Article Text

Statistics from Altmetric.com
Introduction
Neurologists are familiar with the standard definition of apraxia: ‘an inability to perform a motor task that cannot be adequately explained by motor weakness, sensory loss or a lack of understanding’. Being a definition of exclusion, this has led to a bewildering number of motor disorders being described as forms of apraxia, despite many of these failing to capture the essence of what apraxia really is: a disorder of motor cognition. Apraxia reflects an impairment of the storage and transformation of motor representations in the brain, either through degradation of the semantic knowledge of gestures and tool use or through inability to translate the neural representations of higher level goals accurately into lower level patterns of muscle activation and inhibition.
Apraxia
Our current clinical approach to apraxia is similar to that proposed by Liepman in the early 20th century.1 He recognised that left hemispheric lesions tend to cause bilateral upper limb apraxia and suggested a model of motor control in which the left parietal lobe stores a ‘space–time form picture’ of a movement. For a movement to be executed, its picture must be retrieved and activated and then be associated via cortical projections with the relevant motor engrams in the prefrontal regions. From here the information passes to the primary motor cortex before being fed down the corticospinal tracts. For the right upper limb to move the information remains contained within the left hemisphere, but for the left upper limb to move the information from the left parietal lobe must first be sent to the right prefrontal and frontal regions through the corpus callosum.
Using this scheme, Liepman delineated three forms of apraxia. He described ideational apraxia as a disruption of the space–time picture, in which the idea of the movement itself is lost or degraded. In ideomotor apraxia, the idea of the movement is intact but there is an inability to map this accurately on to the motor engrams in the frontal lobes. The disruption of these engrams leads to ‘melokinetic’ apraxia (now called limb-kinetic apraxia, see below), a disturbance of fine motor control. Ideational apraxia is therefore secondary to a disturbance of the conceptual motor system and both ideomotor and limb-kinetic apraxia result from disturbances of the action production system.
Ideational apraxia
In ideational apraxia, the concepts of movement and intent are degraded and patients may not comprehend the appropriate use for a tool.2 Patients presented with a pair of scissors, for example, can name the object correctly but may be unable to describe their use. When the examiner demonstrates their use, patients may be unable to discriminate between poorly executed movements and properly executed movements. When handed the item themselves, they may struggle to use them to cut a sheet of paper. This demonstrates a loss of the conceptual or semantic knowledge about what scissors are and what they are for.
As a result, patients with ideational apraxia also cannot pantomime tool use to command. They may also have lost the basic semantic knowledge underlying simple gestures and may be unable to show how to wave goodbye or how to beckon somebody over. Because the action production system remains intact, such patients should be able to perform these tasks when the examiner gives them a visual demonstration.2 In practice, however, any lesion or degenerative process affecting the conceptual motor system often also affects the action production system, and so they may not necessarily show this dissociation.
Distinguishing between ideational and ideomotor apraxia does not help with lesion localisation. While the inferior parietal lobe is more associated with the conceptual motor system,3 a lesion here does not convincingly correlate with ideational apraxia; similarly, although the superior parietal lobe is more associated with the action production system,3 lesions here do not correlate with the emergence of ideomotor apraxia.1
Patients with ideational apraxia are often very disabled and struggle greatly when trying to carry out the basic activities of daily living.4 It commonly develops in people with advanced Alzheimer's disease (who often also have memory and language disturbance) and in people with a left hemispheric stroke (who often also have dysphasia and hemiplegia).
What is described above amounts to a disruption of movement concepts and so some authors describe this type of deficit as ‘conceptual apraxia’; confusingly, they use ‘ideational apraxia’ instead to refer to an inability to link together complex sequences of tasks when pursuing an overall goal, making a cup of tea for example. However, others consider such difficulties to be a manifestation of the action production system, and classify this deficit as a form of ideomotor apraxia. As discussed below, the practical neurologist can reasonably sidestep these issues by staying away from this terminology entirely!
