Article Text

Abstract
A fundamental characteristic of peripheral vestibular nystagmus, in particular horizontal nystagmus, is that it is suppressed by visual fixation. This means that a patient with a vertigo attack of peripheral vestibular origin might have no obvious spontaneous nystagmus on clinical examination. Goggles that reduce or remove visual fixation allow the cliniican to observe nystagmus in this situation. Nystagmus goggles are essential for any clinician dealing with dizzy patients. Here, we discuss why this is so and how easy it is to acquire and use them.
- Vision
- Neurootology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHY NYSTAGMUS GOGGLES?
The reason for examining a dizzy patient is to find clinical signs that help distinguish a peripheral from a central vestibular cause for the dizziness. Seeking and characterising nystagmus is basic to this examination. But there is a catch. Peripheral vestibular nystagmus, mainly its horizontal component, is normally suppressed by visual fixation (partly if the nystagmus is intense, fully if it is not). The converse of this rule also holds: any horizontal nystagmus that is not suppressed by visual fixation is not of peripheral vestibular origin.
Supplementary file 1
Thus, not only is absence of evidence not evidence of absence, but the opposite might be so: absence of spontaneous nystagmus on naked eye examination of a dizzy patient might indicate that the patient has visually suppressed peripheral vestibular nystagmus, a potentially informative negative finding if there were some way to reveal the peripheral nystagmus.
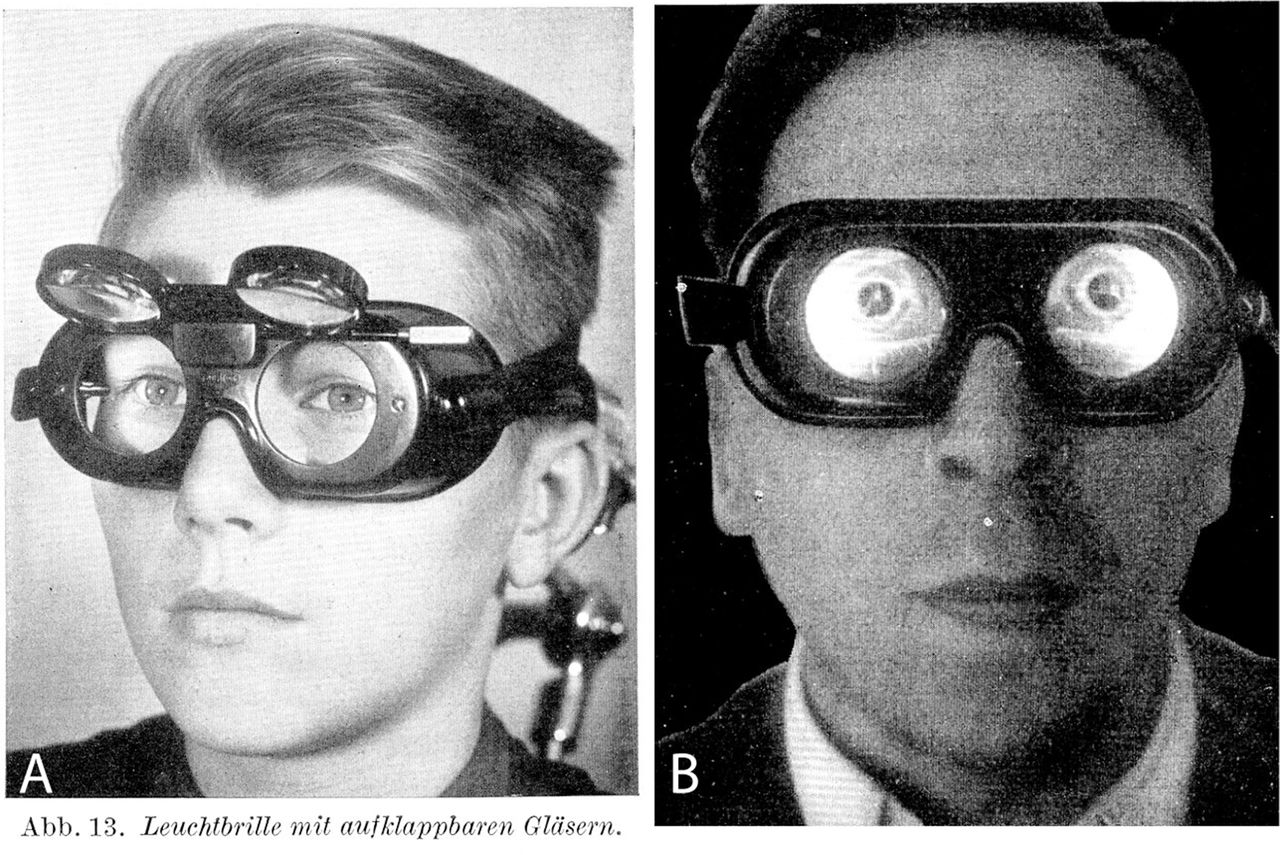
The answer to this conundrum—the removal of visual fixation while still being able to observe the eye movements—was worked out nearly a hundred years ago by Professor Dr Hermann Frenzel (1895–1967) an eminent otolaryngologist from Göttingen.1 His nystagmus goggles incorporated high-dioptre lenses that made it difficult for the patient to focus on him but easy for him to focus on the patient’s eyes, especially when the goggles were illuminated from within (figure 