Article Text

Statistics from Altmetric.com
A 53-year-old woman presented with acute onset of bifrontal headache with fever and vomiting, and a 6-week history of unilateral, left-sided, clear, salty rhinorrhoea. She worked as a veterinary pathologist. On examination, her neck movements were painful, but there were no localising neurological signs. She was obese with a body mass index of 36.5 kg/m2(height 162 cm, weight 96 kg). Cerebrospinal fluid (CSF) examination identified a pleocytosis with a white cell count of 2910/µL (≤5), 91% polymorphs and 9% lymphocytes. The level of CSF glucose was low at 3.9 mmol/L, with a CSF/serum ratio of 0.66. CSF protein was markedly raised at 3.38 g/L (0.15–0.45). We made a presumptive diagnosis of bacterial meningitis and started antimicrobial cover as per local guidelines. This did not include corticosteroids or anti-tuberculous therapy.
Given her occupation, and recent travel to Yosemite National Park, California, we excluded an extensive list of pathogens. CSF PCR was negative for Neisseria meningitidis, Streptococcus pneumoniae, Escherichia coli, Streptococcus agalactiae, Haemophilus influenzae, Listeria monocytogenes, cytomegalovirus, enterovirus, herpes simplex virus type 1 (HSV-1) and type 2 (HSV-2), human herpesvirus 6, varicella zoster virus, human parechovirus and Cryptococcus neoformans. There was no serological evidence of hantavirus, Rickettsia, Treponema pallidum, Borrelia burgdorferi, Leptospira, Histoplasma, Coccidioides or Brucella. Beta-(1,3)-d-glucan and cryptococcal antigens were negative in both serum and CSF samples. Serum Aspergillus antigen (galactomannan) was also negative.
Chest X-ray identified a coexisting right basal pneumonia, confirmed on CT scan of thorax, which also showed evidence of prior granulomatous disease. She was known to have a reactive Mantoux, from occupational screening many decades previously. QuantiFERON-TB Gold was positive, but extended mycobacterial cultures on CSF and bronchoalveolar lavage were negative. Investigative work-up for granulomatous disease showed serum ACE of 38 IU (8–65), adjusted serum calcium of 2.36 mmol/L (2.25–2.59), erythrocyte sedimentation rate of 11 mm/hour (1–20), negative anti-neutrophil cytoplasmic antibody and normal serum immunoglobulins. Bronchoscopy was macroscopically normal. Bacterial culture and PCR on bronchoalveolar lavage fluid were negative.
A follow-up CT scan of thorax 3 months later showed resolution of consolidation and stable granulomatous disease, with calcified lymph nodes. MR scan of brain highlighted meningeal enhancement consistent with recent meningitis and left mucosal sinus enhancement, probably from recurrent sinusitis. High-resolution non-contrast CT scan of the paranasal sinuses, searching for signs of CSF leak, was inconclusive.
She improved to a level at which discharge was appropriate and we arranged outpatient otolaryngological follow-up. Before discharge, we sent a nasal discharge sample for beta-2 transferrin concentration.
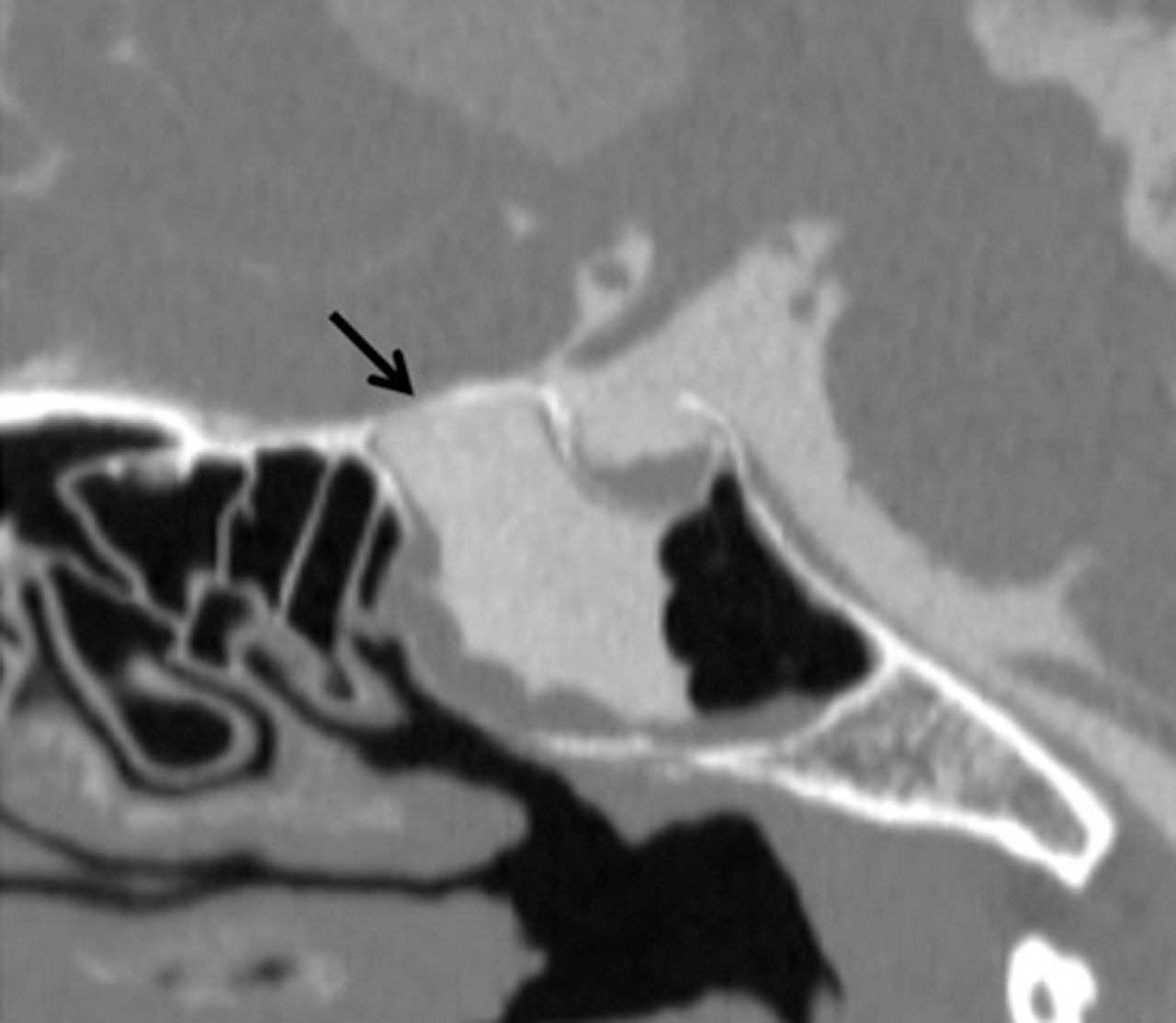
Unfortunately, she was readmitted 1 week later with pneumonitis. Her beta-2 transferrin in nasal discharge was elevated at 14.10 mg/L (negative <1.30 mg/L, possible 1.31–8.88 mg/L, positive >8.89 mg/L), strongly suggesting that it was CSF. This prompted further investigation for a CSF leak with intrathecal contrast-enhanced CT/MR cisternography, which identified a CSF fistula in the planum sphenoidale, the roof of the left sphenoid sinus (figures 1 and 2).