Ideomotor apraxia
Ideomotor apraxia is a disorder of the action production system. Affected patients display errors in the scaling, timing and orientation of movements and may also omit or repeat individual elements of the overall action being assessed. They struggle to generate meaningful and arbitrary hand postures and often perform poorly when asked to pantomime an action. A common error is the ‘body-part-as-object error’, where the patient substitutes a body part for the tool in question when asked to pantomime a particular action. Examples include brushing the fingers through the hair when asked to demonstrate how it should be combed and to rub a finger against the teeth when asked to demonstrate how to use a toothbrush. These errors can also occur in healthy people and they should only be considered pathological if they persist after they have been highlighted to the patient. Despite these difficulties, the goal of the action can usually be recognised, and a typical feature is that the patient's performance significantly improves if they are given the object they have just been asked to pantomime;5 because there is an intact representation of the overall goal of the action, having the visual and tactile feedback associated with natural use of an object improves the selection of an appropriate limb posture and finger configuration. As a consequence, patients with ideomotor apraxia are potentially less disabled than those with ideational apraxia. While it was previously felt that the disorder was mainly something identifiable only on clinical examination and with little impact on day-to-day function, this is not necessarily the case; it often causes significant functional impairment.6
Limb-kinetic apraxia
As well as introducing the terms ideational and ideomotor apraxia, Liepman also described ‘melokinetic’ apraxia, where the overall ‘melody’ of a complex movement is lost. It was subsequently renamed limb-kinetic apraxia, the characteristic feature of which is the loss of co-ordination between the fine, individuated finger movements that are required to perform a skilled task. This is brought about by disruption of the final stages of motor processing in the prefrontal regions before the information is relayed to the ipsilateral primary motor cortices. As such, a lesion affecting one prefrontal lobe or its connections causes limb-kinetic apraxia in the contralateral upper limb.
This form of apraxia has been largely neglected as it is often considered to be a pure dexterity problem rather than a true apraxia,7 though it is a disorder of motor control situated firmly ‘above’ the pyramidal and extrapyramidal systems. Another likely reason for its relatively low profile is that any lesion affecting the prefrontal motor cortex also likely disrupts the integrity of the corticospinal tract, so muscle weakness often overshadows any higher level disorder of motor control. The term is therefore not widely used, but there has been renewed interest in this area with the realisation that many patients with corticobasal syndrome have limb-kinetic apraxic deficits.8 It often manifests early in the disease course and the neurologist should suspect it if a patient struggles to produce any form of rhythmical opposition of their index finger and thumb when testing for bradykinesia. Sometimes it is more easily demonstrated by asking the patient to oppose their thumb to their index, middle, ring and little fingers rapidly in turn. Because patients with limb-kinetic apraxia cannot easily produce individuated finger movements they, like patients with ideomotor apraxia, also have significant difficulty in imitating meaningless hand gestures.9 While limb-kinetic apraxia is often a striking feature of corticobasal syndrome, it often coexists with both ideomotor and ideational apraxia.8
Apraxia of speech and buccofacial apraxia
Speech production requires the transformation of the neural representation of a grammatical sentence into a precise pattern of orofacial muscular activity; the disruption of this process is termed apraxia of speech.10 Patients with apraxia of speech have very slow, deliberate, effortful speech. They may make errors in the shape, ordering and timing of the production of individual syllables and may display ‘articulatory groping’, repeatedly correcting themselves while trying to find the right word or sound. They also have greatly impaired prosody of speech, such that it loses its natural rhythm, intonation and overall melody. While no single brain region is exclusively involved, apraxia of speech strongly associates with lesions of the left inferior frontal gyrus and the left anterior insular.11 It usually occurs in patients with either stroke or progressive non-fluent aphasia, and so there is often some coexistent dysphasia. Distinguishing apraxia of speech from dysphasia can be challenging (and beyond the scope of this article), though identifying buccofacial apraxia (see below) generally suggests that apraxia of speech is significantly contributing to any speech disturbance.
It may also be difficult to differentiate apraxia of speech from dysarthria, though when asked to repeat a single syllable (eg, ‘pa, pa, pa, …’) patients with dysarthria often make errors in timing and pronunciation, whereas patients with apraxia of speech usually manage the task with little difficulty. However, they then often struggle significantly when asked to string a number of syllables together (eg, ‘pa-ta-ka, pa-ta-ka, …’).10 Another helpful clue is that patients with dysarthria might mispronounce words in a consistent manner, whereas pronunciation errors in patients with apraxia of speech vary considerably from one use of a particular word to the next.
Buccofacial apraxia refers to an inability to perform skilled non-speech-related movements involving the muscles of the tongue and face; it is associated with lesions in the ventral premotor cortex. Its assessment involves asking the patient to cough or to click their tongue and to demonstrate how they would drink through a straw or blow out a match. While it can occur in isolation, it almost always coexists with apraxia of speech and/or dysphasia.
