Article Text

Abstract
‘The world is a book and those who do not travel read only one page’.
Augustine of Hippo – Latin philosopher and theologian.
Neurological presentations are seen in about 1.5%–2.0% of returning travellers seeking medical attention, and may pose a particular challenge to diagnose and treat. These may be severe and life threatening, such as meningoencephalitic illnesses or inflammatory radiculoneuropathy (Guillain-Barré-like) syndromes requiring intensive care support. It is essential not to miss the potentially treatable and common diseases such as malaria, which can be lethal if undiagnosed. Herpes simplex virus remains the most common cause of encephalitis in returning travellers to the UK. Furthermore, common bacterial conditions such as pneumococcal meningitis may be associated with different resistance patterns globally, and this must be taken into account in treatment decisio.ns. This review provides a clinical approach, illustrated with a range of cases, and suggestions where to get further management advice.
- tropical neurology
- infectious diseases
- tropical medicine
Statistics from Altmetric.com
Introduction
In the first quarter of 2017, 8.3 million travellers returned to the UK from abroad: a 9% increase from previous years.1 Physicians, especially those at the front line in emergency departments, medical assessment units and attending neurologists, therefore, need to consider infectious disorders, both exotic and non-exotic, in the differential diagnoses of the myriad of neurological presentations.
For those people travelling to low-income and middle-income countries, road traffic accidents are the most common cause of morbidity and mortality. Around half of overseas travellers become unwell, and three-quarters of these develop a gastroenterological, dermatological or a self-limiting feverish illness. About 1.5%–2.0% of returning travellers seeking medical attention have neurological presentations,2 3 which may be challenging to diagnose and treat. These may be severe and life threatening, such as meningoencephalitic illnesses or inflammatory radiculoneuropathy (Guillain-Barré-like) syndromes requiring intensive care support.
Although rare and emerging infections such as Zika virus are novel and exciting to diagnose, it is essential not to miss the potentially treatable and common diseases such as malaria, which can be lethal if undiagnosed. Herpes simplex virus remains the most common cause of encephalitis in returning travellers to the UK and HIV causes a range of neurological manefestations, see Box 2. Furthermore, common bacterial conditions such as pneumococcal meningitis may show different resistance patterns globally, which must be taken into account in treatment decisions.
Clinical approach
As is usually the case in medicine and neurology in particular, the history—specifically the travel history—remains the key to the diagnosis of travel-related neurological disorders. This includes documentation of stopovers and multiple journeys (table 1 and case 3). It is also crucial to document any salient medical history, for example, infection with HIV or immunosuppressant drugs, since these drastically change the clinical presentation, differential diagnoses and management.
Travel history in a returning traveller with neurological disorder
Neurological presentations are classically managed using a syndromic approach, that is, localisation, and this extends to the evaluation of returning travellers with neurological illnesses (table 2). The UK guidelines for meningitis and encephalitis provide an excellent framework for diagnosis and treatment, with individual sections on the evaluation of returned travellers.4 5 There are some data to suggest that the syndromes are not always entirely clear-cut, with bacteria and viruses presenting with meningoencephalitis rather than simply meningitis or encephalitis.6–8
Neurological syndromes
Identifying the potential organism(s) causing the presenting disorder requires knowledge of the epidemiology of infections that the patient will have been exposed to in any part of the world (figure 1). In addition, incubation periods of different conditions present an important variable to consider when trying to make a diagnosis (table 3).

Distribution of the important travel-associated neurological infections of the central nervous system (reproduced with permission from Thakur and Kunt14).
Typical incubation periods of travel-related infections
Case 1
A male university student aged 23 years was admitted to hospital with a 1-week history of a febrile illness. He had spent Christmas in Kenya and Uganda, and had swum in the River Nile. His general practitioner had diagnosed influenza and advised him to rest at home and take paracetamol. In the emergency department, he also reported chills, myalgia, diarrhoea and vomiting. He had mild confusion, with impaired memory for recent events, but his Glasgow coma scale score was 14/15 with no focal neurology. Initially, he was afebrile with a moderate tachycardia, 100 beats per minute. However 8 hours later, on the ward, he became more acutely unwell, with a temperature of 40°C, respiratory rate 33 per min, blood pressure 75/70 mm Hg, pulse 120 beats per min, arterial pH 7.23 (7.35–7.45) and serum bicarbonate 19.3 mmol/L (20–28).