1A, 1B). Modern versions of his nystagmus goggles are still available and still popular. They are rugged and portable and as useful in the Emergency Room as in the clinic (figure 2A, 2B). For greater precision and a permanent measurable record, most neuro-otology clinics use one of the many infrared video nystagmus goggles now available (figure 4) illustrated in the linked videos. While these give high-quality permanent recordings and make repositioning manoeuvres for benign positional vertigo easier to control, they are expensive and not yet easily portable.
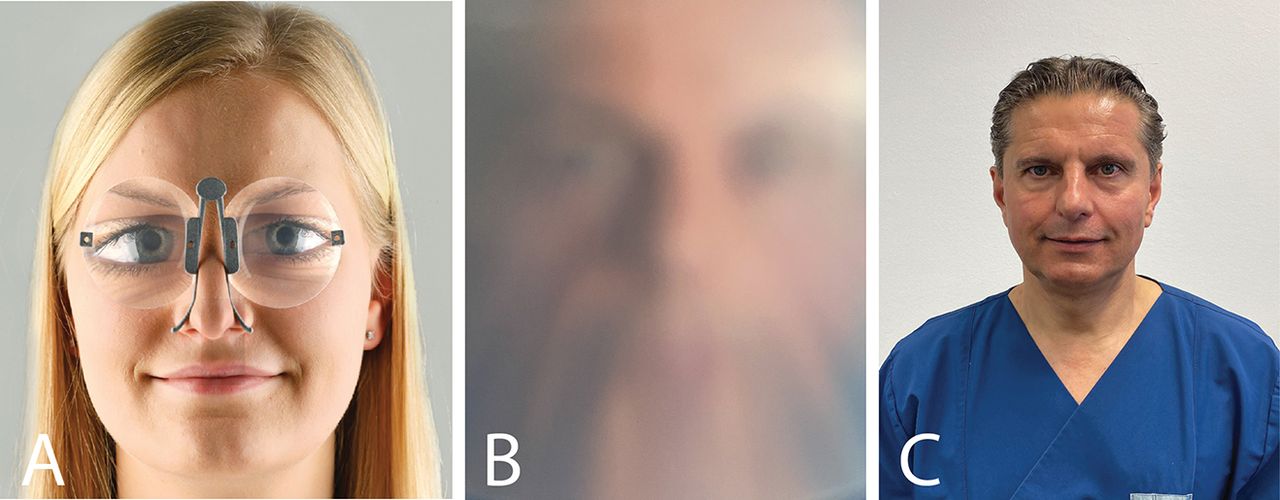
For ease of use and carriage (jacket pocket) and for economy, pince-nez type nystagmus glasses based on Fresnel prisms are useful and have become popular worldwide (figure 3A, 3B).2 There are also many slightly different cheap and cheerful DIY nystagmus goggles/glasses, each with its loyal inventor/enthusiast.3 4
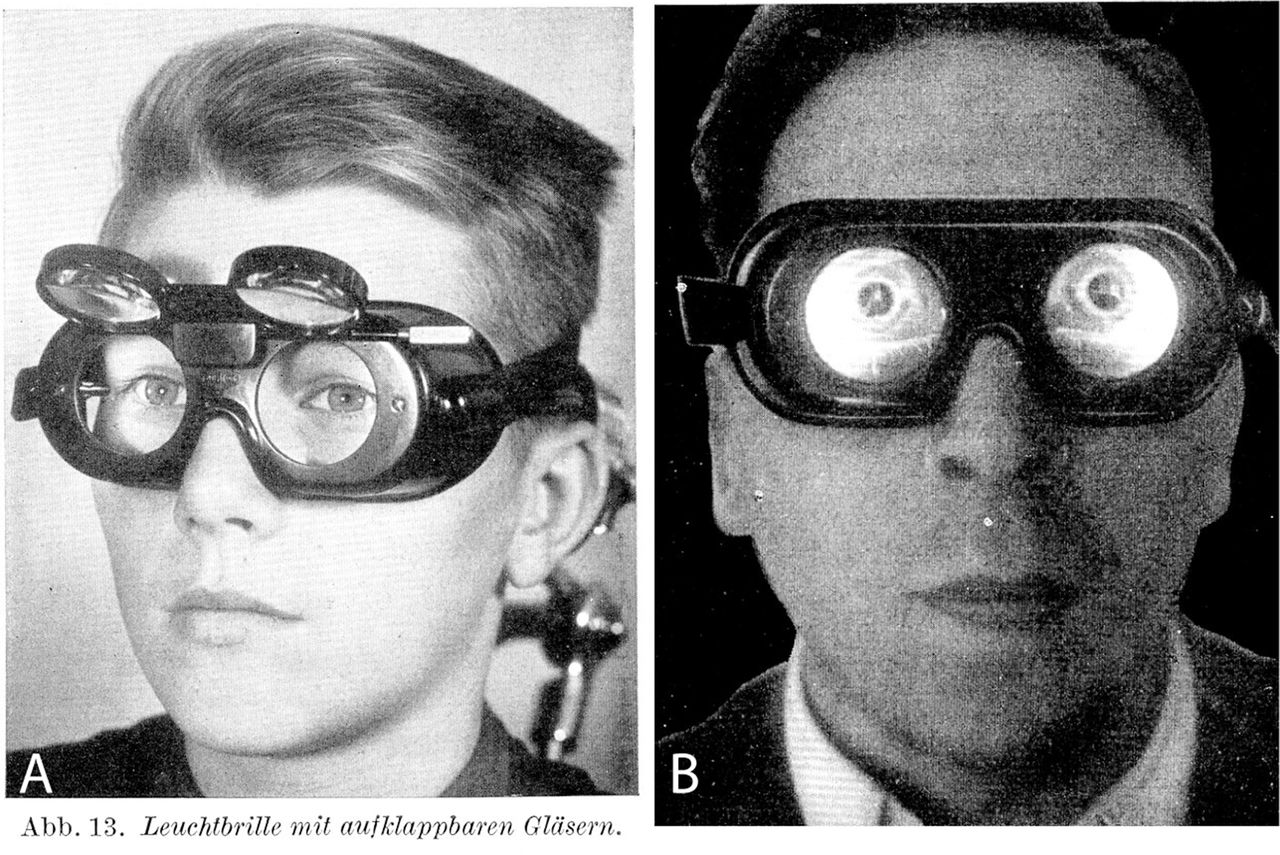
Dr Frenzel’s nystagmus goggles. Open (A), closed (B) and illuminated from within. (from Frenzel5).