Examining a patient for apraxia
Before beginning to assess for the presence of apraxia, the clinician should undertake a careful neurological examination to ensure that the patient's motor symptoms cannot be explained by muscle weakness, spasticity, bradykinesia, ataxia or sensory loss. Below is a scheme for examining for apraxia in which the patient is asked to pantomime tool use, generate meaningful and meaningless hand gestures and perform a motor sequencing task (see table 1).12
A schema for examining praxis
This basic examination sequence has evolved because specific patterns of impairment can help to classify the apraxia into one of the three categories described above, though in practice most patients with apraxia show deficits in both the conceptual and production systems. Given that there is also no universal acceptance of the definition of these terms (ie, is ideational apraxia a ‘conceptual’ apraxia or is it an inability to sequence motor tasks?), there is a strong argument for omitting them from any description of an apraxia patient. So while one can carefully attempt to work out the anatomical and pathological significance of any possible dissociations observed while assessing the distinct actions listed above, it is probably best simply to think of this repertoire of tests as providing a means of testing the action production system in a wide variety of ways.
When it comes to documenting one's findings, it is therefore sufficient simply to describe the body part affected and the movements that are impaired.13 Despite this simplified approach, there is still some practical merit in understanding that a patient with marked asymmetrical hand clumsiness (manifesting as a striking inability to mimic arbitrary postures) may well have limb-kinetic apraxia; this should point the neurologist to the possibility of corticobasal syndrome.
A sensible starting point in the examination scheme is to watch the patient pantomime tool use by issuing a command such as ‘Pretend you have a hammer in your hand and show me how you would hammer in a nail’. Other useful pantomimes include asking the patient to show how they would use a pair of scissors, use a bottle opener or brush their teeth. Mistakes should only be considered pathological if they persist despite correction. If the actions are defective when produced to command, then the examiner could consider demonstrating the correct pantomime and then asking the patient to imitate them. The idea is that a patient with ideational apraxia may be unable to demonstrate the action because they have lost the semantic memory associated with the tool, but if they can see how it should be used then they can still access their largely intact action production system to then produce a good imitation. However, for the reasons described above, there is rarely such a neat dissociation in clinical practice.
The patient should then be asked to demonstrate several meaningful hand gestures, which could include waving goodbye, beckoning ‘come here’, saluting and hitching a lift. If testing for buccofacial apraxia, then the clinician might ask the patient to cough, lick their lips and show how they would drink through a straw or blow out a match.
Because the conceptual and action production systems are usually localised in the left hemisphere, most patients who show deficits in pantomiming tool use and in producing meaningful gestures have a left hemispheric lesion and have bilateral apraxia.
The examiner might then ask the patient to imitate some arbitrary hand positions (figure 1 gives examples). Gestures should be presented to the patient in a mirror-like fashion in that when assessing a patient's left hand, the examiner demonstrates with their own right hand. Difficulty in this task can be a manifestation of limb-kinetic apraxia9 and, because this can be secondary to a unilateral frontal lobe lesion, this should be assessed in both hands.