Blood tests showed haemoglobin of 130 g/L (130–180), white cell count 10.3×109/L (4.0–11.0) and platelets 24×109/L (150–400). A thick film confirmed malarial parasites, with 12% parasitaemia, and a positive malarial antigen test. He was started on intravenous artesunate. The next day his parasite count was still 12%, and his haemoglobin dropped to 81 g/L (130–180), and platelets 78×109/L (150–400). Repeat bloods on the third day of hospital admission showed a fall in the parasite count to 5.2%.
Diagnosis: Plasmodium falciparum malaria—illustrating the rapid clinical deterioration that makes malaria a medical emergency.
Case 2
A male hospital technician aged 61 years was brought into hospital 8 days after returning from Uganda with a Glasgow coma scale score of 5. He had no meningism, but bilateral extensor plantar responses, and was oliguric, jaundiced and tachycardic. He was thrombocytopenic with skin lesions visible as shown in figure 2.9 He eventually recovered completely but required digital amputations.

Peripheral gangrene of the toes of the left foot (reproduced with permission from Helbrok et al9).
Malaria
Malaria is the most common tropical infection imported into the UK, with 1300–1800 cases and 2–11 deaths every year.10 Two-thirds of cases occur in people of African or South-Asian origin, typically after visiting friends and family in endemic regions. Three-quarters of malaria cases are due to P. falciparum, which may rapidly evolve into a severe multiorgan life-threatening disease (as illustrated by the two examples). Most other cases are due to Plasmodium vivax. Late presentations may be with confusion, coma and or seizures. Suspected cases of malaria must be treated as a medical emergency.
Unfortunately, the diagnosis may be delayed because patients and clinicians may each fail to acknowledge the travel history or to consider malaria in differential diagnosis. Other potential pitfalls include the belief that prophylaxis prevents all malaria and that fever is always present. Malaria in children, and sometimes adults, may present with non-specific symptoms implicating the gastrointestinal and respiratory systems.
The most sensitive test for malaria is the microscopic examination of thick and thin blood films by an experienced laboratory technician. However, this expertise is often lacking, especially out of hours. The rapid diagnostic tests that detect parasite antigens are now commonly used. They are less sensitive than blood film examination by an experienced operator but serve as a useful screening test; the tests should be used in conjunction. If the initial blood films are negative, repeat films with or without rapid diagnostic tests should be examined after 12–24 hours and again after a further 24 hours. Three negative blood films examined by an experienced operator make the diagnosis unlikely.11
Uncomplicated P. falciparum malaria should be treated with an artemisinin combination: artemether with lumefantrine, or dihydroartemisinin with piperaquine. If these are not available then quinine combined with oral doxycycline or atovaquone-proguanil (Malarone) can be used.
Patients with severe malaria (>2% red cell parasitaemia) or who have complications need managing in the high-dependency unit or intensive care unit setting, with intravenous artesunate. If artesunate is not available immediately, use intravenous quinine, although this requires careful monitoring for hypoglycaemia.11
Postmalarial neurological syndromes are a well-recognised complication, presenting as cerebellar ataxia, Guillain-Barré syndrome or the specific postmalarial neurological encephalopathic syndrome. The presentation is as a monophasic disorder with confusion, psychosis, seizures, hallucinations and ophthalmoplegia. The MR scan of brain may be normal or have features resembling acute disseminated encephalomyelitis with widespread areas of demyelination. The onset is between 2 and 60 days with a duration of 2–3 (range 1–10) days. The risk factors for this complication are the severity of the falciparum malaria and the antimalarial drug mefloquine.11
Case 3
A man aged 28 years presented with a 4-week history of mild back pain, difficulty with micturition and radicular pains in both legs. He had been working in the Congo as a non-governmental officer travelling to small villages on a bicycle, sleeping in local accommodation and eating local food. On examination, he was afebrile. Neurological examination was normal apart from an absent left ankle jerk.
Routine blood tests were normal. The cerebrospinal fluid examination showed a white cell count of 320/µL (≤5) (lymphocytes), protein 1.25 g/L (0.15–0.45), glucose 2.4 mmol/L (plasma glucose 5.0 mmol/L), cytology reactive lymphocytes only.
MR scan of brain showed high signal in the lower thoracic cord, with gadolinium enhancement.
The differential diagnoses considered were infection (eg, schistosomiasis), inflammatory (eg, sarcoidosis), neoplastic (eg, lymphoma) disorders.
