Article Text

Abstract
Objective Vascular endothelial growth factor (VEGF) plays an essential role in the pathophysiology of polyneuropathy, organomegaly, endocrinopathy, M-protein and skin changes (POEMS) syndrome. Anti-VEGF antibody (bevacizumab) appears to be an attractive therapeutic option. The aim of this study is to investigate the effects of bevacizumab for patients with POEMS syndrome.
Methods We reported six POEMS patients treated with bevacizumab and reviewed the literature.
Results The serum VEGF levels decreased immediately after bevacizumab administration in all six patients. However, four patients had entirely no clinical response, and two of them died. The remaining two showed improvement that could be explained by combined treatments. We also reviewed the literature and found 11 patients treated with bevacizumab; of these, only one was treated with bevacizumab alone. 10 had combined treatments, and four died without any response.
Conclusions Both our experience and the literature suggest ambiguous effects of bevacizumab; inhibition of VEGF alone may be insufficient because multiple cytokines are upregulated, or aberrant neo-vascularization may have already fully developed in the advanced stage of POEMS syndrome.
- HAEMATOLOGY
- NEUROPATHY
Statistics from Altmetric.com
Introduction
Polyneuropathy, organomegaly, endocrinopathy, M-protein and skin changes (POEMS) syndrome is a rare systemic disorder associated with plasma cell dyscrasia, but is increasingly recognised as an important cause of demyelinating neuropathy.1–3 The syndrome is characterised by polyneuropathy (P), organomegaly (O), endocrinopathy and oedema (E), monoclonal gammopathy (M) and skin change (S). The serum level of vascular endothelial growth factor (VEGF) is markedly elevated in POEMS syndrome patients, and is a useful diagnostic biomarker and the best measure of the disease activity.1 Whereas high dose chemotherapy with autologous peripheral blood stem cell transplantation has significantly improved peripheral neuropathy and other symptoms of POEMS syndrome in the past decade,2 ,3 there is a subgroup of patients who are not indicated for transplantation because of organ failure or advanced age.
Many symptoms in POEMS syndrome such as capillary leak syndrome (pleural effusion, ascites and peripheral oedema), organomegaly and skin agiomata can be explained by a strong action of VEGF on neo-vasculisation and increased vascular permeability. Therefore, anti-VEGF monoclonal antibody, bevacizumab, is a theoretically promising treatment option, but the results of previous reports were very mixed and the efficacy of bevacizumab on POEMS syndrome is highly controversial.4–7 To determine the effects of bevacizumab, we report six patients treated with bevacizumab, and reviewed such cases in the literature.
Methods
Between 2005 and 2012, six of the 50 patients with POEMS syndrome, seen at the Chiba University Hospital, Japan, were treated with bevacizumab (table 1). The six patients were treated with bevacizumab because of insufficient response to previous therapies. There were four men and two women, aged 43–71 years (median 61 years). Two cases were previously reported.8 ,9 All fulfilled diagnostic criteria of POEMS syndrome3 ,10 and had a high serum VEGF level measured by ELISA (>600 pg/ml). We gave one course of 5 mg/kg bevacizumab, and examined clinical symptoms, serum VEGF levels, and chest/abdomen CT serially before and 2, 4, 8, 12 and 26 weeks after bevacizumab injection. Neurological symptoms were evaluated with the overall neuropathy limitation scale. The ethics committee of the Chiba University School of Medicine approved this study, and we received patient consents. We also searched Medline (January 2000 through December 2012) for case reports and case series of bevacizumab therapy for POEMS syndrome.
Profiles of patients with treated with bevacizumab
Results
Our case series
At the time of bevacizumab treatment, the disease duration ranged from 10 to 68 months (median 51 months), and all six patients had been already treated by other agents such as corticosteroids, melphalan, vincristine or thalidmide (table 1). These previous therapies were not sufficiently effective; five of the six patients were bed-bound because of severe polyneuropathy and massive plural effusion/ascites. Their serum VEGF level was still elevated (range, 601–4670 pg/ml) before bevacizumab treatment.