Contemporary version of Dr Frenzel’s nystagmus goggles. Examiner’s view of the patient (A) and patient’s view of the examiner (B).
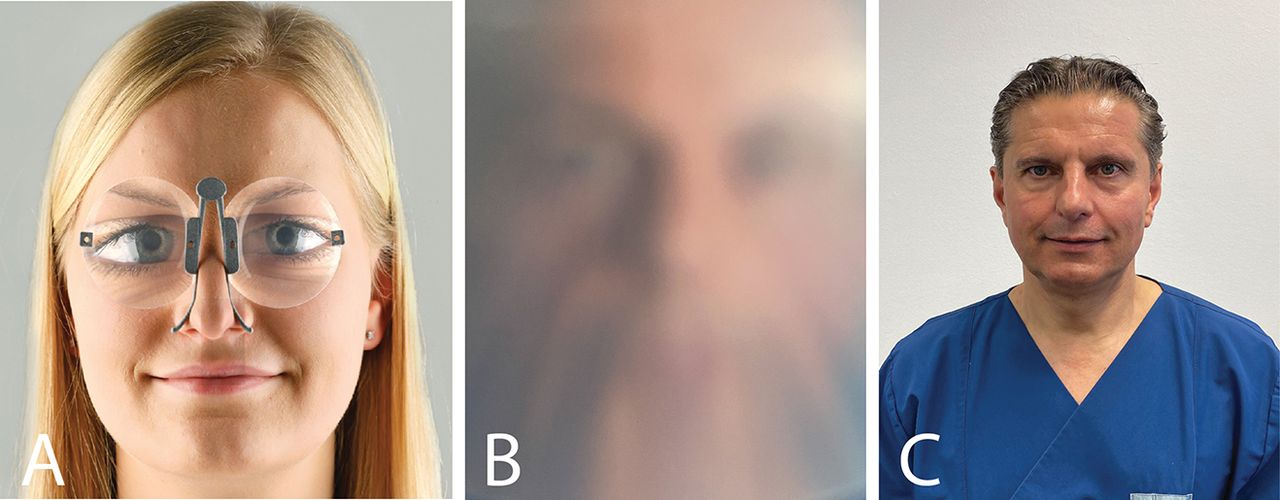
Dr Strupp’s ‘M’ nystagmus glasses. Examiner’s view of the patient (A), patient’s view of the examiner (B) and the examiner (C).
MECHANISM OF PERIPHERAL VESTIBULAR NYSTAGMUS
In order to understand and to interpret correctly, observations made with nystagmus goggles, it is useful to know something about the mechanisms and characteristics of peripheral vestibular nystagmus.
Vestibular neurons are active at rest. This means, for example, that the peripheral vestibular nerve neurons that transmit impulses from receptor hair cells in the two lateral semicircular canals to central vestibular nucleus neurons in the brainstem, and these vestibular nucleus neurons themselves, actively signal the fact that the head is not rotating. The resting rate of these single neurons in a monkey is around 40 action potentials per second.
Semicircular canals work as pairs. Resting activity makes vestibular neurons bidirectionally responsive. For instance, an angular acceleration to the right increases the activity of right vestibular neurons and decreases the activity of left vestibular neurons.
The vestibulo-ocular reflex, including the slow phase of peripheral vestibular nystagmus, rotates the eyes at the same speed as the head—in the opposite direction. The fast phases of vestibular nystagmus (the beats) originate in the pontine reticular formation, adjacent to the vestibular nucleus. This means that, for example, both the leftward slow phases and the rightward fast phases of the right-beating nystagmus produced by a rightward head acceleration are generated by the right lower brainstem.
If the peripheral vestibular system on one side, say the left, is acutely damaged (or cooled, as in a caloric test), there will be asymmetrical resting activity in the two vestibular nuclei: reduced on the left, normal but now relatively higher on the right; the result is right-beating peripheral vestibular nystagmus. This is the same as what would happen during a rightward rotation.