On the basis of his travel history and the neurological presentation, he was diagnosed with myeloradiculopathy due to schistosomiasis. He received praziquantel and prednisolone before the serological results were available. Four weeks later, there was no improvement and all serological tests for schistosomiasis were negative. A further travel history revealed at that after returning from the Congo, he had been on a walking holiday in Scotland. Although he could not recall a tick bite, subsequent serology for Lyme disease was strongly positive. Following treatment with 1 month of ceftriaxone, he completely recovered.
Diagnosis: Lyme myeloradiculopathy due to Borrelia burgdorferi (Bannwarth’s syndrome).
This case illustrates the importance of taking a full and detailed travel history.
Case 4
A woman aged 44 years gave a 1-week history of progressive symptoms of paraparesis, altered sensation and micturition difficulties.12 Enquiries into her travel history revealed a 4-year period spent in Zimbabwe, 5 years before. She had swum in Lake Malawi. On examination, there was a flaccid paraparesis with a T11 sensory level. MR imaging (figure 3) showed conus medullaris expansion with high T2 signal extending rostrally up to the T10 level. There was also irregular gadolinium enhancement of the conus and cauda equina.

A. Sagittal T2-weighted sequences of the spine showing swelling and hyperintense signal change of the caudal spinal cord and conus medullaris. B. Postcontrast sagittal T1-weighted sequences of the spine showing patchy avid enhancement of the caudal spinal cord and conus medullaris. There is also some caudal nerve root thickening and enhancement.
The impression was that the patient had a neoplastic lesion, and she was started on corticosteroid treatment, with improvement in symptoms. However, surgical resection and subsequent histology identified schistosoma eggs within necrotising granulomas. Examination of urine and stool found no schistosoma eggs. Specific schistosoma ELISA antibody test was positive.
She was treated with praziquantel and gradually made a full motor recovery, although with a mild sensory deficit.
Diagnosis: Schistosomiasis myelopathy. This case illustrates that patients with schistosomiasis can present years after exposure, emphasising the importance of a detailed travel history.
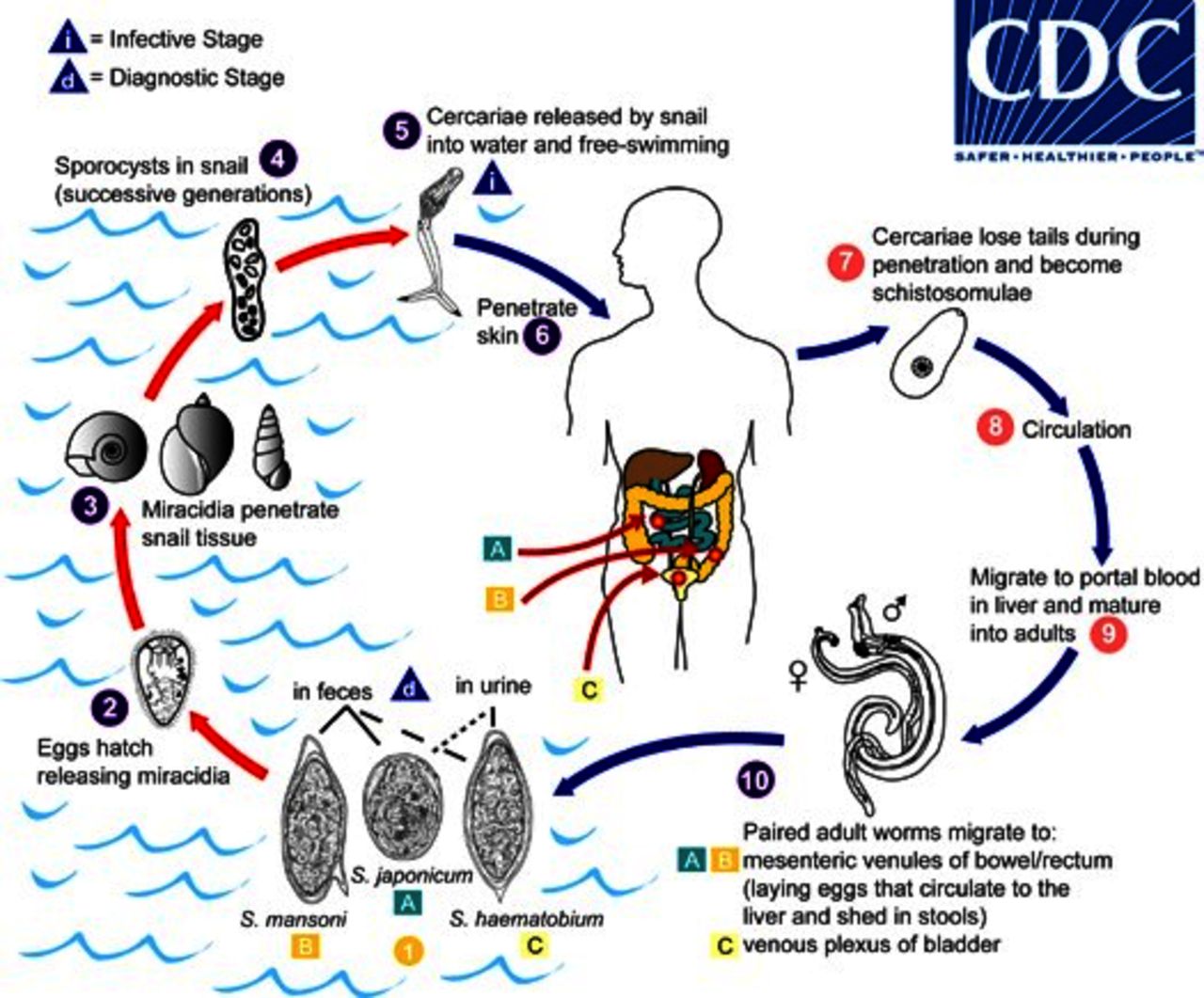
Life cycle of schistosomiasis (reproduced with permission from the Centers for Disease Control and Prevention).
Schistosomiasis
The lifecycle of schistosomiasis is illustrated in figure 4. Infection with the helminthic blood fluke schistoma is second only to malaria in terms of socioeconomic and public health importance in tropical and subtropical areas. Worldwide, almost 200 million people are infected. Schistosoma japonicum is mainly found in China, the Philippines and South-East Asia; Schistosoma mansoni is found in Africa, South-East Asia, the Caribbean, the Middle East and parts of South America; Schistosoma haematobium occurs mainly in Africa.