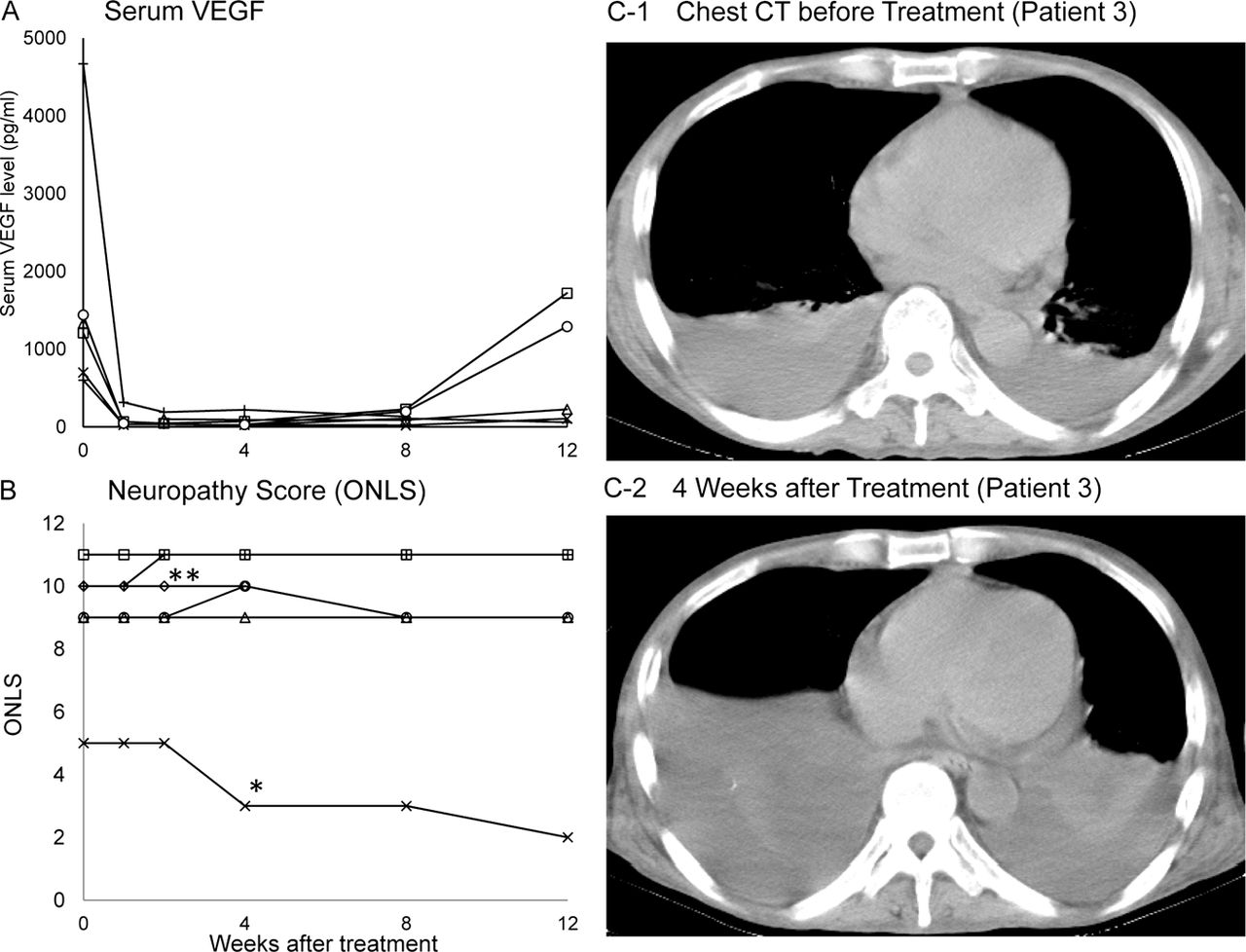
After bevacizumab therapy, serum VEGF levels dramatically decreased (range, 46–190 pg/ml) 2 weeks later, and remained low 8 weeks later (figure 1A). VEGF levels returned to the pretreatment level at Week 12 in two patients, and at Week 16 in four patients. The treatment resulted in entirely no response in four (Patients 3–6 in table 1), and two of them died of multiorgan failure due to massive and intractable pleural effusion, 6 and 2 months later respectively. Patients 1 and 2 showed a gradual decrease in peripheral oedema and pleural effusion over months, but the effects were likely to be explained by thalidomide/dexamethasone therapy because the changes in clinical and laboratory findings started after the treatment and 8 weeks after bevacizumab injection. The scores of overall neuropathy limitation scale and inflammatory neuropathy cause and treatment did not change in five patients (figure 1B). No serious adverse effects by bevacizumab were observed.