CSF rhinorrhoea. Sagittal CT cisternogram obtained after injection of 8 mL of intrathecal iohexol showing contrast leakage through a defect in the planum sphenoidale (arrow) with contrast extending from the cranial subarachnoid space and accumulating in the left sphenoid sinus.
CSF, cerebrospinal fluid.

{kind=link}
{kind=link}
CSF rhinorrhoea. Coronal T1-weighted MR cisternogram obtained after 0.2 mL of intrathecal gadobutrol injection (1.0 mmol/mL) showing contrast leakage (arrow) extending from the cranial subarachnoid space into the sphenoid from a defect in the left side of the planum sphenoidale—roof of the sphenoid sinus.
CSF, cerebrospinal fluid.
In the absence of prior trauma, we diagnosed spontaneous CSF rhinorrhoea. We gave pneumococcal vaccine and discharged her home on prophylactic amoxicillin until she could have definitive surgical management.
Spontaneous CSF rhinorrhoea is rare, poorly understood and variable. Obesity is a known risk factor. It is probably linked to the development of intracranial hypertension, with resulting bone remodelling and thinning.1 Coughing, sneezing and any other causes of fluctuating intracranial pressure may affect its progression.
In this case, the combination of raised body mass index and recurrent sinusitis with coughing and sneezing was probably important in forming the fistula, in turn leading to bacterial meningitis and aspiration pneumonitis.
This diagnosis requires a thorough investigation and a high index of suspicion. CT and MR cisternography are effective for evaluating and localising suspected CSF fistulae along the skull base and for guiding surgical repair.2
She underwent an urgent endoscopic CSF leak repair under the care of otolaryngology. Eight weeks postoperatively, she had mild fatigue and headache but was otherwise well, and has had no further rhinorrhoea or episodes of meningitis. At 6-month follow-up, she had recovered fully, had returned to regular exercise and is planning her return to work.
Footnotes
Contributors ÁM was the leading consultant treating the patient and reviewing the manuscript. GR gathered information of the patient and wrote the case report. NF provided neuroradiological guidance and investigation throughout her treatment along with a review of this aspect of the case report. RB provided microbiological guidance and advice on treatment cover along with a review of the article.
Funding None.
Competing interests None declared.
Patient consent for publication Obtained.
Data sharing statement Not applicable.
Provenance and peer review Not commissioned. Externally peer reviewed by Tyagi Alok, Glasgow, UK, and Paul Smith, Bristol, UK.
Other content recommended for you
- Just another case of bacterial meningitis… or… is it?
- Spontaneous cerebrospinal fluid rhinorrhoea as the presenting feature of an invasive macroprolactinoma
- Idiopathic sphenoid sinus CSF rhinorrhoea
- A clue in the nose
- Carolyn’s window approach for spontaneous frontal sinus meningoencephalocele
- Endoscopic and fluoroscopic-guided closure of the eustachian tube using a biliary cytology brush and liquid embolic agent for a persistent CSF leak after schwannoma resection
- Spontaneous cerebrospinal fluid rhinorrhoea: a rare clinical entity
- Oval window perilymph fistula in child with recurrent meningitis and unilateral hearing loss
- Endoscopic pedicled nasoseptal flap repair of spontaneous sphenoid sinus cerebrospinal fluid leaks
- Transnasal transpterygoid resection of meningoencephalocoele with abolition of seizures