Article Text

Abstract
Headache is a common neurological referral and a frequent cause for acute hospital admissions. Despite peripheral nerve blocks being widely used in headache and pain services to treat patients with headache disorders, there is no readily accessible resource with instructions for the delivery of peripheral nerve blocks. Here we provide a practical approach for administering peripheral nerve blocks and cover the current evidence base for such procedures in different headache disorders. We provide instructions and an audiovisual guide for administering greater and lesser occipital, supratrochlear, supraorbital and auriculotemporal nerves blocks, and give information on their adverse effects and potential complications. This information will provide a reference for headache practitioners when giving peripheral nerve blocks safely to people with headache.
- Headache
- migraine
- pain
Statistics from Altmetric.com
INTRODUCTION
Headache is one of the most prevalent, disabling and undertreated conditions in neurological clinical practice.1 Headache practitioners commonly administer peripheral nerve blocks to treat various headache disorders both in the acute and outpatient setting, often with rewarding results.2 There is no current national consensus on the technical aspects of delivering peripheral nerve blocks. However, a recent survey among UK headache practitioners showed that blocks have become relatively popular transitional treatments for cluster headache and chronic migraine.3 Here we aim to provide practical instructions for effective and safe delivery of the most common peripheral nerve blocks used in headache medicine. We briefly outline the evidence base for common indications and describe the peripheral nerve block method, including injection location, technique, drug constituents and potential pitfalls. This, together with the supplementary illustrative videos, should provide a comprehensive guide on nerve block delivery. This guide should be used to support, but not to replace, the experience obtained from clinical supervision by practised healthcare professionals.
EVIDENCE BASE FOR PERIPHERAL NERVE BLOCKS
Headache practitioners frequently target the greater occipital nerve (GON), but the treatment of both primary and secondary headaches might target other cervical and cranial nerves. Despite headache specialists seeing positive results in clinical practice, there is little high-quality information to support their widespread use.4
Several recent randomised controlled trials and cohort studies have studied the efficacy of peripheral nerve blocks, particularly GON blocks. The level of evidence for the effectiveness of peripheral nerve blocks for managing different headache disorders varies depending on the pericranial nerve targeted and the outcome measure used (table 1). GON blocks for the acute and preventative treatment of migraine and cluster headaches reduce headache days and give high levels of patient-reported efficacy.5 6 Furthermore, peripheral nerve blocks have been effective in managing acute or prolonged migrainous episodes that commonly present to the emergency department.7 8 The rapid onset of pain relief provided by anaesthetic nerve blocks makes them ideal for acute headache presentations, where timely management is essential, reducing the need for opiate-based therapies.
Evidence base for the efficacy of peripheral nerve block in treating different headache disorders
Although it is difficult to predict which patients will benefit significantly from peripheral nerve blocks, headache practitioners have developed a wealth of clinical experience in maximising their efficacy. In the trigeminal autonomic cephalalgias—predominantly unilateral headaches including cluster headache and hemicrania continua—ipsilateral greater and lesser occipital nerve (LON) blocks as first-line treatments may avoid the need for corticosteroids or indometacin. Patients with headache who have reproducible pain with palpation over the pericranial nerve area in the scalp, and those with localised cutaneous allodynia, are also likely to respond to nerve blocks.7 18 Peripheral nerve blocks are also demonstrably effective in the older population with headache disorders, whose comorbidities might preclude the use of first-line preventative medications.6 There are conflicting results about adding corticosteroid to nerve blocks in people with migraine, but evidence to support its efficacy in cluster headache.11 14 19 Greater occipital neuralgia with or without another coexisting headache disorder is not uncommon.20 Giving a GON block to a patient with suspected GON neuralgia can be both diagnostic and therapeutic, usually conferring prolonged relief. The evidence base for using peripheral nerve blocks in other cranial neuralgias, such as auriculotemporal and supraorbital neuralgias, is predominantly anecdotal, from published case series.15 16 Pregnant women with troublesome headaches can often be managed throughout pregnancy and the post-partum period with anaesthetic nerve blocks without corticosteroid, reducing the need for medications. The frequency of the nerve blocks can be tailored to the individual’s response duration but is usually 3 months or more. If the benefit lasts less than 2 months, then clinicians might consider other headache medications or interventions.
