Article Text

Abstract
The call to the bedside and the prognostication of a comatose patient—telling family members what to expect—commonly falls to neurologists. The assessment is often confounded by the treatment paradigms of modern intensive care (ie, drugs, drug interactions and targeted temperature management). Patients may be too unstable to leave the intensive care unit for neuroimaging; thus, repeated clinical examinations are decisive. Despite diverse causes, certain principles do apply: (1) Many patients can improve, although with significant abnormalities; (2) Neuroimaging and electrodiagnostic tests can help but are rarely definitive; (3) Secondary involvement of the upper brainstem marks a tipping point with much lower probability for an independent outcome; (4) We rarely predict mortality or diagnose brain death; usually the major concern is anticipated neurological deficits; and (5) Prior comorbidity and permanent organ dysfunction are critical factors in making decisions about de-escalation or escalation of care. This review provides a practical approach to evaluating outcome of a comatose patient. Prognostication is difficult, and we should only attempt it when the diagnosis is confirmed and appropriate (often aggressive) medical or surgical treatment has been tried.
- COMA
- cerebral oedema
- consciousness
- persistent vegetative state
- stroke
Statistics from Altmetric.com
Introduction
We, as the neurologists, have all been asked to see ‘unresponsive’ patients immobile in bed, on a ventilator, doing nothing, with no movement, no grimace except for an occasional twitch and, when eyes are opened, a blank stare. What do we say? What can we say? We do not want to ‘write the obituary’ for a patient who might be sitting in a chair the next day. (‘Have you seen Mr. Taylor? You won’t believe it!’) We do not want to tell families not to lose hope (or worse, that ‘time will tell’) when we are pretty convinced that the status will not change for the better. We cannot (and should not) provide escalating intensive care to a patient who, because of a significant injury, is in devastatingly poor shape or even imminently close to brain death.
Any neurologist will approach these patients with trepidation because we seldom know enough about their circumstances; their hospital course has been long and complicated, and prior (sometimes critically essential) details are hard to find in the records. Prognostication of coma is difficult; truly it is. Algorithms are inherently artificial, lack the necessary precision and performance and never account for all those confounders (drugs, drugs, drugs) and medical illness, either present or intercurrent. Many new guidelines are derivatives of older ones and the parameters have not changed, only their interpretation. This review is an amalgamation of literature review and opinions, as well as an attempt to establish some procedure to address the questions. The neurologist’s prognostications are not scientific instruments. Neurology is not like that.
Definition of coma
A traditional, but simple and useful distinction, is to separate states by the degrees of wakefulness and awareness (figure 1). This distinction allows us to separate coma from a persistent vegetative state (and severe forms of minimally conscious state, MCS). Coma denotes being unaware and not awake. Clinicians have gone farther in describing a comatose patient, and this includes descriptions of eye movements (absent fixation or finger tracking), motor responses (absent localisation or reflexive movements) and no verbal output but of no significance in many instances, because comatose patients are intubated to protect the airway. Attempts to categorise coma into several grades of severity have proven futile unless the evaluation takes into account the absence of one or more brainstem reflexes. An important clinical fact is that most patients in coma recover and become more awake. Prolonged disorders of consciousness, such as a vegetative state or MCS, are, therefore, rarely seen after the first year of the injury. It is also a real possibility that patients were misdiagnosed and misclassified after being admitted to neurorehabilitation centres or nursing homes.1
Researchers have subclassified MCSs into those with (MCS+) or without language (MCS–); those with language are more likely to improve further. The classification becomes less articulate since functional MR scan-based categorisation has identified a patient subset fulfilling all vegetative state criteria but in whom functional MR showed a command-following response. Doing or asking something to the patient creates brain activation maps. Another patient subset, higher order cortex motor dissociation, shows a cortical response to the auditory stimuli, again without evident awareness.2 Similar observations have been made with EEG power spectral analysis both early3 and late4 in the clinical course. EEG responses to spoken simple one-task commands were variable among the small group of patients who responded. Responses on EEG spectra and MR cannot (yet) be seen as proof of awareness and may cause considerable disquiet if deciding family members interpret them as such. More importantly, neurologists do not seem to know how to channel these research observations into the practice of prognostication.

