Article Text

Abstract
It is increasingly common for secondary care to provide advice to primary care without an outpatient appointment. Even before the increased telemedicine during COVID-19, many hospital services gave advice alone for some referrals, yet there are few published data about patient outcomes. Does advice and guidance alter outpatient numbers or simply mean that patients are seen later? Which neurological conditions can we manage at a distance? Do complaints increase from either primary care or patients? Do clinics become more complex and time consuming? Our department has developed an advice and guidance service embedded within the English electronic referral system since 2017, allowing detailed analysis of the outcome of 6500 patients over 2.5 years. We suggest ways to set up and run a neurology advice and guidance service, looking at the potential benefits and the barriers.
- clinical neurology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Electronic consultations (e-consults, known within the UK as ‘advice and guidance’) let clinicians communicate within a secure, electronic healthcare platform. Its use is rapidly increasing world-wide with the wish to improve primary care access to specialty care, reduce direct healthcare costs and reduce waiting times for face-to-face visits by reducing the pool of patients who require them.
Since 2018, the electronic referral system (e-RS) has been the obligatory electronic pathway within England for all primary care referrals into a hospital consultant-led service. An advice-only option was in the system for many years, but not widely used until 2019. Use of advice and guidance grew rapidly in 2020 when the COVID-19 pandemic closed many routine referral pathways.1 2
The Association of British Neurologists (ABN) recently produced guidelines for referral management including advice and guidance services within neurology.1 They emphasised the need for audit, liaison with information technology services, job planning the activity and making this one part of patient care, rather than simply a way to reduce long waiting lists. Clinicians have adapted to telephone and video consultations during 2020 to a greater or lesser degree. However, managing patients by providing electronic advice and guidance still represents a big shift in traditional models of secondary care, particularly given the value that most neurologists place on a detailed face-to-face history and neurological examination.
The ABN report detailed earlier reports of advice and guidance in various UK neurology departments,3–7 including advice by email, telephone, dictated letters or a shared electronic record. Only small numbers of cases have been included in published series, with few outcomes measured in the UK or elsewhere. The largest single reported dataset was 1675 in Northern Ireland (Forbes and Campbell, unpublished data). There have been no reports of outcomes of advice and guidance use within the current national e-RS used by National Health Service England. The largest systematic review of North American e-consults to date highlighted a lack of high-quality evidence but suggested that patient satisfaction was high, outcomes were largely positive, there was no increase in adverse events but that specialists remained ambivalent and had some concerns about workload.8
Box 1 details our experience in developing our advice and guidance.
The Newcastle advice and guidance service—development and lessons learnt
The Newcastle Regional Neurosciences service has 15 whole-time equivalent consultants serving a population of 1.3 million. We see 27 000 neurology new and review outpatients annually. This includes the expected mix of routine general neurology outpatient clinics, sub-specialist clinics and emergency clinics.
In 2013, an audit of 116 patients waiting longer than 18 weeks showed that only 24% required a face-to-face appointment, having first received written advice. A further audit in 2015 showed highly variable triage among consultants: some wrote with advice and guidance for >30% of referrals while some accepted all referrals. Of those patients given advice and guidance, only 21% subsequently required review within the department within the next 12 months.
In 2017, we moved to department-wide advice and guidance, which has evolved into a referral management system using the national electronic referral system (e-RS), with a dedicated group of five consultants who are job planned to answer advice and guidance for 2 hours per week. Primary care can choose advice and guidance immediately or send in a referral for triage. This is then allocated to advice only or to an appointment. General practitioners (GPs) can no longer book directly into a neurology clinic slot.