Some headache practitioners inject only the occipital nerves during the first session, which reduces the number of injections and allows for an assessment of initial response. If the patient reports some benefit but has residual facial pain, then at a subsequent session, the trigeminal nerves can be blocked as well as the occipital nerves. Consensus recommendations by the American Headache Society and the Spanish Headache Study Group have used this evidence base to provide guidance on the administration of peripheral nerve blocks for different headache disorders.21 22
GENERAL CONSIDERATIONS
Knowledge of the anatomical landmarks of the occipital and superficial branches of the trigeminal nerve is important for effective nerve blockade, and to avoid possible complications such as nerve trauma, bleeding or inadvertent arterial injection of anaesthetic drug. People with headache disorders often describe pain over the forehead, behind their eyes, temples, occipital and upper cervical areas. The forehead and upper periocular areas are innervated by peripheral branches of the first division of the trigeminal nerve (V1), mainly the supraorbital and the supratrochlear nerves. The temples are largely innervated by the auriculotemporal nerve branch from the mandibular division of the trigeminal nerve (V3). The upper cervical and occipital region is innervated by C2/C3 posterior cervical branches, mainly the greater, lesser and third occipital nerves.23
Having identified someone as suitable for a peripheral nerve block, we find it helps to show them an illustration of the peripheral cranial nerve to be injected (figure 1). The written consent should include the known complications of any invasive procedure, such as bleeding or infection at the injection site, and some may find the procedure painful. Peripheral nerve blocks are contraindicated at any previous surgical site, for example, previous burr hole or craniotomy, as there is a risk of anaesthetic infiltration into the central nervous system. Blocks should also be routinely avoided in patients with implants such as nerve stimulators or shunts, although in exceptional circumstances can be used in skilled hands with appropriate consent for risks. Following the informed consent process, patients are asked either to lie in a supine position on the examination bed or to sit on a chair, depending on the superficial nerve being injected. Patients should also be advised to eat and drink before attending for the procedure, to reduce the chances of a syncopal episode. As with any invasive procedure, clinicians should take care to confirm the patient’s details and site to be blocked, while adhering to the local personal protection equipment guidance. Topical anaesthetic cream a few minutes before the procedure can be used to numb the skin around the injection site, especially for the supraorbital, supratrochlear and auriculotemporal nerve injection sites. Most people develop numbness in the distribution of the nerve injected within a few minutes after the procedure, and warning patients of this anticipated effect can alleviate postprocedure anxiety. Furthermore, numbness in the dermatomal distribution of the nerve injected is a sign that the procedure has infiltrated the targeted nerve. The constituents of the nerve block differ with the cranial nerve injected and between headache centres (table 2). Corticosteroids are commonly used only for GON blocks, but some headache centres use them to infiltrate the LON as well. We recommend avoiding corticosteroids for any of the trigeminal nerve blocks, particularly due to unwanted cosmetic side effects such as localised alopecia and lipoatrophy.24 The systemic effects of corticosteroids in peripheral nerve blocks are not negligible and there have been reported cases of iatrogenic Cushing’s syndrome both in the literature and anecdotally among headache centres.25 For this reason, it is important to ask the patient about other corticosteroid medications they might be receiving; patients already taking corticosteroids should not receive a repeat corticosteroid-containing nerve block within 3 months or longer. Peripheral nerve blocks appear generally safe, but there are other contraindications and possible complications to take into account, depending upon which cranial nerve is being blocked (table 3).