Definition of coma and vegetative state.
Once coma is diagnosed, any clinician will seek an explanation, and in most cases, the explanation can be found through neuroimaging, electrophysiology or cerebrospinal fluid evaluation. It is uncommon to still have a patient with an unexplained coma 24 hours after the admission. When confronted with such an unresolved situation, the neurologist should seek a less common cause, such as an undetected toxin or prolonged, unrecorded hypoglycaemia or anoxia. Emergency departments, worldwide, see coma from opioids, anoxic–ischaemic injury after cardiopulmonary resuscitation, traumatic brain injury, status epilepticus, acute central nervous system (CNS) infections and rapid multiorgan failure. Psychiatric causes for coma do exist, but they are not of long duration. They are quite rare, declare themselves quickly and are not further considered. Extreme forms of catatonia (previously known as lethal catatonia) require a careful assessment and often a search for autoimmune encephalitis. We can safely say that most comas originate from neuronal depression due to intoxication, acute metabolic or endocrine derangement or a lesion in crucially important brain structures. In the case of a structural brain injury, the affected structures are the bilateral cortex or white-matter connections to the cortex, thalamus, dorsal pons and midbrain containing the fibres of the ascending reticular activating system. Acute coma will involve each of these structures. Deepening or emerging coma from a lesser state of impaired consciousness can result from a unilateral lesion displacing other structures from mass effect and causing those structures to become dysfunctional, either from a pressure effect or through ischaemia when the feeding arteries are threatened.
Neuroimaging, frequently just a CT scan by itself, often establishes the cause. MRI becomes exceedingly important in the workup of a patient when the cause cannot be established. For example, it may show posterior reversible encephalopathy syndrome not clearly imaged on CT scan and any of the more severe leucoencephalopathies associated with illicit drug use. Patients rarely go into non-convulsive status epilepticus ‘out of the blue’; usually, there are clinical signs pointing to it (blinking, eye deviation and jaw twitching). In any patient in whom the EEG shows epileptiform activity, further monitoring might be necessary. We all think of it, hoping that it is the cause, but we very rarely diagnose non-convulsive status epilepticus clinically or electrographically—despite consulting on a large volume of patients admitted to medical or surgical intensive care units with no prior neurological injury. Other studies have claimed higher percentages (still less than 10%) in comatose patients treated for a critical illness but without a proven effect on outcome after treatment. Transformation of generalised convulsive status epilepticus to non-convulsive status epilepticus is far more common and eminently treatable.5
Before we can prognosticate, we must diagnose the condition. Wrong diagnoses lead to incorrect prognoses (but not always). Much may be said for experience. Indeed, some studies suggest that seniority of staff boosts chances of survival, but careful assessment of all possible variables remains key.6 7 Additionally, before we prognosticate, we must consider all potential (including aggressive) treatments. No neurologist should entertain an outcome prediction if the results of a medical or surgical treatment are not yet known. An additional important, seldom mentioned or acknowledged factor is the early recognition of the cause of coma. Outcome has to be linked to time of intervention and acting quickly. Untreated hydrocephalus, prolonged pressure effect from a mass, untreated large-vessel occlusion and untreated (or inadequately treated) seizures or infection can all impede recovery. There are several situations where timely and aggressive treatment may lead to substantial recoveries. These recoveries may surprise the uninitiated but should not surprise the experienced neurologist (box 1).
Ten ‘surprising’ coma recoveries
Acute meningitis (treated).
Acute subdural haematoma (evacuated).
Acute hydrocephalus (drained).
Intoxications (antidotes).
Non-convulsive status epilepticus (antiepileptic medications).
Uraemic encephalopathy (dialysis).
Posterior reversible encephalopathy syndrome (lowered blood pressure).
Myxoedema coma (thyroid supplement).
