Article Text

Abstract
Intracerebral haemorrhage (ICH) accounts for half of the disability-adjusted life years lost due to stroke worldwide. Care pathways for acute stroke result in the rapid identification of ICH, but its acute management can prove challenging because no individual treatment has been shown definitively to improve its outcome. Nonetheless, acute stroke unit care improves outcome after ICH, patients benefit from interventions to prevent complications, acute blood pressure lowering appears safe and might have a modest benefit, and implementing a bundle of high-quality acute care is associated with a greater chance of survival. In this article, we address the important questions that neurologists face in the diagnosis and acute management of ICH, and focus on the supporting evidence and practical delivery for the main acute interventions.
- Stroke
- clinical neurology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
INTRODUCTION
Spontaneous intracerebral haemorrhage (ICH) refers to non-traumatic bleeding in the brain parenchyma and is the deadliest form of stroke. The high 1-month case-fatality rate of ~40% and poor long-term outcome make it a major contributor to global morbidity and mortality.1 2 Although ICH accounts for a minority of stroke worldwide (10–30%), it is associated with a greater burden of disability-adjusted life years than ischaemic stroke, given its high incidence in low- and middle-income countries.3 Despite dramatic drops in ischaemic stroke mortality rates,3 there has been limited improvement in case fatality from ICH in the last few decades2 4 5 and most survivors are left with severe disability.2 6 7
ICH is not a single entity; 85% of cases are due to cerebral small vessel disease, predominantly deep perforator arteriopathy (also termed hypertensive arteriopathy or arteriosclerosis) and cerebral amyloid angiopathy, while the remainder results from a macrovascular (eg, arteriovenous malformation, cavernoma, aneurysm and venous thrombosis) or neoplastic cause. Vascular malformations are the most common cause of ICH in young adults, accounting for up to one-third of cases.8 The term ‘primary’ ICH is often applied to cases caused by cerebral small vessel disease, but it discourages adequate investigation and accurate classification and is not recommended. Deep haemorrhages account for about two-thirds of cases, occur in the internal capsule, basal ganglia or brainstem, and more likely result from deep perforator arteriopathy. About 5–10% of ICH occurs in the cerebellum. The remainder is lobar haemorrhage located in cortico-subcortical areas, often near or reaching the cerebral convexities, of which ~40% are due to arteriosclerosis alone, ~40% to arteriosclerosis and amyloid angiopathy and the remaining ~20% to amyloid angiopathy alone.9
There are no medical treatments for acute ICH that have been definitively proven in primary outcome analyses of randomised clinical trials. Patients with ICH are frequently referred for surgery, but the roles of various surgical methods and timing of surgery remain controversial. In this article, we outline a practical approach to the diagnosis and management of acute ICH.
ACUTE EVALUATION
Time is limited; what information do I need to obtain early on?
The approach to an efficient and focused history and physical examination in suspected acute stroke has been outlined in the first article in this series.10 It is important to obtain a history of any recent trauma, including from a witness if available, and to assess for any circumstantial evidence, making sure to determine clinically whether the trauma preceded the haemorrhage or vice versa. Acute ischaemic stroke and ICH cannot be reliably distinguished at the bedside but the diagnosis is made rapidly and easily on imaging, so every effort should be made to minimise delays to the initial CT brain scan. Crucial information specific to the management of ICH must be obtained as early as possible after the CT brain scan; table 1 lists the key questions to ask focused on modifiable predictors of outcome.