Constituents and volumes for individual nerve blocks
Common pitfalls and solutions for the safe administration of peripheral nerve blocks
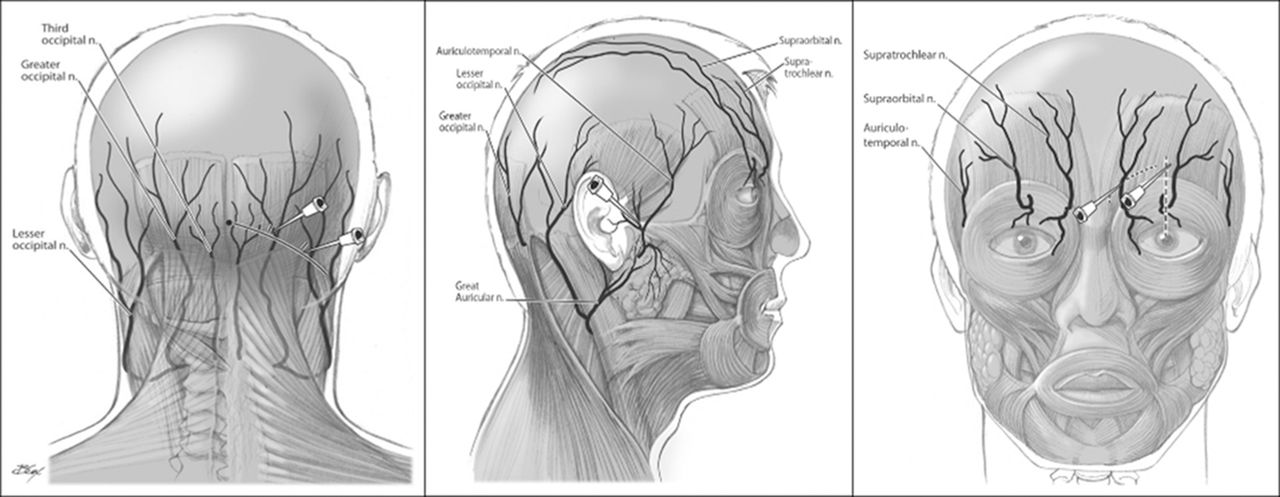
Illustrative drawings of the anatomical course of the peripheral cranial nerves. These are used during the consent process to demonstrate the location of the nerves to be injected. Adapted with permission from Blumenfeld et al.21
GON BLOCKS
The GON arises as the medial branch from the dorsal primary ramus of the second cervical nerve. It emerges below the obliquus capitis inferior muscle and passes through the semispinalis muscle, before ascending to innervate the posterior scalp to the vertex.29 The GON can be localised superficially by identifying a point one-third (medially) of the way between the occipital protuberance (inion) and the mastoid process, approximately 2 cm lateral and 1.5–2.0 cm below the inion (figure 2). The occipital artery usually runs lateral to the GON, and this should be considered when injecting the nerve.
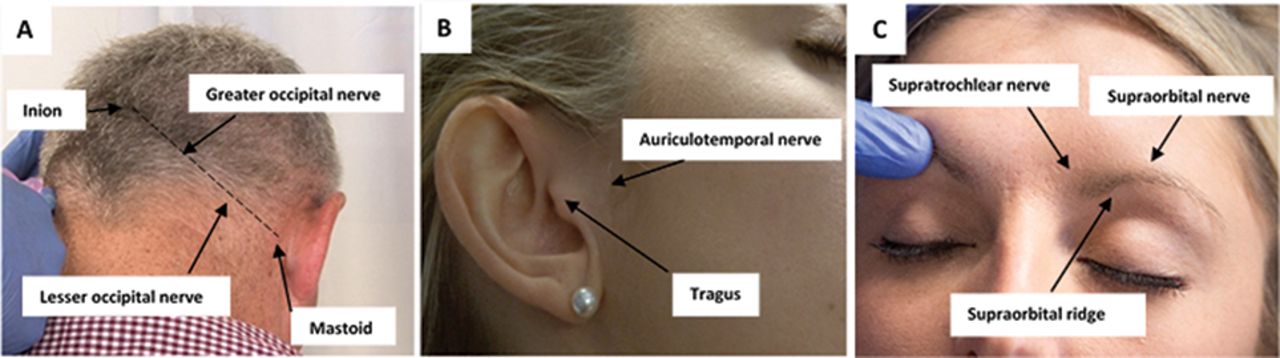
Superficial anatomical landmarks for the main cranial nerve blocks. (A) Superficial points for the greater and lesser occipital nerve blocks. (B) Location of the auriculotemporal nerve block. (C) Superficial points for the supratrochlear and supraorbital nerve blocks.
Injection technique
The patient should be comfortably seated on a chair with the head slightly flexed, and the clinician standing behind. Locate the GON, and if needed use topical anaesthetic cream before the injection. Use a 5 mL syringe with a 25-gauge needle. Gently insert the needle perpendicular to the skin, until meeting firm resistance, indicating the needle tip is at the periosteum. This helps to ensure there is no skull defect that might precipitate intracerebral infiltration of the anaesthetic. Withdraw the needle slightly and aspirate to confirm no arterial drawback. Then, redirect the needle slightly superiorly and gently inject the solution in a fanlike distribution (figure 3). Some practitioners inject the solution with the needle in the same position, which is sufficient if injecting a reasonable volume of anaesthetic. The patient may feel a burning sensation as the anaesthetic is infiltrated, but this should subside in a few minutes once the anaesthetic takes effect. Withdraw the needle and apply pressure to the site with gauze to minimise bleeding (online supplemental file 1). If the patient has had previous vasovagal episodes due to pain or previous injections, we recommend performing the injection with the patient in a lateral decubitus position, which will help avoid a sudden fall in blood pressure and hence a sudden decrease in cerebral perfusion pressure.