Basilar artery embolus (clot retrieval).
Accidental hypothermia (warming).
Principles of prognostication in coma
Accurate prognostication is based on good judgement, and the key to good judgement is good evaluation of all the information. In some situations, it is coming to terms with it; in others, it is better to deflect a request to make a final decision. The main principles in assessing the patient in prolonged (>24 hours) coma are (1) to examine and identify what counts; (2) to review neuroimaging and know what matters; (3) to evaluate laboratory tests and ancillary tests to see what is missing; (4) to find confounders and consider contributing factors that might have been forgotten; (5) to decide and acknowledge inevitable uncertainties; (6) to factor in the bigger picture (ie, the patient’s previously stated wishes regarding independence and comorbidity); (7) to refrain from predictions if all too confusing; (8) to proceed with a brain-death examination to declare a patient brain dead (the deceased have no prognoses); (9) to speak candidly with family members in a scheduled conference with all medical stakeholders and (10) to proceed with an agreed-on de-escalation plan or withdrawal of support when the best time has been identified. This may help to answer the most commonly asked questions (ie, what is the likelihood that patients will die or remain in an absolutely hopeless condition whatever we do? How far should treatment go?)
Prognosis by disease categories
It is important to confirm the manner in which the brain has been injured and to identify important and clinical and laboratory data specific to certain disorders. These prime indicators of outcome are critical to an accurate prognosis. Neurologists are often (and undeservedly) mislabelled as harbingers of doom or nihilists, but our goal is to distinguish between the situations that are futile and situations in which the patient has a ‘fighting chance’ (often, when others are ready to give up) and may gain some state of self-reliance. But prognostication for full recovery after a major neurological injury leading to coma continues to elude us.
Coma and traumatic brain injury
In the elderly, any major traumatic brain injury resulting in coma generally has a poor outcome. Age remains the most important determinant and most indicative variable.8–10 Prognostication in the case of a young adult with a traumatic brain injury is difficult.11 Traumatic brain injury in younger persons (<40 years) remains a ‘roll of the dice’ probability in any multicentre, large-database model.10 While many awaken, survive and improve to the point of walking, talking and taking care of basic needs, their recovery is often accompanied by depression, new addictions, epilepsy and emotional instability. Certain variables, including prolonged severe hypotension and anoxia during injury or during transport to hospital, light-fixed pupils or extensor motor responses, move the needle somewhat but not enough to claim these models as clinical bedside aids. Neuroimaging is seldom definitive, but the presence of primary traumatic brainstem lesions on neuroimaging consistently indicates a poor prognosis12 (figure 2). Similarly, MR-confirmed lesions of the genu of corpus callosum correlate with severe disability. Each of these lesions represents major flexion–extension tearing injuries to the parenchymal structures.

Primary brainstem trauma with basal ganglia contusion.
Another determinant is sustained, increased intracranial pressure, and we can expect this to lead to a shift of the brain tissue, displacement of the thalamus and midbrain, and a change in pupil size and light responses. Decompressive hemicraniectomy as a treatment for intractable increased intracranial pressure results in a 6-month postoperative mortality rate around 30% but with no measurable effect on the severity of morbidity.13 14 Traumatic brain injury with evacuation of a contusion or epidural or subdural haematoma may lead to protracted recovery. Despite adequate removal of the subdural hematoma, patients may take weeks to improve, and many need close EEG monitoring for seizures.15
In any patient with traumatic brain injury, physicians should watch for the presence of paroxysmal sympathetic hyperactivity. Physicians unfamiliar with this complication may consider these manifestations a mere epiphenomenon of severe brain injury. Paroxysmal sympathetic hyperactivity (‘storming’) after traumatic brain injury is often associated with a worse neurological outcome with longer rehabilitation stays and more cognitive impairment. Paroxysmal sympathetic hyperactivities are rapid and episodic manifestations of excessive sympathetic activity (tachycardia; hypertension with increased pulse pressure, tachypnoea, fever spike and diaphoresis; and increased muscle tone assuming extensor or dystonic postures). An effective treatment is intravenous morphine, scheduled doses of clonidine and increasing doses of gabapentin. It is very uncertain whether aggressive early treatment of these storming episodes affects long-term outcome.