Humans, the definitive hosts, excrete the parasite eggs through faeces and urine into fresh water. The released miracidia then penetrate the intermediate host—the fresh water snail—where asexual multiplication occurs. The released cercariae penetrate human skin exposed to fresh water. The mature schistosomulae worms form mating pairs that inhabit the venous plexi around the bladder (S. haematobium), rectum (S. mansoni) and portal vein and liver (S. japonicum).
Neuroschistosomiasis occurs when eggs pass into the central nervous system by retrograde venous flow from the iliac veins and inferior vena cava through the valveless Batson venous plexus. The mature larvae elicit a variable inflammatory reaction depending on the host immune status. In naïve patients, such as travellers to endemic areas, the response is often more intense with a severe granulomatous reaction or occasionally a vasculitis.13
Cerebral involvement is rare and usually occurs with S. japonicum because the eggs are smaller. The clinical presentation may be with acute encephalopathy (delirium, headache, seizures, focal neurological deficits or coma) usually in people with prior exposure. Alternatively, patients can present with granulomatous mass lesions that mimic brain tumours or abscesses.14
A myeloradiculopathy is usually caused by S. mansoni or S. haematobium. The presentation may be acute or subacute with a lower spinal cord and cauda equina syndrome. Occasionally, as in the case above, the onset may be delayed. The underlying pathological mechanism of damage can be either myelitic (with a rapidly progressive necrotic myelopathy and a relatively poor prognosis) or a granulomatous form that, if treated early, has a better outcome.
Blood tests are usually normal, although an eosinophilia may be an indicator. The CSF may show a lymphocytosis with or without eosinophils with an elevated protein concentration.
Serological tests in blood with ELISA are positive in >90% of patients but cannot distinguish between exposure and acute infection. A positive CSF ELISA may help more in confirming the diagnosis.13 Antischistosomal antibodies occur in 80%–90% of neuroschistosomiasis cases.
Schistoma eggs may be detected in faeces (S. mansoni and S. japonicum) or urine (S. haematobium). Repeat sampling and centrifugation of urine and examination of the sediment increases the diagnostic rate.
The treatment is usually with praziquantel 60 mg/kg/day for 3 days with prednisolone cover.13
Case 5
A Caucasian man aged 32 years presented with a generalised tonic-clonic seizure. Neurological examination was normal. He had an extensive travel history: Borneo, India (Mumbai, Goa, Kerala) and Morocco.