Important information to obtain as soon as possible after ICH to guide prognostication and management
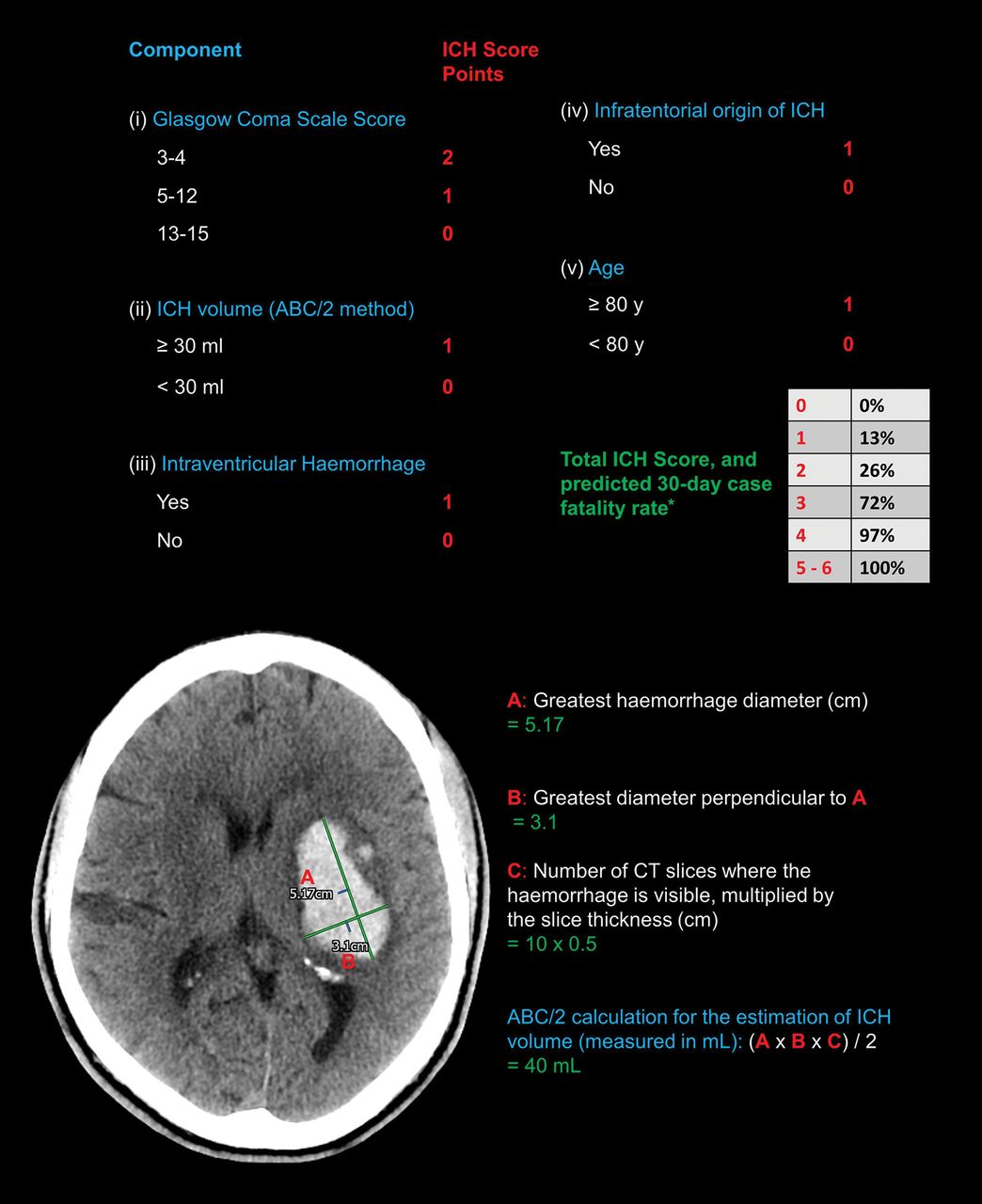
The National Institutes of Health Stroke Scale (NIHSS) used for ischaemic stroke is also valuable in ICH, but its utility may be limited by the more frequent occurrence of depressed consciousness in ICH.21 The Glasgow Coma Scale (GCS) score is the most useful initial evaluation because of its similar prognostic value to NIHSS, its simplicity and its incorporation in the ICH score (figure 1 outlines its calculation). However, as in ischaemic stroke, aphasia can reduce the verbal subdomain score, and thus cause underestimation of the GCS.

Upper panel: Calculation of the intracerebral haemorrhage score, a clinical grading scale and a useful communication tool. Predicted 30-day case-fatality rates are derived from the original validation study22; *a subsequent study in which early do-not-resuscitate orders were not placed observed 30% lower mortality rates.23 Lower panel: The use of the ABC/2 calculation (essentially the formula for the volume of an ellipsoid) to rapidly and accurately24 25 estimate the volume of an acute left-sided ganglio-capsular haemorrhage on non-contrast CT brain scan. (Copyright Iain McGurgan).
What baseline tests should I perform?
