Logistic regression (backward stepwise) of predictors for postconcussional syndrome at 3 months
Logistic regression (backward stepwise) of predictors for postconcussional syndrome at 6 months
Discussion
This prospective study investigated how cognitive, emotional, behavioural and social risk factors contributed to the development of PCS at 3 and 6 months after MTBI. The findings indicate that patients' all-or-nothing coping behaviour shortly after MTBI was the most important predictor of PCS at 3 months whereas patients' negative head injury perceptions were the most important predictor at 6 months. The study suggests that cognitive and behavioural responses to the head injury may be more important predictors than emotional and social factors in the development of PCS at 3 and 6 months after injury.
Prevalence of PCS and PCS symptoms
Previous research has reported considerable variation in the prevalence of PCS, ranging from 10% to 80% at 3 months.30 31 As assessed by RPQ and based on the ICD-10 diagnostic criteria, 22% of a whole sample of 107 patients were probable PCS cases at 3 months in this study, which is close to the 25% reported by Whittaker et al,10 and some previous estimates of 15% of individuals having PCS.3 32 33 However, this finding is relatively low compared with the 40–55% reported in recent studies in a Scandinavian population,14 34 35 possibly due to different severity levels of MTBI, as the mean GCS score was reported as 14.70 in one of those studies14 which is lower than that in this study (14.97). When our finding was reassessed at 6 months, the prevalence of PCS was 21%, which is similar to the 28% reported previously by Mittenberg and Strauman.36 We also found that there was no significant recovery of PCS from 3 to 6 months in the study population, which suggests that PCS symptoms persist during this period when no intervention is involved. In terms of the prevalence of symptoms (see figure 3), somatic symptoms were most prevalent, such as headache, fatigue and sleep disturbance, which is consistent with the study by Lannsjo and colleagues.15 The prevalence of PCS and PCS symptoms may help clinicians to have a clearer picture of prognosis after MTBI.
Role of perceptions of injury and coping behaviour
Consistent with Meares' study,37 unhelpful cognitive responses to MTBI are actually present early in the development of PCS. Patients' early negative beliefs about their head injury were found to be the only significant independent predictor at 6 months. This was also the first study to show that all-or-nothing behaviour in response to the acute injury also predicted the onset of PCS.
The significant role of negative illness perceptions is consistent with the previous study by Whittaker et al,10 and supports previous models and theory.3 7 38 In particular, patients who were at heightened risk of developing PCS tended to believe that their brain injury symptoms would last a long time (timeline) and have a negative impact on their life (consequences); they were also more likely to associate their head injury with a number of symptoms (illness identity) and to feel that they had little control over it (illness control). In accordance with Whittaker et al, beliefs about timeline and consequences of head injury were stronger predictors, indicating that these may be possible intervention targets. The predictive power of illness beliefs is stronger at 6 months than at 3 months, indicating that these beliefs may be reinforced over time. Comparatively, an initial response of all-or-nothing coping behaviour is a stronger predictor for PCS at 3 months. Findings were consistent with its role in similar functional somatic syndromes such as chronic fatigue syndrome39 and irritable bowel syndrome,17 which suggests that similar management approaches might be effective and could therefore be adopted.40
Contribution of emotional factors: anxiety and depression
In contrast with Dischinger's34 and Garden and Sullivan's findings41 which suggest that anxiety and depression are important predictors for PCS, measures of emotional factors failed to predict PCS when cognitive and behavioural factors were added to the model, although when considered individually, anxiety in particular was a significant predictor. Our finding is inconsistent with King's study13 where measures of emotional factors taken early after injury were found to be the best predictors of severity of PCS. This may be due to different outcome measures having been used in the two studies, where King looked at the severity of PCS using the total score of RPQ instead of categorical diagnosis, and to the use of different cognitive and behavioural measures. Ours was the first study to look at the relative importance of negative perceptions of injury and coping with symptoms when taking other factors such as mood and social support into consideration. The predictive power of emotional factors was not as strong as the cognitive or behavioural factors, suggesting that they might be secondary responses to injury perceptions and coping behaviour or that these cognitions and behaviours mediate the effects of mood on the onset of PCS. The impact of social support and the involvement of litigation/compensation were also examined, as the latter have been found to be the most consistent predictors of delayed recovery after MTBI.5 However, lack of perceived support was not associated with the onset of PCS, and the findings did not reveal the ‘litigation effect’ noted previously.12
Proposed model for PCS
This study provides support for the role of early perpetuating factors in the development of PCS. Consistent with our proposed model, despite similar minor head injuries, patients may respond differently. The initial behavioural response, such as an all-or-nothing behavioural pattern, is a stronger predictor at an early stage, however as beliefs about the injury are reinforced, they predict the outcome in the longer term. Therefore, an early intervention programme targeting patients' coping processes may minimise the impact of unhelpful beliefs and behaviours, reduce anxiety, prevent the development of PCS and improve clinical outcome after MTBI. An early intervention manual or booklet which provides information for coping with MTBI, included in the initial management strategies, may potentially benefit patients in the longer term.
Limitations
There are several limitations which should be taken into account when interpreting the findings of this study. (1) We recruited patients through the emergency department and many people with MTBI may not present to the hospital. (2) Although the follow-up rates were good, the initial response rate was relatively low. Thus the sample may not be representative of the whole MTBI population, and generalisation of the findings should be made with caution. (3) The primary outcomes were measured via telephone, rather than face to face interview. (4) All-or-nothing behaviour is a self-report of people's behaviour or indeed their perceptions of their behaviour. (5) There was no control group either without injury or with a non-head injury so it is difficult to conclude that it was the MTBI that triggered the ongoing symptoms. (6) The use of the term PCS to link long term negative outcomes to MTBI is under debate. It has been argued that PCS symptoms are not unique to MTBI but occur in chronic pain patients, other types of injuries and in healthy controls.5 11 42–45 Therefore, we have justified the use of PCS (see introduction) and assessed PCS with attention to possible contributing factors in this study. (7) While we looked at the role of head injury beliefs and behaviour in the acute phase, it is possible that, at different time points after injury, other ‘windows of vulnerability’ may emerge. Therefore, future research would benefit from the investigation of these risk factors at different time points to clarify their impact on the perpetuation of PCS.
Conclusion
An accurate understanding of the biological and psychosocial factors in the development of PCS at various time points after injury is crucial to guide clinical management.46 We believe this is the first prospective study to investigate the impact of early cognitive, emotional and behavioural risk factors considered together on the development of PCS based on a proposed model. To date, there is no scientifically established treatment for PCS. An early intervention programme, using a cognitive behavioural approach, targeting patients' illness perceptions and coping behaviours may potentially prevent the development of PCS. Research to assess the effectiveness of such an intervention is warranted before it could be applied in clinical practice.
Acknowledgments
The authors thank Dr Valentina Di Pietro, Sarah McVeigh, Zeynep Ayse Sunbay, Kin Tong Chung and Emma Roger for their contribution to the process of data collection. They would also like to thank Mr David Culliford, medical statistician-NIHR Research Design Service South Central, who provided valuable statistical advice and support, the Wellcome Trust Clinical Research Facility at Southampton General Hospital for providing assessment facilities.
References
Footnotes
Funding This study was funded by the Faculty of Medicine Research Management Committee at the University of Southampton (grant reference code: 503836112).
Competing interests None.
Ethics approval This study was reviewed and approved by the Southampton and South West Hampshire Research Ethics Committee (B) (reference No: 08/H0504/106).
Provenance and peer review Not commissioned; externally peer reviewed.