{kind=link}
Serial changes in serum levels of vascular endothelial growth factor (VEGF; A), overall neuropathy limitation scale (ONLS; B) and chest CT (C) after bevacizumab administration. The serum VEGF levels dramatically decreased. However, ONLS score did not change entirely in five of the six patients and pleural effusion rather increased on chest CT in Patient 3 (table 1A). *Patient 1 underwent auto blood stem cell transplantation 47 days after bevacizumab. **Patient 6 died 43 days after the treatment. The ONLS score in Patient 3 was 11 at the baseline and 12 weeks later.
Literature review
We found 11 cases of bevacizumab treatment for POEMS syndrome (table 1B).4–6 11–17 Of these, seven patients eventually had improvement in neuropathy and systemic symptoms, but six of them received previous or combined treatments. In only one patient with subacute onset of polyneuropathy (Patient 1 in table 1B)11 bevacizumab was administered as an initial and single therapy, resulting in improvement in neuropathic symptoms within 4 weeks. Bevacizumab appeared to be effective in this patient. In Patients 2 and 3 (table 1B), serum VEGF levels were normalised after irradiation before bevacizumab injection.12 In Patient 4 (table 1B), haematological remission was achieved by melphalan treatment, before bevacizumab administration. Therefore, it is difficult to conclude that bevacizumab had beneficial effects in these patients. The remaining patients (nos 5–11; table 1B) received combined treatments, and three of them died without any response to bevacizumab.6 ,16 ,17
Discussion
Both our experience and the literature suggest ambiguous effects of bevacizumab on POEMS syndrome. Bevacizumab therapy results in a rapid decrease in the serum VEGF levels, but this was not necessarily associated with clinical improvement. The large biological and clinical heterogeneities of POEMS syndrome could explain variable sensitivities to anti-VEGF therapy. Furthermore, because of the lack of standard treatment regimen for POEMS syndrome, many patients had received multiple treatments as shown in table 1.
Of our six patients, bevacizumab was obviously ineffective in four, and in the remaining two it was difficult to determine the effects because of multiple treatments. In the literature, only one of the 11 patients had a single treatment with bevacizumab in the very early phase of the disease,11 and the drug appeared to have positive effects in this patient. However, the efficacy was not justified in the remaining patients. It should be noted that two of our six patients, and four of the 11 reported patients died several months after bevacizumab injection.
There are several hypotheses for the failure of bevacizumab treatment. First, in POEMS patients, VEGF and several other cytokines, such as interleukin-6 (IL-6), IL-12, tumour necrosis factor-α and hepatocyte growth factor, are elevated,18–20 and inhibition of VEGF alone is not sufficient to suppress the disease activity. Second, during the long course of the disease, aberrant angiogenesis has already systemically developed, and the structural changes may result in permanently leaky vessels. Under these conditions, reduction of VEGF may not be enough to induce obvious clinical improvement. Some researchers also suggest that sudden VEGF removal may cause sudden collapse of newly formed fragile vessels because VEGF is an important factor for new vessels, and may lead to an increase capillary leakage.6
Buxhofer-Ausch et al12 proposed that the short disease duration before bevacizumab initiation may be an important factor for a good outcome. We agree with that bevacizumab may be efficacious in the very early phase of the disorder when abnormal neo-vasculisation has not been fully developed. We also suggest that the standard or first-line treatment for POEMS syndrome should target plasma cell dyscrasia, and that temporary relief of symptoms by VEGF-targeted therapy would not be effective in many of the patients with long-standing POEMS syndrome.
Acknowledgments
This work was supported in part by the Health and Labour Sciences Research Grant on Intractable Diseases (Neuroimmunological Diseases) from the Ministry of Health, Labour and Welfare of Japan (SK).
References
Footnotes
-
Contributors YS, SM and SK designed the research and wrote the manuscript. KS, SN, SM, YI, MB, SS, SI, SH and CN collected and analysed data. All authors approved the final draft of the paper.
-
Funding The Health and Labour Sciences Research Grant on Intractable Diseases (Neuroimmunological Diseases) from the Ministry of Health, Labour and Welfare of Japan.
-
Competing interests None.
-
Patient consent Obtained.
-
Ethics approval Ethics Committee, Chiba University School of Medicine.
-
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial commentary