For all the complexity and uncertainty in ICH management, the initial diagnosis of acute blood in the brain substance is straightforward. Non-contrast brain CT (figure 2) is rapid, highly sensitive and specific for all forms of ICH, and widely available, so is considered the reference standard for ICH diagnosis.21 26 27

This axial non-contrast CT brain scan shows an acute large right parietal lobar haematoma, with moderately severe confluent low attenuation (leukoaraiosis) extending from the lateral ventricles into the subcortical white matter. (Copyright David Werring.)
The CT scan should be assessed for ICH location, brain changes consistent with small vessel disease (atrophy, leukoaraiosis (figure 2) and lacunes), the presence and degree of mass effect or midline shift, hydrocephalus, intraventricular extension and the size of the haematoma. Haematoma volume independently predicts haematoma expansion and early mortality11 28 and can be estimated rapidly and accurately on CT with the ABC/2 formula, as shown in figure 1. A blood-fluid level is highly specific for coagulopathy or the use of anticoagulants and should prompt a search for these factors if not already established.29 MR is as sensitive as CT in the hyperacute diagnosis of ICH26 30 but it rarely provides more information in the acute stage; the longer scan duration and delays obtaining MR for often critically ill patients make CT a preferred choice.
Blood tests including coagulation studies, glucose, cardiac-specific troponin and a toxicology screen should be performed. Point-of-care INR testing should be implemented to avoid delays in anticoagulation reversal for patients taking warfarin.31 ECG abnormalities are common, but concomitant myocardial injury should not be overlooked.32
Do I need to request further imaging?
Early diagnosis of macrovascular causes of ICH allows timely starting of specific treatment and refines the prognosis. The decision whether to pursue further imaging has often been made based on assumptions guided by patient risk factors, but these are not a reliable way to exclude a potential macrovascular cause in all cases, and clinical practice varies widely.33
CT angiography (CTA) should be performed acutely in all patients, preferably within 2 days of the non-contrast brain CT,34 except those definitely at low risk of having an underlying macrovascular cause (figure 3). Imaging predictors of haematoma expansion on CTA such as the ‘spot sign’ (foci of contrast extravasation within the haematoma) may also add prognostic value.11 35 If CTA is negative for structural vascular abnormalities, MR/MR angiography should be considered as soon as possible as it has additional diagnostic yield.34 Digital subtraction angiography is then warranted in patients at high risk of an underlying macrovascular cause after negative CTA (and negative MR, if performed).34 There is an appreciable yield of repeat digital subtraction angiography performed a few weeks later, especially in lobar ICH,36 so persistence is often required.

Algorithm with risk stratification to aid decision-making on further imaging, and the diagnostic yield of intra-arterial digital subtraction angiography in ICH. CTA, CT angiography; DSA, digital subtraction angiography; ICH, intracerebral haemorrhage. ¥Parameters for pre-test risk estimation are derived from scoring systems based on patient characteristics and non-contrast CT from the DIagnostic AngioGRAphy to find vascular Malformations (DIAGRAM) study, a prospective, multicentre study assessing the accuracy of multiple imaging modalities in the diagnosis of macrovascular causes of ICH.34 37 Individuals meeting the ‘low risk’ criteria above were excluded from the DIAGRAM study because of the low probability of finding an underlying macrovascular cause,38 and the yield of CTA in the remainder was 17%. Low rates of underlying macrovascular causes in this group were confirmed in a subsequent validation cohort.37 Primary intraventricular haemorrhage (ie, that with no discernible parenchymal component) has been added to the high-risk group, based on high detected rates of underlying macrovascular causes.39 ¶Acute CTA should be performed within 2 days of CT, where possible. The diagnostic algorithm of the yield of intra-arterial DSA based on the CTA and clinical characteristics has been adapted from Wilson et al. 40 MR/MR angiography performed acutely after a negative CTA may have additional value, particularly for the diagnosis of non-macrovascular causes, before considering intra-arterial DSA.34 *Confluent leukoaraiosis (see fig ure 2) or lacunar infarction on acute CT brain scan.
Beyond the acute phase, MR (including blood-sensitive sequences to detect cerebral microbleeds and cortical superficial siderosis) provides important additional information about the underlying cerebral small vessel disease.
Should I pursue intensive treatment?