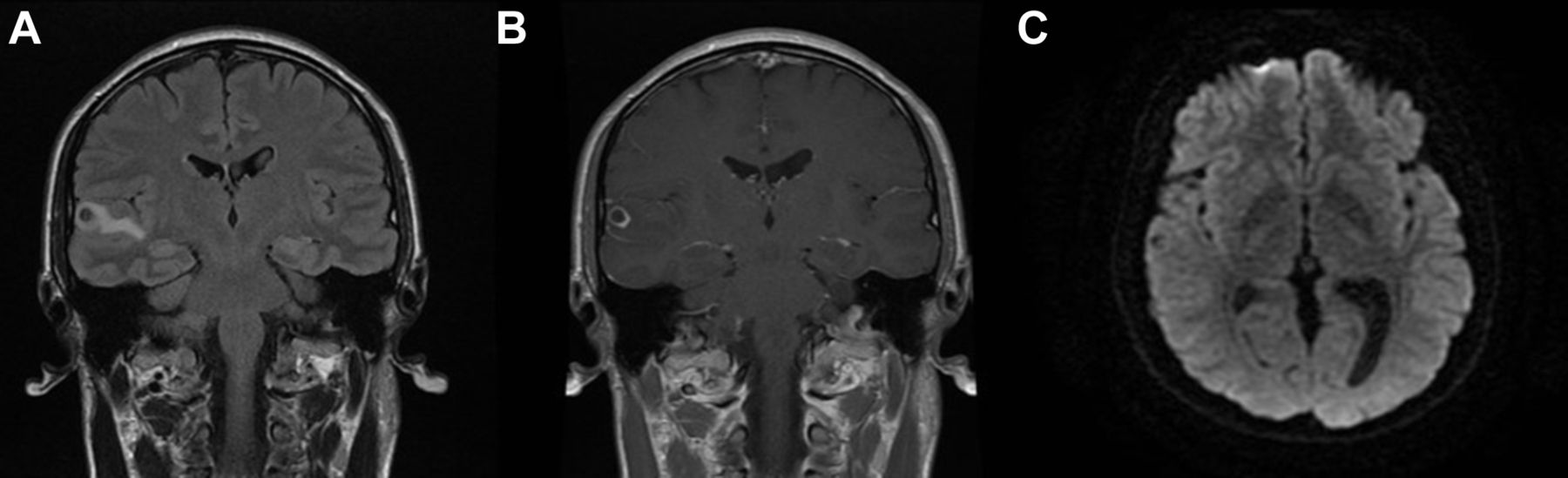
MR scans (figure 5) showed a single lesion in the right superior temporal gyrus with a) perilesional oedema, b) enhancement and c) a visible scolex.

(A) Coronal fluid-attenuated inversion recovery MR scan of brain showing a small hypointense focus within the right superior temporal gyrus, suggesting a granuloma, with associated perilesional oedema. (B) Postcontrast T1-weighted coronal MR scan of brain showing peripheral enhancement of the lesion situated within the right superior temporal gyrus. (C) Axial diffusion-weighted imaging MR scan of brain showing a temporal lesion with the scolex visible.
Specific blood serological investigations found that the cystercercal immunoblot and cysticeral antigen were negative. The CSF showed two lymphocytes/µL (≤5), protein 0.43 g/L (0.15–0.45). The CSF immunoblot test was negative but the cystericercal antigen test was positive.
He was given antiepileptic medication lamotrigine 100 mg twice daily. Subsequently, he was admitted to hospital and treated with oral praziquantel and albendazole under dexamethasone cover. Six months later, he remained seizure free with complete resolution of the temporal lesion.