{kind=link}
{kind=link}
{kind=link}
Still images illustrating the injection sites of the peripheral nerve blocks. Videos with commentary for these nerve blocks are available in the online supplemental file. (A) Greater occipital nerve blocks. (B) Lesser occipital nerve block. (C) Supratrochlear nerve block. (D) Supraorbital nerve block. (E) Auriculotemporal nerve block.
Supplemental material
LON BLOCKS
The LON arises from the ventral primary rami of the second and third cervical nerves. It passes superiorly along the posterior border of the sternocleidomastoid muscle, dividing into cutaneous branches that innervate the lateral portion of the posterior scalp.29 The LON is localised by identifying a point two-thirds of the way between the inion and the mastoid process (figure 2). It is commonly injected along with the GON.
Injection technique
The procedure is broadly similar to the GON injection with the patient seated and clinician standing behind. Having located the LON, use a suitable 25-gauge needle, entering perpendicular to the skin, stopping once the periosteum is reached. After gentle aspiration to ensure no arterial entry, the injection is delivered (figure 3) (online supplemental file 2)
Supplemental material
SUPRATROCHLEAR NERVE BLOCKS
The supratrochlear nerve is one of the terminal cutaneous branches of the frontal nerve, which in turn arises from the ophthalmic division of the trigeminal nerve (V1). The supratrochlear nerve exits the orbital cavity anteriorly and ascends the forehead to innervate the upper eyelid, forehead and anterior scalp.29 It is located superficially at the superomedial aspect of the supraorbital ridge, which is the injection site (figure 2).
Injection technique
Position the patient supine with their head in a neutral position. From here, the clinician, standing beside the patient, has easy access to the supratrochlear nerve. Use a 1.0 or 2.5 mL syringe with a 30-gauge needle. Locate the nasal bridge and the medial aspect of the supraorbital ridge. Gently insert the needle at the medial aspect of the corrugator muscle, just lateral to the procerus and above the eyebrow line to a depth of 4–5 mm. Gently aspirate to ensure no arterial flashback and then inject the solution, which will produce a small weal under the skin (figure 3) (online supplemental file 3).
Supplemental material
SUPRAORBITAL NERVE BLOCKS
The supraorbital nerve is the larger of the terminal cutaneous branches of the frontal nerve and runs through the supraorbital notch to innervate the upper eyelid and conjunctiva. It then ascends the forehead, being closely associated medially with the supraorbital artery. The supraorbital nerve is located just above the supraorbital notch (figure 2).
Injection technique
With the patient supine and their head in a neutral position, palpate the supraorbital notch. Use a 1.0 or a 2.5 mL syringe with a 30-gauge needle. Insert the needle perpendicularly, just above supraorbital notch (avoid injecting into the supraorbital notch), to a depth of 4–5 mm. Gently aspirate to confirm no arterial entry and then inject the solution (figure 3) (online supplemental file 4).
Supplemental material
AURICULOTEMPORAL NERVE BLOCKS
The auriculotemporal nerve arises as a posterior division of the mandibular branch of the trigeminal nerve. It innervates the temples and the temporomandibular joint. Its superficial branches innervate the tragus and the auricle of the ear; its proximal trunk is located superficially just anterior to the tragus (figure 2).29
Injection technique
The positioning for this nerve injection can be with the patient seated and physician standing beside them, or with the patient supine and their head in a neutral position. At the point just anterior to the tragus, use a 5 mL syringe with a 30-gauge needle to infiltrate 1–2 mL into the subcutaneous tissue to a depth of about 4–6 mm. After gentle aspiration to exclude any arterial flashback, inject the solution (figure 3) (online supplemental file 5).
Supplemental material
CASE STUDIES
Case 1
A 26-year-old woman was referred to the headache clinic when 4-weeks pregnant. She had a lifelong history of episodic migraine headaches with and without aura, which had transformed into daily headaches in the previous 3 weeks. She also described shooting pains over the right occipital region. The headaches were predominantly right sided associated with allodynia over the right forehead and the right occipital region was tender. Her headaches had previously responded poorly to propranolol and she had stopped her current prophylactic, amitriptyline, on finding she was pregnant. Her Headache Impact Test (HIT6) score was 72 on presentation. The HIT6 score is a headache score between 36 and 78, which measures headache burden, with higher scores demonstrating a worse outcome.