The focus for the great majority of patients should be on the full provision of high-quality active treatment and supportive care, at least in the first 24–48 hours. Decisions about instituting a ceiling of care should depend on an assessment of prognosis, but this is difficult to determine acutely. There are multiple dedicated ICH prognostic grading scales, the most widely used being the ICH score,22 which has acceptable discrimination for functional outcome measured by the modified Rankin score at up to 12 months (figure 1). Such scales should not be used, however, as the sole means to gauge prognosis or guide the withdrawal of supportive treatment.21
Like other conditions with high rates of poor outcomes and a perceived lack of effective treatments, ICH is vulnerable to therapeutic nihilism. Early ceilings of care and a focus on comfort measures are more likely to be pursued acutely in ICH than in ischaemic stroke, independent of neurological deterioration and co-morbidities, and are associated with poorer outcome.41 While timely do-not-resuscitate orders are important considerations in stroke management, these should not influence other aspects of care. In practice, however, do-not-resuscitate orders in ICH often herald less active supportive care,42 43 so clinicians should be cautious when considering early do-not-resuscitate orders.
ACUTE MANAGEMENT
How do I approach the management of ICH?
ICH is a neurological emergency. The presence of expanding haematoma and vasogenic oedema inside the fixed volume of the cranial vault can lead to a precipitous increase in intracranial pressure (ICP) and fatal brain herniation syndromes. The principle of ‘time is brain’ also firmly applies to ICH; haematoma expansion occurs very early11 and independently predicts a poor outcome.18 The rapid delivery of a care bundle incorporating anticoagulation reversal, intensive blood pressure management and neurosurgery/critical care if required has been associated with a substantial improvement in 30-day case-fatality rates.44
The overarching goals of acute management are to stabilise the patient to ensure they survive the initial insult, and to prevent secondary brain injury (figure 4). Patients with ICH may require immediate intensive care unit admission. Otherwise, all patients should be admitted to an acute stroke unit as soon as possible; the benefit is at least as great for patients with ICH as it is for those with ischaemic stroke.45 The general principles of acute care are the same as those for acute ischaemic stroke, as outlined in the first article in this series.10 Secondary prevention measures, cerebral small vessel disease and decisions regarding restarting antithrombotic therapy will be addressed in subsequent articles.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Schema of the time course and mechanisms of secondary brain injury in intracerebral haemorrhage, including intraventricular haemorrhage.
Management of the complications of ICH is a key focus of acute care. Raised ICP can result from the mass effect of the bleed or peri-haematomal oedema or from hydrocephalus. Although there is a lack of evidence to guide its management in ICH, measures used for raised ICP in other settings may help. These include raising the head of the bed to 30° (although without supportive evidence in acute stroke46), mild sedation, analgesia and mannitol (or hypertonic saline, depending on cardiac and renal comorbidities).18 Intensive ICP monitoring is recommended in those with a GCS<9, evidence of herniation or hydrocephalus.21 Corticosteroids are possibly associated with more harm than benefit when used for lowering ICP in ICH, so should not be used.47 Early-onset seizures are not uncommon, occurring in one in seven patients, with most occurring at or near the onset.48 Clinical seizures should be managed with antiseizure medications, but prophylactic treatment should not be offered routinely.21 Cortical involvement, age younger than 65 years, volume greater than 10 mL and early seizures within 7 days of ICH identify patients at higher risk of subsequent late seizure development.49
If the patient takes anticoagulant treatment, how do I reverse it?
Anticoagulation-associated ICH accounts for nearly 20% of all cases.50 The haemorrhage in this setting is of larger volume,51 52 is more likely to exhibit haematoma expansion11 and is associated with higher morbidity and mortality53–55 compared with ICH not associated with anticoagulation. Stopping antithrombotic therapy and reversing anticoagulation immediately after the diagnosis of ICH is, therefore, crucial.56 Although ICH risk associated with the use of direct oral anticoagulants (DOACs) was around half that of warfarin in randomised trials,57 a previous lack of specific reversal agents for DOACs prompted concerns that DOAC-associated ICH may be associated with poorer outcomes. In fact, the prognosis of ICH associated with DOACs is likely better58 or at least no worse59 than that of warfarin, and the availability of approved specific reversal agents for DOACs has improved. Table 2 provides a guide to the reversal of anticoagulation.