Diagnosis: Neurocysticercosis.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
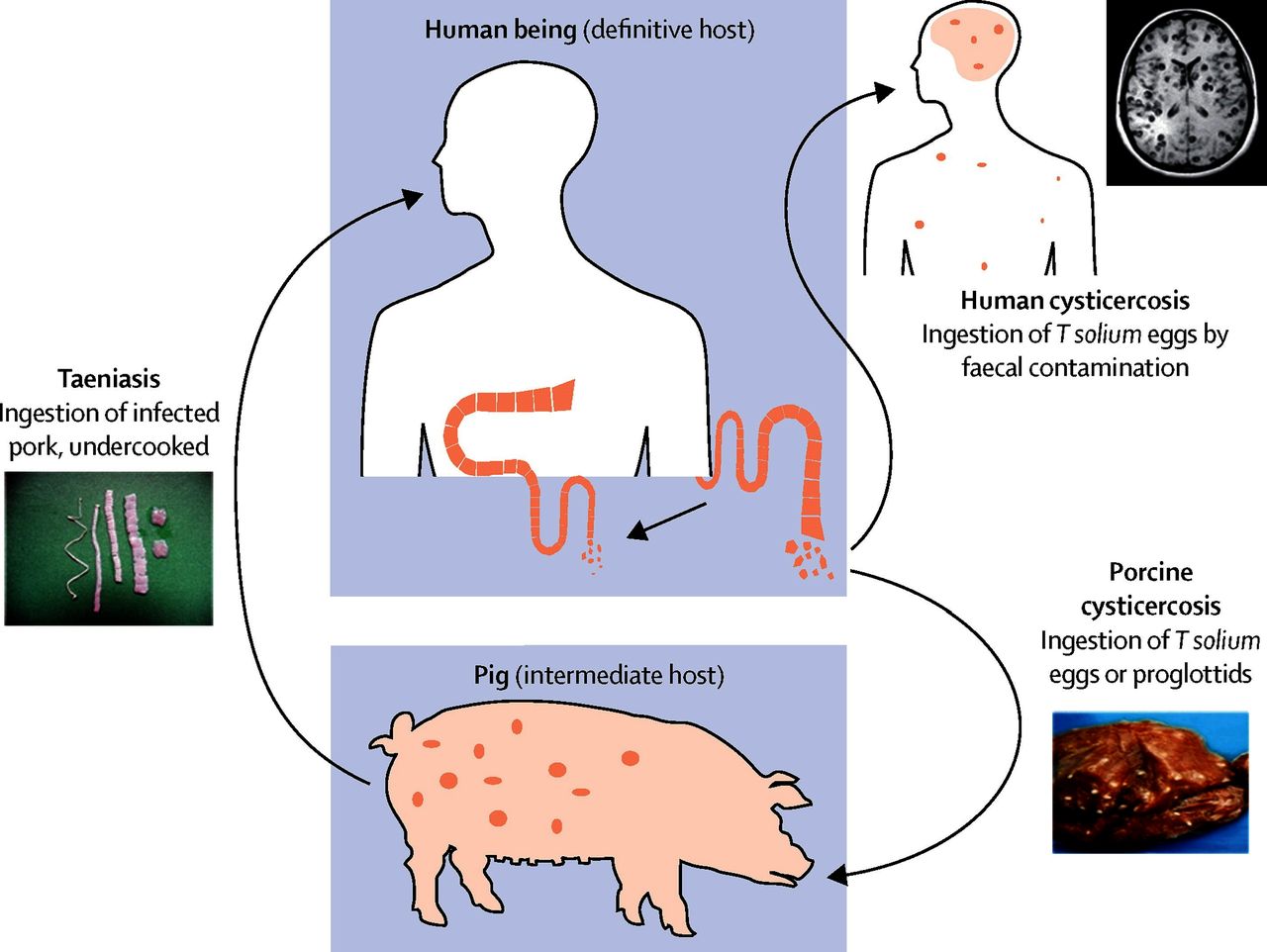
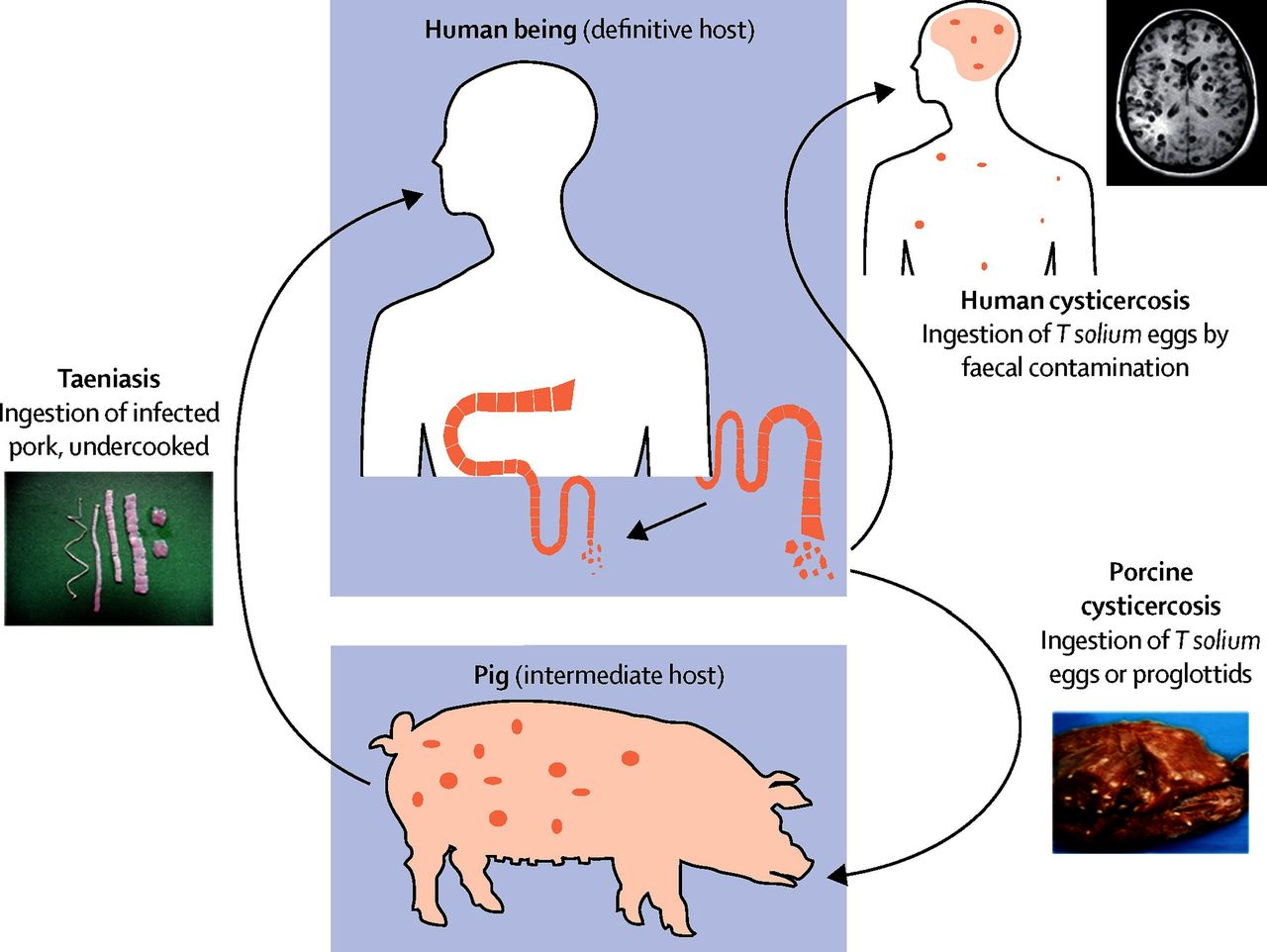
Life cycle of neurocysticercosis (reproduced with permission from Garcia et al18).
Neurocysticercosis is one the most common parasitic diseases of the central nervous system, and the most common cause of seizures in certain parts of the world. It is endemic in most low-income countries where pigs are raised.15 In non-endemic areas, the diagnosis in increasingly made in immigrants from and travellers to endemic areas, which include Central and South America, India, South-East Asia and parts of sub-Saharan Africa.
It is important to note that it is not necessary to eat pork to develop neurocysticercosis, since the disease follows the ingestion of eggs of the pork tapeworm (Taenia solium); these are excreted in the stools of a carrier (taeniasis) and then spread by faecal-oral contamination due to poor hygiene, see figure 6. The eggs hatch and the larvae disseminate usually to the brain, muscles, spinal cord or the eyes. Cysts (single or multiple) may remain viable (in the vesicular stage) for many years, but eventually degenerate, provoking an inflammatory response and granuloma formation.16 Seizures, the most common manifestation of neurocysticercosis, usually present when the viable cysts degenerate but may also occur in the presence of already calcified cysts, which may from time to time develop perilesional inflammation. Other presentations include hydrocephalus due to intraventricular cysts or subarachnoid (racemose) lesions. Rarely, patients with a heavy lesion load develop massive inflammation (cysticercosis encephalitis).