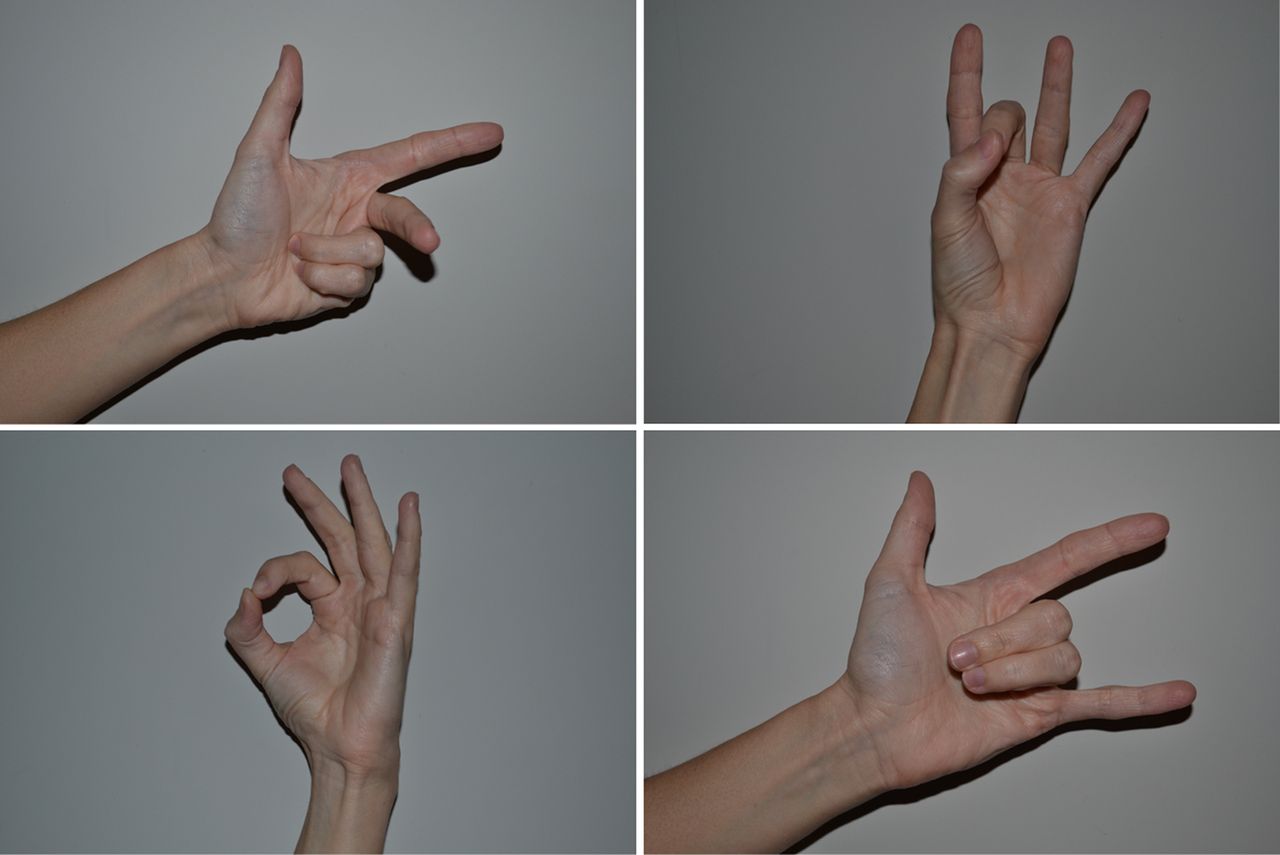
Examples of arbitrary hand postures to present when assessing a patient for apraxia. Adapted from Goldenberg.19
The assessment should finish with a sequencing task such as Luria's three-step command. The examiner should alternately tap a surface with the side of their fist, the edge of their hand and the palm of their hand (figure 2) several times before asking the patient to do the same. While this task clearly tests the integrity of the action production system, a poor performance might also result from impaired working memory or executive function.

The three hand positions comprising Luria's three-step sequencing task.
Other forms of apraxia
As described above, the traditional definition of apraxia is an inability to perform a motor task that cannot be adequately explained by motor weakness, sensory loss or a lack of understanding. Generally speaking, however, apraxia is taken to be an inability to perform skilled motor tasks secondary to a disturbance of higher level motor function. Thus, several disorders originally labelled as forms of apraxia are no longer universally considered to be so.
Constructional apraxia is an inability to copy drawings or 3D structures accurately. The underlying problem, however, is with visuospatial processing and not with higher level motor control, and so this should not be regarded as a true apraxia. Likewise, patients with dressing apraxia lack the visuospatial capacity required to orientate items of clothing correctly with respect to themselves.
Patients with apraxia of eyelid opening are transiently unable to open their eyelids. The precise mechanism remains uncertain but it is probably a disorder of the supranuclear control of eyelid elevation that requires the simultaneous activation of levator palpebrae superioris and inhibition of orbicularis oculi.14 While this is indeed probably a disorder of higher level motor control, the act of opening one’s eyes is largely automatic and in no way skilled; thus, most authorities would not consider this to be a true apraxia. Because it seems to be caused by the abnormal co-contraction of agonist and antagonist muscles, it is probably best considered as a form of dystonia and indeed, many patients with apraxia of lid opening also have blepharospasm.15
Oculomotor apraxia is an inability to generate voluntary saccades to a visual target. Its basis is an inability to direct visual attention to the appropriate part of the outside world due to impaired function of the posterior parietal regions.16 While this ultimately manifests as a motor deficit, it is not secondary to a disturbance of higher level motor control and so is not a true apraxia.
Gait apraxia has been defined as ‘the loss of ability to properly use the lower limbs in the act of walking, which cannot be accounted for by demonstrable sensory impairment or motor weakness’.17 Its characteristic features are slow speed, short steps, hesitancy, a wide base and freezing of gait. Such a gait generally results from bilateral cerebral disease and frequently occurs in normal pressure hydrocephalus, Alzheimer's disease and diffuse cerebrovascular disease. Many affected patients therefore have global cognitive impairment along with pyramidal and extrapyramidal signs, though they often do not have coexistent upper limb apraxia. As such, its classification as an apraxia (a disorder of pure higher level motor control) has been challenged and the term high-level gait disorder has been proposed in its place.18
Case 1
A 64-year-old man was referred to neurology with a 6-month history of progressive ‘weakness’ of his left, dominant hand. He described increasing difficulty in numerous activities of daily living, including writing, using a knife and fork and fastening buttons. His wife reported that his thinking and speech had slowed down but that he could still remember the details of day-to-day events and conversations.