Coma and anoxia
Coma after resumption of circulation following cardiopulmonary resuscitation has been associated with and explained by severe anoxic–ischaemic injury to the cortical mantle, thalamus, striatum and globus pallidus. Outcome predictions were, for many years, based on a prospective study of the findings on neurological examination and, more importantly, improvement over time.16 17 The distinctions proposed by Levy et al were too clinically useful to dismiss and shifted the conversation.16 Suddenly, 3 days seemed enough (and could be enough) to ascertain whether the patient had a chance to improve. However, a later study found less certainty with this time interval.18 The American Academy of Neurology practice parameter identified poor prognostication but only in a small group of patients.19 We hope no physicians consider employing the 3-day cut-off in these patients without persistent loss of brainstem reflexes or other very good reasons that lead them to doubt the possibility of improvement.
Prognostication in coma after cardiopulmonary resuscitation has been studied extensively in recent years and led to the 2014 European Resuscitation Council/European Society of Intensive Care Medicine Guideline.20 Several factors clearly determine a poor prognosis. These include early anoxic brain swelling, an indication of severity (figure 3); diffuse cortical restriction on diffusion-weighted MR scan of brain; absent cortical somatosensory evoked potentials; rising serum neurone-specific enolase21; unreactive and burst–suppression EEG patterns or marked suppression to less than 20 µV,22 burst–suppression EEG time locked with myoclonus status and refractory status epilepticus after CPR (with or without clinical manifestations and with or without myoclonus status).

Brain oedema after severe anoxia.
There are exceptions, and there are late recoveries with variable outcomes.23–25 However, these occur too infrequently to affect decision-making in this category of patient. Prognostication was perhaps ‘simpler‘ in earlier days of examining patients after a successful cardiopulmonary resuscitation—now, confounders (mostly hypothermia but also a slew of intravenous drugs to support the intervention) are very significant. Drug washout in a severely afflicted patient with associated kidney and liver injury during cardiopulmonary resuscitation remains very difficult to assess and cannot be predicted. Conspicuously lacking in many studies on outcome is information about the neurological examination, use of sedation, neuroimaging and postresuscitation haemodynamic and organ function, which many of us consider crucial in deciphering these patients’ prognoses. Caution is key, and the decision to address the level of care (and what can help the patient) may still have to wait or be regularly revisited.
Coma and stroke
Both haemorrhagic stroke and ischaemic stroke are heterogeneous disorders, and thus, prognosis is very disease specific.26–28 Coma after a parenchymal (lobar or deep ganglionic) haemorrhage denotes shift from a large-volume destruction of the thalamus or trapping of the ventricle causing obstructive hydrocephalus. Another factor influencing prognosis is the expansion of the clot volume due to anticoagulation.
Prognosis in a patient with a deteriorating lobar haematoma depends on whether evacuation is entertained, feasible or delayed. Rapid improvement with resolution of shift attests to that observation. Deep-seated haematomas (putamen and caudate thalamus) cannot be reached surgically, and even placement of a ventricular drain with use of thrombolytic drugs does not improve outcome.29
Haemorrhage in the cerebellum or pons is much less common. Cerebellar haemorrhage with CT evidence of a tight posterior fossa (obliteration of cisterns, tissue displacement upward or downward and tonsillar herniation) will lead to rapid loss of brainstem reflexes without emergent evacuation. Once evaluated, the outcome can be quite good because stance and gait are more affected by injury to efferent fibres than cerebellar structures. Pontine haemorrhages causing coma rarely (if ever) resolve to improvement in functional status and most certainly when they additionally damage the thalamus due to upward extension.30
Coma from ischaemic stroke is based on similar principles. Shift from oedema will not be tolerated unless relieved by a decompression. Haemorrhagic conversion of a large ischaemic stroke does increase mass effect and is a major additional determinant in outcome (figure 4). In a haemispheric stroke (ie, middle cerebral artery), outcome is poor when a decompressive craniectomy is not considered or when performed in the elderly (>60 years).31 32 Early versus late decompressive surgery also influences outcome, and the preponderance of evidence suggests that early decompression before the patient develops clinical signs of deterioration from brainstem involvement will help more. Bithalamic infarcts (from the top-of-the-basilar artery clot) are associated with coma at presentation, but patients may awaken, often after a period of marked fluctuation in alertness. An acute embolus to the basilar artery is devastating (causing infarction of the pons, midbrain and cerebellar haemispheres). Endovascular retrieval of a clot has a high success rate if the admission CT scan is normal. An embolus in the basilar artery that causes coma or locked-in syndrome (caveat non-neurologist) is associated with high mortality and no functional recovery, but there is a chance for substantial recovery if the clot is retrieved.