The diagnosis is made in patients with the appropriate travel history and supported by imaging studies and serology. CT scan of head shows single or multiple cysts with variable degrees of calcification. MR imaging shows vesicular cysts as small lesions (with no enhancement or oedema) and the tapeworm scolex appears as an internal asymmetric nodule. Fluid-attenuated inversion recovery, fast-imaging employing steady state acquisition sequence, constructive interference in steady state or balanced-fast field echo sequences are more sensitive to intraventricular and cisternal cysts. Susceptibility-weighted imaging is best for detecting calcified lesions.16
The enzyme-linked immmuno-electrotransfer blot assay, which detects antibodies to T. solium in serum, has a sensitivity of 98% in patients with two or more live parasites in the nervous system, but a low sensitivity (50%–60%) is people with a single lesion. Serial quantification of circulating cystericercal antigen by ELISA with monoclonal antibodies is used to monitor treatment response. The antigen test may sometimes help to confirm the diagnosis in blood or CSF, as in case 5, thus avoiding an excision biopsy procedure.
Treatment. After years of controversy regarding treatment with antiparasitic drugs, the current consensus is to treat those people who have single or multiple cysts that are in the vesicular or colloidal degenerating stages, in order to decrease the number of active brain lesions on imaging and to reduce long-term seizure frequency. This is best done as an inpatient and under dexamethasone cover.15 17 More recently, a study by Garcia et al, showed that combination therapy with albendazole (15 mg/kg/day) and praziquantel (50 mg/kg/day) for 10 days with dexamethasone 0.1 mg/kg/day was safe and more effective than albendazole alone.16 18 Calcified cysts do not require treatment.15
Where to ask for help
There are structures in place, and being developed, to provide us with real-time information on emerging diseases and outbreaks. Aside from local infection specialists, or the UK Imported Fever Service, there are invaluable online resources such as Public Health England, the National Travel Health Network and Centre, Centers for Disease Control and Prevention (CDC) and the Programme for Monitoring Emerging Infectious Diseases, see full details in box 1.
Useful resources for UK neurologists
Imported Fever Service
24 hours, 7 days a week UK service—to provide expert clinical and microbiological advice and sample testing to support management of febrile patients, infection control and public health interventions (https://www.gov.uk/guidance/imported-fever-service-ifs); +44 844 778 8990.
National Travel Health Network and Centre
UK resource to provide the best quality, evidence-based travel health advice and services (https://travelhealthpro.org.uk/); +44 845 602 6712.
Programme for Monitoring Emerging Infectious Diseases
Internet-based reporting system dedicated to rapid global dissemination of information on outbreaks of infectious diseases and acute exposures to toxins that affect human health. Official programme of the International Society of Infectious Diseases (https://www.promedmail.org/).
UCLH/HTD/PHE Department of Parasitology offers 24 hours advice.
Notifiable diseases
Many infections fall into the category of notifiable diseases, those that should be notified to Public Health England. The infection specialist may do this, but it is important to check.
Key points
Take a detailed travel and vaccination history, including precise dates of travel and onset of symptoms, food eaten, exposure to animals, caves and water.
Consider a diagnosis of malaria in anyone with a fever, or a history of fever, who is returning from an endemic region, regardless of prophylaxis.
Neurocysticercosis occurs in non-pork eaters.
Consider HIV and seroconverting illnesses(table 2).
Communicate with your infection teams early (microbiology, virology, infectious diseases) and discuss cases with them to ensure the correct samples are taken.
Ask for expert help, including the Imported Fever Service and the UK Parasitology laboratory.
Acknowledgments
We thank Professor Peter Chiodini for helpful advice on serology testing in schistosomiasis and neurocysticercosis, Dr Stephen Wright for advice on case 3, Dr Richard Greenwood for case 4 and Dr Indran Davagnanam for MR imaging interpretation.
References
Footnotes
Contributors TB and HM contributed equally to the drafting and revisions of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Commissioned; externally peer reviewed by Nick Davies, London, UK.
Data sharing statement There is no other data available.
Linked Articles
- Editors’ commentary
Other content recommended for you
- Diagnosis and management of schistosomiasis
- Rare cause of right iliac fossa pain in a UK patient
- How to interpret malaria tests
- A rare cause of asymptomatic solitary pulmonary nodule: adult Schistosoma worm
- Fever in the returning traveller: the importance of sensitivity
- Fever in the returning traveller
- Identification and management of co-infections in people with malaria
- Surgical case of subacute headache in a young Latin American woman
- Schistosoma haematobium causing pulmonary schistosomiasis in a returning traveller
- Evaluation of Artesunate-mefloquine as a Novel Alternative Treatment for Schistosomiasis in African Children (SchistoSAM): protocol of a proof-of-concept, open-label, two-arm, individually-randomised controlled trial