On examination, there was mild hypomimia, with diminished arm swing on the left but an otherwise normal gait. His pursuit eye movements were broken but with no nystagmus and with normal saccades. There was no tremor of the limbs, no dystonia and no muscle weakness. There was mild rigidity of the right upper limb and severe rigidity of the left upper limb. There was mild bradykinesia in the right hand but he could not produce ordered repetitive movements with his left hand. He was completely unable to imitate arbitrary hand postures with his left hand but had only mild difficulty with his right hand. When asked to pantomime brushing his teeth, he rubbed the side of his teeth to-and-fro with the side of his left index finger. He could easily demonstrate a salute but struggled to perform a beckoning motion with his left index finger and made frequent errors when attempting Luria's three-step command.
This man was parkinsonian and had severe apraxia of his left upper limb. This manifested primarily as a lack of dexterity and neurological examination identified a prominent limb-kinetic apraxia. An MR scan of brain showed mild generalised atrophy with more focal atrophy of the right parietal lobe (figure 3). His symptoms did not respond to levodopa and we diagnosed corticobasal syndrome.

{kind=link}
{kind=link}
{kind=link}
MR scan of brain (coronal sections of fluid attenuation inversion recovery (FLAIR) sequences) in a patient with corticobasal syndrome, showing generalised atrophy, with the right parietal region being more severely affected.
Case 2
A 74-year-old woman had a long history of cognitive impairment. For 2 years, she had increasingly struggled to remember the details of day-to-day events and more recently had developed word-finding difficulties. Over the preceding few months, she had relied more on her husband for assistance with basic activities of daily living and now could not make a cup of tea, use a knife and fork or use any household appliance.
A routine neurological examination was difficult due to an inability to co-operate with basic motor commands, but was normal apart from broken pursuit eye movements and a positive grasp reflex. When asked to pantomime combing her hair, she waved her open palm over her face; when asked to pantomime cleaning her teeth, she slowly moved the palm of her hand across her lips while her mouth was closed. She could wave goodbye but could not salute to command. With difficulty she could orientate some of her digits to match the examiner's arbitrary hand postures.
This woman has severe apraxia in the context of progressive amnesia and language disturbance and has a diagnosis of Alzheimer's disease. Her extremely poor performance at pantomiming simple activities suggests that she has little conceptual understanding of the actions required and that she has an ideational apraxia. Her deficits probably represent the downstream effect of a defective conceptual motor system, but she most likely also has a degree of ideomotor apraxia. The label of ideational apraxia would be more secure if we had shown that she could not use a toothbrush or comb when presented with these, but such a distinction would probably not have affected her diagnosis or treatment.
Key points
Apraxia is an inability to perform skilled motor tasks secondary to a disturbance in the processes of higher level motor control.
In ideational apraxia, the concepts of movement and intent are degraded and patients may not comprehend the appropriate use for a tool.
In ideomotor apraxia, patients cannot convert the neural representation of an idea or goal into a precise pattern of motor activity and so make errors in the scaling, timing and orientation of movements.
In limb-kinetic apraxia, there is a breakdown in fine individuated hand movements, often from a lesion in the contralateral prefrontal cortex or associated subcortical pathways; it is frequently very prominent in patients with corticobasal syndrome.
These forms of apraxia can be difficult to disentangle in clinical practice; a practical solution is simply to interrogate the action production system by asking the patient to perform a wide variety of motor tasks.
Acknowledgments
The author thanks Dr Anaïs Thouin for her helpful comments on the manuscript.
References
Footnotes
Competing interests None declared.
Provenance and peer review Commissioned; externally peer reviewed. Commissioned; reviewed by Masud Husain, Oxford, UK.
Linked Articles
- Editors' commentary
Other content recommended for you
- Corticobasal syndrome: a practical guide
- Utility of testing for apraxia and associated features in dementia
- Apraxia: another view
- Brain activation during ideomotor praxis: imitation and movements executed by verbal command
- Lateralised motor control: hemispheric damage and the loss of deftness
- Biparietal variant of Alzheimer's disease: a rare presentation of a common disease
- Apraxia, agnosias, and higher visual function abnormalities
- Corticobasal syndrome due to a thalamic tuberculoma and focal cortical atrophy
- Pure apraxic agraphia with abnormal writing stroke sequences: report of a Japanese patient with a left superior parietal haemorrhage
- Assessing the dysexecutive syndrome in dementia