After discussion, she opted for peripheral nerve blocks as a transitional migraine treatment. She underwent bilateral GON blocks with anaesthetic only, and right-sided supraorbital, supratrochlear and auriculotemporal blocks. There was sustained improvement in her migraine for 7 weeks, with an HIT6 score of 48 after 4 weeks. She continued the same combination of peripheral nerve blocks every 3 months throughout her pregnancy.
Case 2
A 40-year-old man was referred to the nerve block clinic with a 5-year history of seasonal stereotyped left hemicranial stabbing pains lasting about 2 hours, with occasional neuralgia affecting the left trigeminal nerve maxillary division (V2). There were associated left trigeminal autonomic symptoms including conjunctival injection, eye redness, lacrimation and nasal congestion. He was restless during these episodes, which occurred up to three times a day during the winter months, over a few weeks. Oxygen treatment and triptans had previously helped. He also had a history of left temporomandibular joint pain and previous episodic migraine. He had tried topiramate, verapamil and propranolol but had stopped this due to symptomatic bradycardia. Investigations were normal, including intracranial imaging looking for secondary causes. On examination, there was tenderness of the left greater and LON area, as well as left temporomandibular joint clicking and tenderness. We established the diagnoses of cluster headache and co-existing left temporomandibular joint dysfunction. The baseline HIT6 score was 78.
Due to his frequent cluster attacks and temporomandibular joint pain, we offered a left GON block with corticosteroid, and left lesser occipital, supraorbital, supratrochlear and auriculotemporal nerve blocks. On follow-up at 12 weeks, he reported a favourable response with only three further cluster attacks that had responded to sumatriptan injection rescue therapy.
CONCLUSION
Peripheral nerve blocks are effective in the acute and preventative management of several headache disorders. It is difficult to identify those who will respond best, but the procedures allow an interventional approach for those with troublesome and refractory headache. Neurologists can administer these blocks as a day procedure, in clinic or the emergency department, where quick pain relief can provide a satisfactory outcome.
Key points
Peripheral nerve blocks have a role in acute and transitional treatment of acute migraine, chronic migraine, cluster headache and painful cranial neuralgias.
Patient position and anatomical landmarks are key for their successful delivery.
Corticosteroids are frequently used for greater occipital nerve blocks but may also be used for lesser occipital nerve blocks.
Supraorbital, supratrochlear and auriculotemporal nerve blocks involve a combination of lidocaine and/or bupivacaine.
Uncommon but important adverse effects include transient dizziness, light-headedness, transient headache exacerbation, and rarely localised lipoatrophy and alopecia with corticosteroids.
FURTHER READING
Blumenfeld A, Ashkenazi A, Napchan U, et al. Expert consensus recommendations for the performance of peripheral nerve blocks for headaches—a narrative review. Headache J Head Face Pain 2013;53:437–46. doi:10.1111/head.12053.
Levin M. Nerve blocks in the treatment of headache. Neurotherapeutics 2010;7:197–203. doi:10.1016/j.nurt.2010.03.001.
REFERENCES
Footnotes
Contributors LF drafted the manuscript, edited and narrated the illustrative videos, and revised the manuscript for intellectual content. MR edited and revised the manuscript for intellectual content. LI produced the illustrative videos, edited and revised the manuscript for intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Consent for patient illustration and supplemental videos has been obtained.
Provenance and peer review Commissioned. Externally peer reviewed by Nick Silver, Liverpool, UK.
Data availability statement All the content, figures, tables and videos in the manuscript are available to all the authors.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Editors’ commentary
Other content recommended for you
- What is new in migraine management in children and young people?
- Greater occipital nerve block modulates nociceptive signals within the trigeminocervical complex
- Shot in the dark: three patients successfully treated with onabotulinumtoxin A injections for relief of post-traumatic chronic headaches and dystonia induced by gunshot wounds
- Postdural puncture headache in the obstetric population: a new approach?
- Effectiveness and safety profile of greater occipital nerve blockade in cluster headache: a systematic review
- Greater occipital nerve block using local anaesthetics alone or with triamcinolone for transformed migraine: a randomised comparative study
- Update on corneal neurotisation
- Debunking myths in headache diagnosis for the pain practitioner
- Headache management: pharmacological approaches
- 365 Greater occipital nerve block as a treatment for paediatric migraines