CLINICAL FEATURES OF PERIPHERAL VESTIBULAR NYSTAGMUS
It always beats in the direction of the relatively more active of a semicircular canal pair: that is, fast phase towards and slow phase away from the relatively more active labyrinth.
It is always transient if stimulus-induced, say by rotation, head-shaking or canalithiasis, and temporary if disease-induced as in acute vestibular neuritis or an attack of Menière’s disease.
It is always due to unilateral, or if bilateral then asymmetrical, vestibular disease or stimulation. Warm caloric stimulation of the right labyrinth produces right-beating nystagmus (online supplemental video 1). Right-beating rotational vestibular nystagmus is due to excitation of primary afferent neurons from the right labyrinth and disfacilitation of primary afferent neurons from the left labyrinth (online supplemental video 2). A right Dix-Hallpike test or diagnostic Semont manoeuvre in a patient with right posterior canalolithiasis and benign positional vertigo produces upbeating and rightward torsional nystagmus from stimulation of the right posterior semicircular canal. An acute right vestibular neuritis produces left beating-horizontal-torsional nystagmus from unopposed tonic activity of the left lateral and posterior semicircular canal primary afferent neurons.
It is always suppressed by visual fixation. Failure of fixation suppression indicates cerebellar disease (see below and online supplemental video 3, online supplemental video legends).
Supplementary file 2
Supplementary file 3
Supplementary file 4
VISUAL SUPPRESSION OF PERIPHERAL VESTIBULAR NYSTAGMUS
In the series of linked videos, we provide examples of normal visual suppression of normal peripheral vestibular nystagmus induced in normal subjects. Our aim is to emphasise that if visual fixation is not removed, it is difficult or even impossible to recognise that the patient has peripheral vestibular nystagmus (box 1). While visual fixation also needs to be removed for caloric or rotational laboratory tests of vestibular function (figure 5), is not our aim to describe these tests here.
For practising neurologists, the takeaway message from all this is that when examining an acutely dizzy patient, the absence of nystagmus by naked eye examination of the eyes does not mean that the patient has no nystagmus; it might mean that the patient has a peripheral vestibular nystagmus that is being normally suppressed by vision.6

Infrared video nystagmus goggles. Camera with fixation LED occupies the left socket and cover occupies the right. (A) Examiner’s view with fixation LED on. (B) Subject’s view with fixation on. (C) Subject’s view with fixation off—the subject would now be in total darkness. With camera out, cover in: (D) examiner’s view; (E) subject’s view; the subject can see the room. With camera in, fixation on, cover out: (F) examiner’s view; (G) subject’s view—the subject can also see the room.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
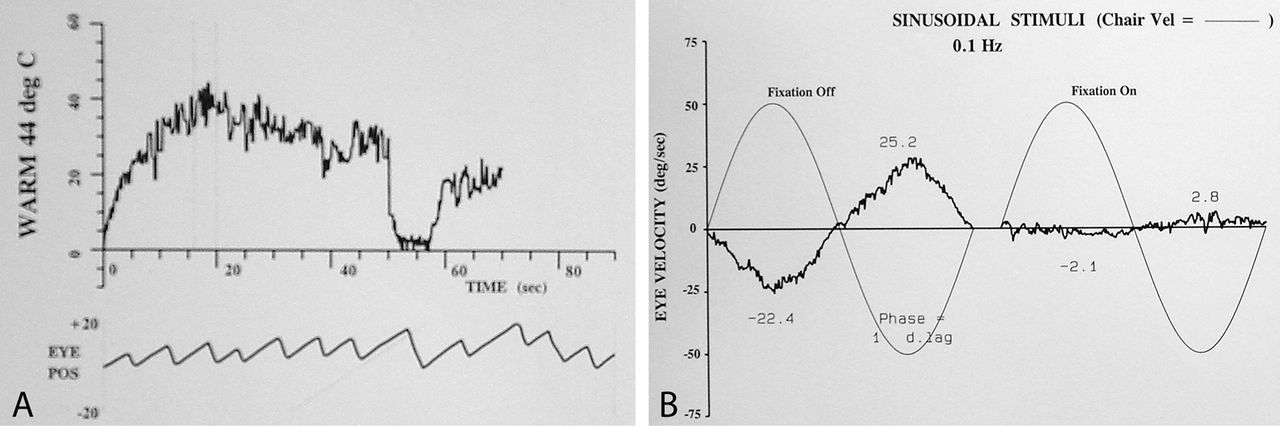