Haemorrhagic infarct with mass effect.
Prognostication in aneurysmal subarchnoid hemorrhage is largely unreliable - even in patients who appear moribund soon after the rupture. A comatose patient with aneurysmal subarachnoid haemorrhage can improve rapidly within hours after placement of a ventriculostomy and removal of a temporal lobe clot associated with middle cerebral artery aneurysm. However, if upper brainstem reflexes remain lost after this ‘cerebral resuscitation’, recovery rarely occurs. In many cases, patients presenting with coma have large ventricles filled with blood, and many have rebleeding—the overwhelmingly critical factor in outcome of aneurysmal subarachnoid haemorrhage. The development of later cerebral ischaemia from cerebral vasospasm and inability to control it medically are the major factors in poorer outcomes.33 Older age greatly influences outcome, and in patients over age 80 years, the likelihood of meaningful survival is low.33 34 Nonetheless caution is important because poor grade patients may become good grade patients after active interventions.
Coma and CNS infections
The outcome for patients with an infection-induced coma (bacterial or viral) depends on the degree of coma and ‘FOUR Score’ on admission. No patient with a ‘FOUR score’ of less than 3 will survive meningitis.35 Causes for this poor prognosis are cerebral oedema, secondary cerebral infarcts (possibly from associated cerebral venous thrombophlebitis and thrombosis) and hydrocephalus. Time to antibiotic treatment36 is a critical determinant, with delay reducing the likelihood of a good functional outcome. Associated sepsis and septic shock, which can result from late recognition and insufficient aggressive intervention, can also worsen the outcome.37 Likely complications include seizures, acute hydrocephalus and septic cerebral infarctions, all of which affect morbidity. Multiorgan failure and septic shock may be the first presentation in a patient with bacterial meningitis. The most important factor associated with poor outcome in bacterial meningitis is systemic illness that manifests itself by tachycardia, hypotension, positive blood cultures, increased erythrocyte sedimentation rate and thrombocytopaenia.38 39 The underlying cause is important, and the odds of an unfavourable outcome are six times higher in patients infected with Streptococcus pneumoniae when compared with patients infected with Neisseria meningitidis. A CT scan of head showing ventriculomegaly or diffuse brain oedema denotes a poor prognosis.
Outcome of encephalitis remains indeterminate. The variables include age, duration of disease and level of consciousness. Patients younger than 30 years of age who remain largely alert have a much higher chance of returning to preinfection normal life than older patients with altered consciousness. Encephalitis leading to coma is associated with poor outcome, largely because the available treatments are ineffective.40 41 A small proportion will awaken, and an even smaller proportion will regain independent status. Some encephalitides have no effective treatment and hence a poor outcome. These include rabies encephalitis, many of the fungal infections and, more recently, West Nile virus encephalitis. Many patients with fever or meningitis recover fully, but the more invasive neurological form can cause flaccid paralysis and marked changes in basal ganglia, thalami and brainstem. In general, West Nile virus encephalitis has a 20% mortality rate and acute West Nile virus encephalitis myelitis has a 10%–15% mortality rate (and higher in the elderly). A patient who is comatose from West Nile virus encephalitis has a high risk of mortality. Patients requiring mechanical ventilation may seem to have a poor prognosis, but many can show substantial recovery over a number of years.40 41 These recoveries cannot be adequately predicted. Prognostication in most infectious encephalitides likely should be avoided.