Strategies and rationale for anticoagulation reversal in acute ICH
Poorer outcomes are also seen for ICH associated with antiplatelet therapy,70 but platelet transfusions increase rather than decrease morbidity and mortality in this group,71 and therefore should not be used.
Patients with ICH in the context of coagulation factor deficiencies or thrombocytopenia should undergo replacement, with input from a haematologist.21 Several trials have assessed the efficacy of coagulation factors more generally in the management of acute ICH but found that the risk of thromboembolic complications outweighed the benefits.72 A trial of early administration of factor VIIa in an identified subgroup of patients most likely to benefit, however, has been approved (FASTEST, NCT03496883). Antifibrinolytic drugs, on the other hand, have proven promising. A large trial of intravenous tranexamic acid (TICH-2) showed a significant reduction in haematoma growth and early mortality, but there was no overall benefit for the primary outcome of later functional recovery,73 and it is thus not recommended as part of current care. A further study focusing on effects on early mortality and targeting earlier treatment is planned, and an ongoing trial is evaluating tranexamic acid in hyperacute presentations of ICH including mobile units (STOP-MSU, NCT03385928). Randomised evidence on associations of tranexamic acid in anticoagulation-associated ICH is lacking, although a trial in DOAC-associated ICH is currently underway (TICH-NOAC, NCT02866838).
Do I need to lower the patient’s blood pressure, and if so, by how much?
Observational data suggest that blood pressure is very high in the acute phase after ICH, significantly higher than that after ischaemic stroke.14 High blood pressure in acute ICH is associated with haematoma expansion and poor clinical outcome.15 16 There have been concerns for many years that high blood pressure may be necessary to ensure adequate cerebral perfusion after ICH, and that aggressively treating it may cause harm. Such concerns have been assuaged by evidence that suggests that adequate cerebral blood flow is maintained after acute blood pressure reduction in ICH.74 75 However, results of the two largest trials of intensive blood pressure lowering early after ICH76 77 have renewed uncertainty. Meta-analyses of these trials and other smaller studies showed that early intensive blood pressure lowering was safe, but without functional or mortality benefit.78–82 In contrast, a linear association between systolic blood pressure achieved in the first 24 hours and functional status was found in a recent individual participant data meta-analysis of the two largest trials, with improvements in functional recovery seen for blood pressure as low as 120–130 mm Hg.83 These trials excluded patients with large and severe haematomas, however, so caution must be exercised when treating such patients, especially where large reductions in very hypertensive patients might predispose to harm.19 84 ⇓ Table 3 provides some practical advice for blood pressure management in acute ICH, based on existing guidelines.85 It should be noted that, in light of the uncertainty described above, future research might conclude that there is no benefit from acute intensive blood pressure lowering.
Which patients should I refer for neurosurgery?
The rationale for clot removal surgery is to reduce direct and secondary brain injury (figure 4). The location of ICH has a large bearing on decision-making. Neurosurgical intervention is generally recommended for infratentorial bleeding despite a lack of randomised evidence,88 given the high risk of brainstem compression and herniation syndromes in the confined space of the posterior fossa. Clinical guidelines recommend posterior fossa decompressive evacuation for cerebellar ICH>3 cm in diameter, or for smaller haematomas associated with brainstem compression or hydrocephalus from ventricular obstruction.21 This recommendation is based on observational evidence that haematoma evacuation is associated with decreased mortality, but there is no evidence for improvements in functional outcome.89 Management of hydrocephalus by external ventricular drainage alone is not recommended in this setting and may be harmful, especially if the basal cisterns are compressed.90 The lack of clinical equipoise probably precludes the design of any future randomised trials to address the question of surgical vs conservative management.