Visual suppression of peripheral vestibular nystagmus in normal subject. (Left) beating nystagmus in response to 44°C caloric irrigation of the left ear. After removal of the nystagmus quick phases, the nystagmus slow-phase velocity envelope is shown for 70 s starting at 20 s after the start of irrigation. The nystagmus slow-phase velocity builds up over 20 s to a peak velocity of 40 deg/s. The segment of nystagmus at peak slow-phase velocity, from 15 s to 20 s after the start of recording (interval indicated by two dotted vertical lines), is shown at the lower part of the figure. At 50 s, the fixation LED is turned on for 10 s and this suppresses the nystagmus, almost totally. Time on the horizontal axis, nystagmus slow-phase velocity on the vertical axis (online supplementary video 1). (Right) Nystagmus slow phase velocity in response to sinusoidal oscillation at 0.1 Hz right–left at peak velocity of 50 deg/s in a normal subject (GMH). On the left of the figure is the extracted slow-phase velocity of the nystagmus with fixation off, and on the right with fixation on. The peak slow-phase velocity on rightward rotation without fixation is 22.4 deg/s; with fixation it is 2.1 deg/s; on leftward rotation, these values are 25.2 deg/s and 2.8 deg/s. This shows that at a stimulus frequency of 0.1 Hz and magnitude of 50 deg/s, vision suppressed vestibular nystagmus by around 90% (See online supplementary video 2, section 2).
Key points
Peripheral vestibular nystagmus, especially its horizontal component, is suppressed by visual fixation; horizontal nystagmus that is not suppressed by visual fixation is not peripheral.
Nystagmus goggles remove visual fixation and allow the neurologist to see any peripheral vestibular nystagmus.
Nystagmus goggles come in different shapes and sizes from cheap, pocketable versions to expensive transportable versions; you can also make your own.
Examining a dizzy patient without using nystagmus glasses is like examining a weak patient without using a tendon hammer.
Footnotes
Contributors GMH drafted and finalised the manuscript, MS wrote sections of the manuscript and LAMcG collected and analysed data.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GMH and LAM have no conflicts to declare. MS is joint Chief Editor of the Journal of Neurology, Chief Editor of Frontiers of Neuro-otology and Section Editor of F1000. MS has received speaker’s honoraria from Abbott, Actelion, Auris Medical, Biogen, Eisai, Grunenthal, GSK, Henning Phrama, Interacoustics, MSD, Otometrics, Pierre-Fabre, TEVA, and UCB. MS is a shareholder of IntraBio. MS is the distributor of M glasses and acts as consultant for Abbott, Actelion, Ausric Medical, Heel, IntraBio and Sensorion.
Patient consent for publication Not applicable.
Provenance and peer review Commissioned; externally peer reviewed by Diego Kaski, London, UK.
Data availability statement All data relevant to the study are included in the article or uploaded as supplementary information.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Image of the moment
Other content recommended for you
- Penlight-cover test: a new bedside method to unmask nystagmus
- Dizziness demystified
- A practical approach to acute vertigo
- Assessment and treatment of dizziness
- Epley and beyond: an update on treating positional vertigo
- Vestibular reflexes and positional manoeuvres
- Bedside neuro-otological examination and interpretation of commonly used investigations
- Light cupula: the pathophysiological basis of persistent geotropic positional nystagmus
- Diagnostic value of nystagmus: spontaneous and induced ocular oscillations
- Click evoked myogenic potentials in the differential diagnosis of acute vertigo