Coma and immune-mediated encephalitis
There is increasing evidence that, in a large proportion of patients, encephalitis has an autoimmune origin. Patients often present with worsening encephalopathy and status epilepticus. N-methyl-d-aspartate-receptor encephalitis often results in coma from new-onset refractory epilepsy (NORSE), and there is an emerging consensus that patients with NORSE also require immunotherapy. A recent study warned that dyskinetic and stereotypical movements might have been misdiagnosed and overtreated as status epilepticus.42 First-line immunotherapy includes corticosteroids, intravenous immunoglobulin or plasma exchange, with several more options for second-line immune therapies. The outcome in this patient population is always uncertain, and aggressive escalation of therapy with multiple antiepileptic drugs eventually may lead to months of stay in an intensive care unit and protracted improvement. None of the intuitive poor prognostic indicators (MR brain scan abnormalities, refractory status epilepticus and mechanical ventilation for coma) panned out.43 Some patients may develop severe catatonia.44
Coma and neurotoxicity
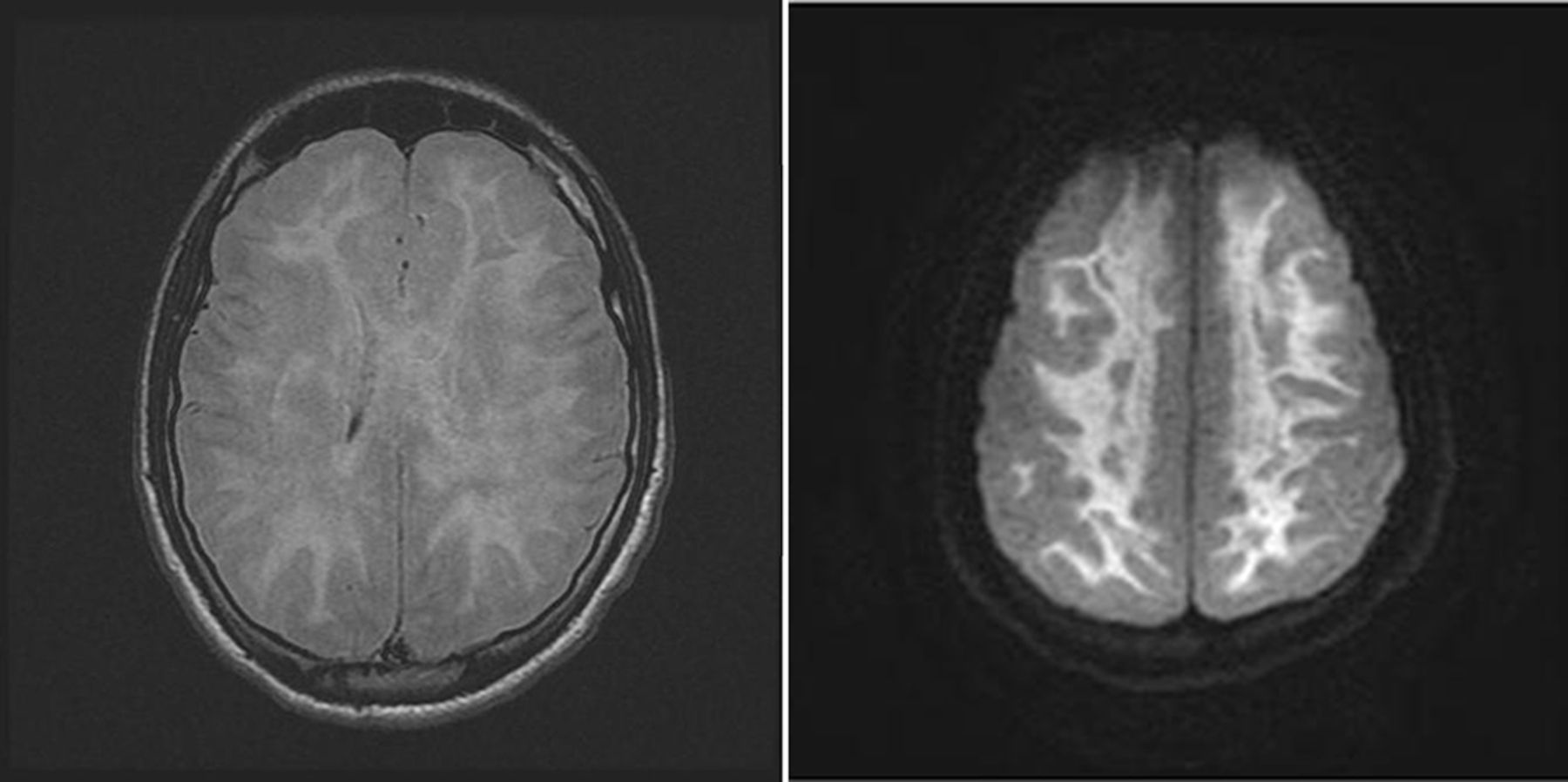
Several types of intoxication and medication overdoses are immediately problematic and may lead to permanent neurological deficits. In many instances, clinical presentation is not easily attributed to a single known toxin. In today’s world, we are confronted with drug abusers, intentional poisoners and, in nearly epidemic proportions, the synthetic opioids. In addition, there is another whole world out there of inhalants containing brain-damaging substances such as aerosols and dry-cleaning fluids. Opioid toxicity—mostly through heroin injection or the use of oxycodone for chronic pain management—can cause permanent injury through anoxic–ischaemic injury. There is a known methadone leucoencephalopathy associated with abnormalities on MR brain imaging that spares the subcortical U-fibres. Usually, this pattern is seen with methadone intoxication.45 Heroin users can remain comatose for weeks with severe white-matter change but sparing of cortex (figure 5). There are a couple extremely important questions that the consulting neurologist should ask. Are there elements of permanent injury, particularly