Equipoise exists in bounds, however, where supratentorial haemorrhage is concerned. Seventeen randomised controlled trials have addressed surgical evacuation of supratentorial ICH, with all of the larger trials and meta-analyses returning neutral results on the primary outcomes.91 As a result, best medical management is usually pursued, but trials were complicated by high crossover rates, and there appear to be subgroups of patients who might benefit from surgical intervention. Patients with a GCS at presentation of 10–13, that is, not at either extreme of arousal, those with large ICH and those with superficial bleeds may experience improved outcomes.92–94
Multiple surgical techniques have been investigated for different indications; table 4 provides a summary of the evidence for each. Developments in minimally invasive surgery for patients with supratentorial ICH are promising. The only large trial of catheter evacuation followed by irrigation with alteplase (MISTIE III95) found no clear benefit but noted that the procedure was safe. There was, however, evidence of functional improvement in patients meeting the surgical goal of reducing haematoma size to <15 mL.96 The ongoing ENRICH trial (NCT02880878) is investigating a novel minimally invasive technique involving a small-directed craniotomy and image-guided trans-sulcal evacuation97 and is one of several currently enrolling trials, some with an earlier time window for surgery (Dutch ICH Surgery Trial, NCT03608423; MIND, NCT03342664; INVEST, NCT02654015).
Summary of the evidence for different neurosurgical techniques in ICH
Optimal timing of surgical intervention remains controversial due to the risk of re-bleeding, although reducing haematoma volume early may reduce secondary brain injury and could improve outcome.91 100
FUTURE DIRECTIONS
The management of ICH has not paralleled the dramatic advances in acute ischaemic stroke therapeutics driven by many large randomised controlled trials. Clinical trials in ICH face unique challenges; a less common and more severe on average condition with poorly understood pathophysiology results in a sizeable proportion of patients being ineligible.106 Aspiring to recruit every ICH survivor to at least one trial is the only way to resolve uncertainties and improve outcome. Fortunately, we have much about which to be optimistic. There are currently over 60 active recruiting (or soon-to-be recruiting) ICH trials, many focused on the possible interventions of haemostatic agents and surgical techniques, where much uncertainty persists.
CONCLUSION
ICH has the worst outcomes of all stroke subtypes, but increased research interest in recent years has led to significant advances in its diagnosis and management. The focus of existing treatment is the prevention of haematoma expansion, and progress in supportive care, blood pressure control and anticoagulation reversal has been rewarded with improved outcome. The role of neurosurgery is still unclear but the field is rapidly evolving, with minimally invasive techniques showing promise in selected groups, even in the context of neutral trials so far.
Key points
Intracerebral haemorrhage is a medical emergency; its rapid diagnosis, investigation and treatment should prevent further brain injury and improve outcome.
Although 30-day case fatality is ~40%, full supportive care should be considered for at least the first 24–48 hours, as prognostication can be difficult.
Hyper-acute interventions such as anticoagulation reversal, blood pressure lowering and neurosurgery may improve recovery, but many uncertainties remain.
Clinical trials based on pathophysiological knowledge and embedded in routine clinical practice are the main hope for its better management.
FURTHER READING
Cordonnier C, Demchuk A, Ziai W, Anderson CS. Intracerebral haemorrhage: current approaches to acute management. Lancet. 2018;392(10 154):1257–1268.
Balami JS, Buchan AM. Complications of intracerebral haemorrhage. The Lancet Neurology. 2012;11(1):101–18.
REFERENCES
Footnotes
Correction notice This article has been corrected since it appeared Online First. Text has been corrected from thrombocytopaenia to thrombocytopenia
Contributors IJMG drafted the manuscript. The other authors revised the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned. Externally peer-reviewed by Anthony Pereira, London, UK.
Linked Articles
- Editors’ commentary
Other content recommended for you
- Current management of spontaneous intracerebral haemorrhage
- Effects of blood pressure and tranexamic acid in spontaneous intracerebral haemorrhage: a secondary analysis of a large randomised controlled trial
- Sporadic cerebral amyloid angiopathy revisited: recent insights into pathophysiology and clinical spectrum
- Chinese Stroke Association guidelines for clinical management of cerebrovascular disorders: executive summary and 2019 update of clinical management of intracerebral haemorrhage
- Medical management of intracerebral haemorrhage
- Symptomatic lobar intracerebral haemorrhage preceded by transient focal neurological episodes
- Enlarged perivascular spaces as a marker of underlying arteriopathy in intracerebral haemorrhage: a multicentre MRI cohort study
- Prominent juxtacortical white matter lesion hallmarks NOTCH3-related intracerebral haemorrhage
- Validation of the ICH score in patients with spontaneous intracerebral haemorrhage admitted to the intensive care unit in Southern Spain
- Tranexamic acid for acute intracerebral haemorrhage growth based on imaging assessment (TRAIGE): a multicentre, randomised, placebo-controlled trial