Article Text

Statistics from Altmetric.com
Case summary
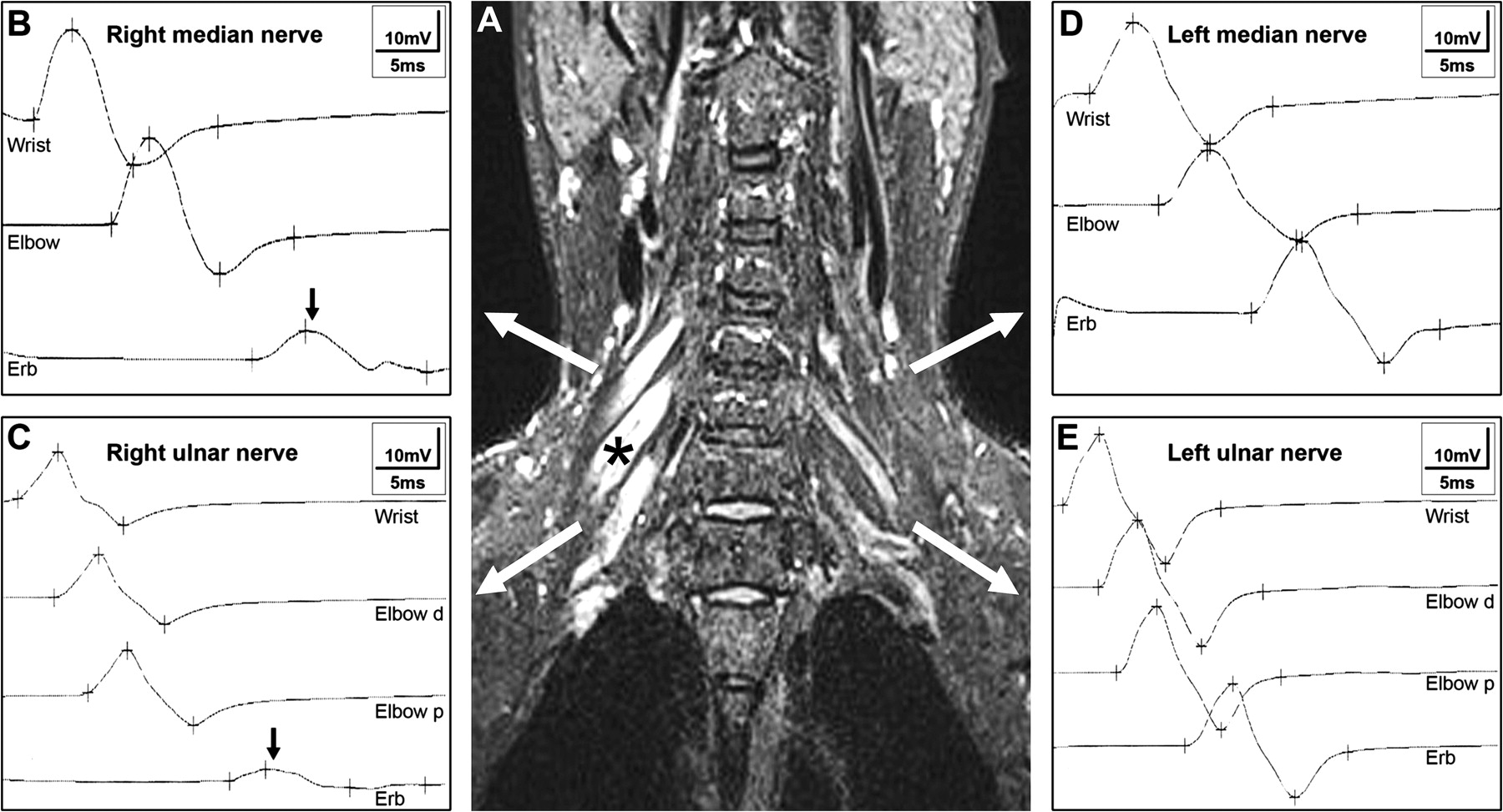
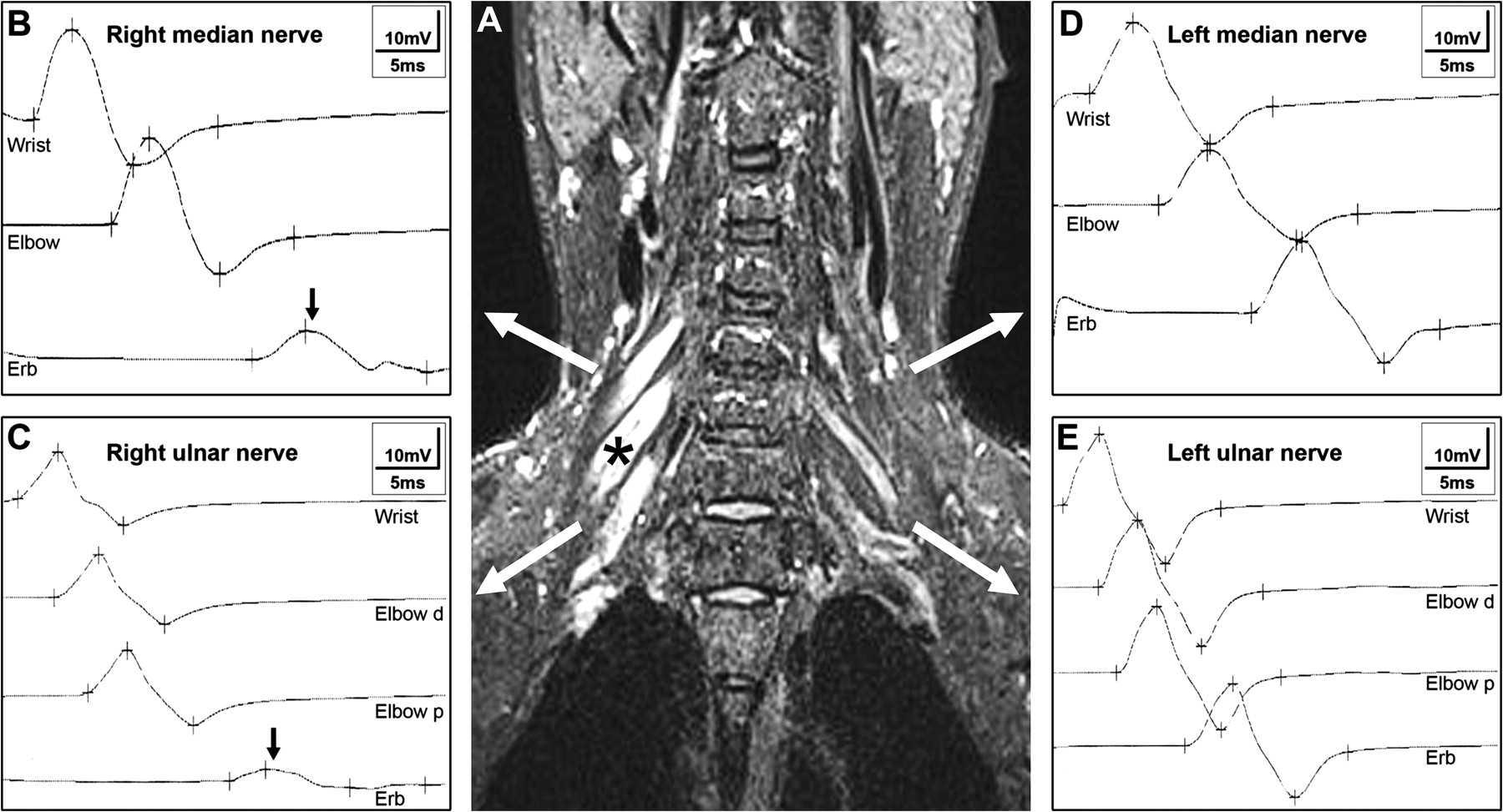
A 45-year-old man presented with 3 months of progressive right hand weakness. Examination showed mild atrophy and weakness of the right hand, and absent tendon reflexes. Cerebrospinal fluid contained 0.42 g/l protein (normal <0.45) and 1 lymphocyte/mm3. Electrodiagnostic studies revealed a multifocal motor neuropathy (MMN) with partial conduction blocks and severe denervation in the muscles of the right hand (figure 1). Sensory nerve conduction studies were normal. Charcot–Marie–Tooth disease, distal demyelinating polyneuropathy associated with monoclonal gammapathy, Lyme disease, lymphoma and malignant plasma cell dyscrasia were excluded using relevant biological, electrophysiological and genetic studies.1 The search for IgM anti-ganglioside GM1 (anti-GM1) antibodies using ELISA was positive. Coronal short tau inversion recovery MRI assessment of the brachial plexus demonstrated diffuse enlargement and abnormally high signals in the right brachial plexus (figure 1). The patient was diagnosed with definite MMN based on the European Federation of Neurological Societies/Peripheral Nerve Society guidelines and treated with intravenous immune globulin for 6 months.2 Right hand strength gradually improved.
{kind=link}
(A) Coronal short tau inversion recovery MRI demonstrates diffuse enlargement and abnormally high signals at the level of the trunks in the right brachial plexus (asterisk). Electrodiagnostic studies reveal partial conduction block in the right median and ulnar nerves, localised between the elbow and Erb's point (B, C; black arrows). No blocks are observed in the left median and ulnar nerves (D, E).
MRI assessment of brachial plexus in MMN usually demonstrates swelling and increased signal intensity.3 The increased signal intensity is believed to be due to demyelination, while inflammation and oedema might lead to swelling in nerves.3 In a few cases, high signal intensity has been shown to co-localise with conduction block in the brachial plexus and in the forearm segment of the arm.4 5 MRI is considered to be of help to differentiate MMN from lower motor neuron disease, with brachial plexus MRI being normal in the latter.1
In our patient, MRI abnormalities corresponded exactly with the symptoms and with partial conduction blocks.
Footnotes
Competing interests None.
Patient consent Obtained.
Ethics approval This study was conducted with the approval of the Strasbourg University Hospital Ethics Committee.
Provenance and peer review Not commissioned; externally peer reviewed.