anoxic–ischaemic injury? Do patients need continuous electroencephalography (EEG) monitoring to recognise and manage ongoing seizures? Awakening does occur despite severe white-matter disease on MRI, and even cognition can substantially improve. Nevertheless, prolonged stays in an intensive care unit with tracheostomy and gastrostomy and prolonged gait rehabilitation are common.46 47 Atypical alcohol ingestion (ie, methanol found in commercial products such as windshield washer fluids, deicers, antifreeze, paints, wood stains and glass cleaners) is very problematic and often lethal. Unfortunate cases of survival of intentional carbon monoxide intoxication are occasionally seen. The earliest signs of carbon monoxide poisoning are personality changes with loss of orderliness, snapping at people and outbursts of anxiety but also profound headache and coma when carboxyhaemoglobin concentration increases. Diffuse, haemispheric white-matter involvement on CT scan often develops in comatose patients and patients with long exposure and predicts poor outcome.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Heroin-associated leucoencephalopathy.
Coma and the unknown
There are several circumstances when we do not know (and will never fully know) due to their rarity. These are patients with environmental injuries (eg, electrocution, lightning strikes) and rare disorders such as severe acute metabolic derangements, including hypoglycaemia, leading to permanent coma. In other situations, patients have been found unconscious, and the circumstances cannot be retraced. The best approach remains serial clinical examination and using MR brain imaging to find structural injury and then interpret the severity of injury.
A discussion with the family
Skilful communication about coma and its consequences is just as important as anything else we do in neurology. This needs a complex core team of nurses, clergy and palliative care professionals with experience in mediating differences of opinion. Fortunately, in many cases—after an adequate explanation—common sense prevails, and consensus between families and the healthcare team can be achieved. Again, prognosis is certainly poor in several conditions (box 2).48 49
When the prognosis is certainly poor
Massive haemispheric swelling (any cause).
Deterioration and sequential loss of brainstem reflexes (any cause).
Traumatic brain injury (with primary brainstem and corpus callosum lesions).
Pontine haemorrhage with thalamic extension.
Embolus to basilar artery (with no reopening).
The term ‘futility’ has important connotations, but definitions of medical futility can easily become ‘gobbledy-gook’, and families may wish to continue care even with a very low likelihood of improvement (as long as continuing care does not harm the patient). The quality of the information provided is decisive for many family members. Families may not be fully able to judge the long-term effects of a major neurological injury, and explanations about quality of life should follow. Neurological disability is difficult to describe, and it is even more difficult to know whether the patient can handle these deficits. Just as we would be under similar circumstances, the patient’s family is notoriously unprepared for these situations; the onus is on the experienced neurologist to explain what neurological morbidity and disability entail. Families should clearly understand what we mean by ‘palliative care’, and we should carefully re-explain anything that seems unclear. In general, the aim of palliative care is to reduce suffering and promote comfort resulting in a peaceful and natural death. Conversations should typically occur after 2 weeks have passed or when the patient needs a tracheostomy and gastrostomy. This fork in the road will often lead to reassessment: either support in the hope of improvement or de-escalation to palliative care. We should provide sufficient details about what can be expected for both options. This may be harsh news for the families to absorb: death in a number of days versus prolonged weaning off the ventilator, treatment of multiple complications associated with immobilisation and nursing home placement. The practising neurologist should actively participate in these discussions and develop a rapport with family members.
A final word
The overall lesson is that we rarely should be surprised by the actual outcome if we take all predictive factors into account. If identified, we should ‘Venn diagram’ the comatose patient with a multitude of serious and often obvious medical conditions. Whether all of this will improve our prediction is uncertain. And then there is the unknown. Reawakening is, of course, not the same as recovery, and long convalescence may reveal pervasive major deficits; for many, traits and skills will never return. We will never have an early, reliable prediction for the previously young and healthy comatose patient with a likely structural injury but no convincing abnormality on MR or other poor clinical indicators. We have limited understanding of the outcome in many patients, and we always will. Machine learning will introduce itself in the coming decade, but machines depend on the questions we pose, and even then it may not be enough.50 Prognostication in coma is not a just fallacy of predetermined outcome or in the eye in the beholder and requires a careful evaluation and some observation time to put the deficit into sharp focus. That is why it is important to acknowledge the neurologist who works beyond simple coma scales or scores.
Key points
Prognostication in coma can only proceed with full understanding of its cause.
Prognostication is not improved using major statistical models.
Prognostication works best in identifying the extremes of injury.
Prognostication misjudgements often relate to failure to identify confounders.
References
Footnotes
Contributors EFMW is the sole author of this manuscript. He completed all literature review associated with this article and wrote the first version and the current revision.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests EFMW receives book royalties from Oxford University Press and Elsevier Publishing for authored books on coma, brain death and other issues of critical care neurology.
Patient consent for publication Not required.
Provenance and peer review Commissioned. Externally peer reviewed by Robin Howard, London, UK.
Other content recommended for you
- The Bare Essentials
- Non-convulsive status epilepticus: mimics and chameleons
- Neurointensive care biophysiological monitoring
- Prognosis of status epilepticus: role of aetiology, age, and consciousness impairment at presentation
- Somatosensory evoked potentials aid prediction after hypoxic–ischaemic brain injury
- Intravenous levetiracetam: a new treatment alternative for refractory status epilepticus
- Predictors and prognosis of refractory status epilepticus treated in a neurological intensive care unit
- Efficacy and economic evaluation of delivery of care with tele-continuous EEG in critically ill patients: a multicentre, randomised controlled trial (Tele-cRCT) study protocol
- Continuous EEG use and status epilepticus treatment in Australasia: a practice survey of Australian and New Zealand epileptologists
- Generalised convulsive status epilepticus: an overview