We agreed that exclusions for advice and guidance were to be: urgent referrals, patients already under a consultant neurologist’s care, patients with a movement disorder or any patient with an abnormal examination. We encouraged referrals for headache management, sensory disturbance with normal examination and if the GP was checking whether neurology was the appropriate service for the problem (see figure 1 for the GP view within e-RS).
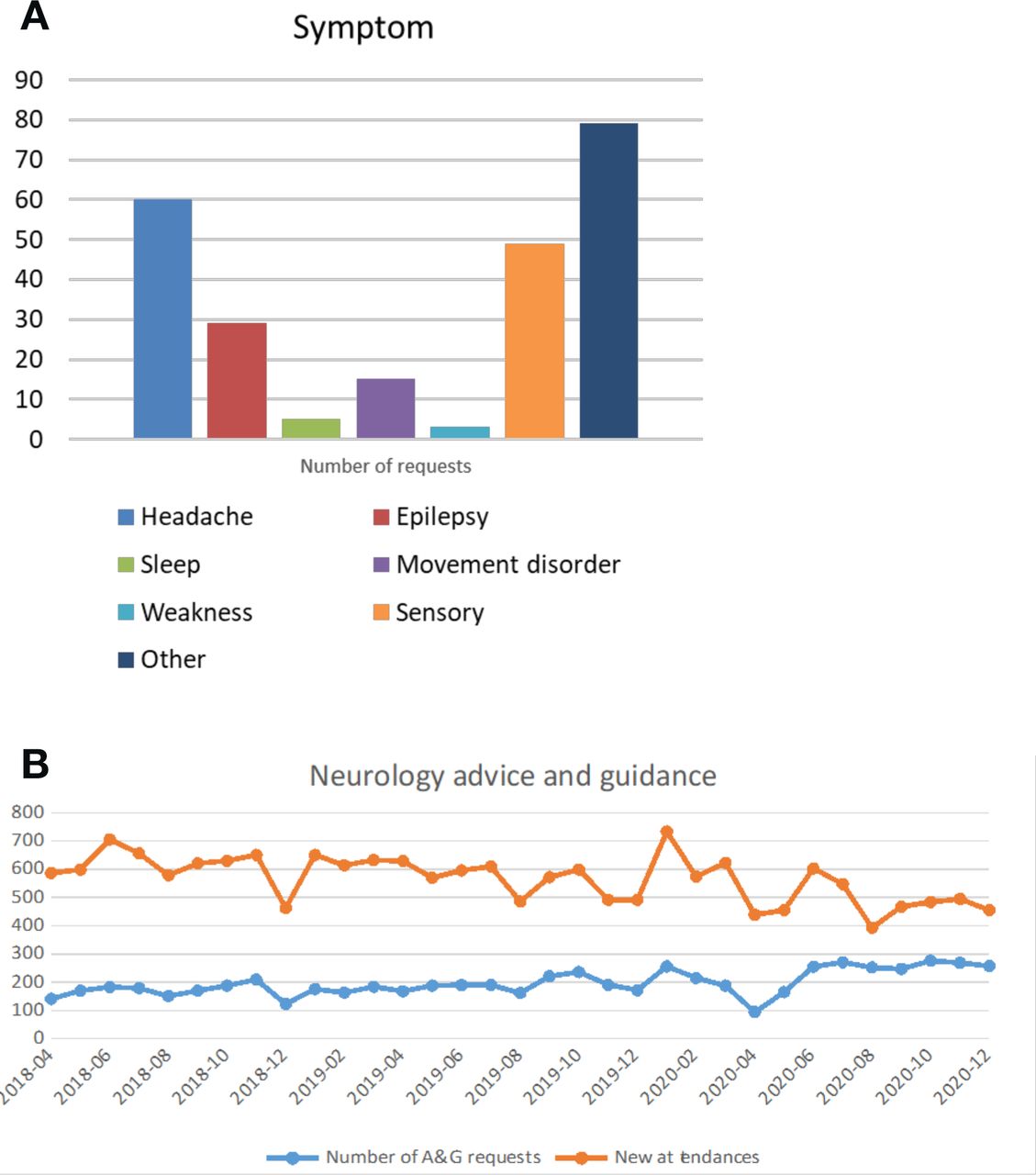
Headache, sensory symptoms were the most common conditions (figure 2A). Advice regarding management was 72% of requests, 19.5% asked about investigations such as blood tests or the need for imaging, only 11% asked about diagnosis. We answered requests within a mean response time of 0.5 days, excluding weekends and bank holidays. Figure 2B shows the monthly data from the advice and guidance service referrals and outpatient attendances; currently advice and guidance accounts for 35% of all new patient activity coming in to e-RS; 7% of these requests were converted by the triaging neurologist to a face-to-face appointment.
Advice and guidance has not significantly changed the total number of outpatient attendances, which have remained stable over the last 5 years. However, a significant number of additional patients have benefited from remote neurological advice.
Did complaints increase?
This was a key concern raised by colleagues before moving to a referral management system. Complaints against health professionals can be very time consuming and cited as a source of distress and burnout for physicians. There were 75 complaints over the 3 years (January 2017–December 2020) regarding the neurology service. Only four related to advice and guidance given rather than to a face-to-face consultation. None had formal complaints instigated by the GP, and none proceeded beyond a written response from the hospital.
Primary care engagement and education. We developed the service in close liaison with primary educational leads and support from the clinical commissioning groups. This led to our developing concise, single-page guidelines for all common neurology problems (examples included in online supplemental file l). These could then be attached with advice responses. The feedback is qualitative but can be summarised as: the educational part was very helpful; anything over a page is too long; we should not expect GPs to do complicated examinations with which they are unfamiliar (such as head-impulse test); if we ask a second time or if the patient is unhappy—please see them (which we do).
Supplemental material

The GP view within the electronic referral system (e–RS) of our inclusion and exclusion list. GP, general practitioner.
{kind=link}
{kind=link}
(A) Requests received during June 2018. A total of 214 sequential advice and guidance requests received with the symptoms described. (B) The total number of advice and guidance requests (darker lower line) and new patient attendances within Newcastle service (upper line) from April 2018 to December 2020. Number of patients are shown per month.
General principles for advice and guidance for neurology services
Liaise with primary care: Neurologists should liaise with the referring physicians in primary care (in England this is general practitioner (GP) Clinical Commissioning Group leads) before starting the service, and regularly thereafter.
Use opportunities for primary care education: There is an opportunity to increase GP education about common neurological complaints and specific elements of neurological examination (such as a Dix-Hallpike manoeuvre). Meeting with primary care colleagues can help to manage expectations.
Agree on appropriate patients: It is important to agree which patients are likely, or not likely, to benefit from advice and guidance. Patients with symptoms but no signs are most likely to benefit; those with movement disorders, gait disorders or weakness are far harder to manage with advice alone (see figure 1).
Understand what investigations are available: Ensure that GPs have access to investigations before you ask that they request them. This may require negotiation with other services such as radiology to provide access if appropriate alongside advice and guidance.
Ensure guidelines are accessible: Any guidelines used within advice and guidance responses should align with national primary care guidelines, such as those of the National Institute for Health and Care Excellence, but can also signpost to relevant local services. These should be in a site accessible to referring doctors. Such guidelines should be updated annually. An example of one of our guidelines (Bell’s palsy) is within online supplemental files.
Keep a list of Frequently Asked Questions: There are several very common primary care enquiries and so it helps to develop a list and agreeing answers beforehand. Regular contact with the GP educational leads is important to keep these up to date.
Understand what advice and guidance is available from other specialties: Be aware of other advice and guidance services within secondary care specialities. Ensure there is a consistent approach between services.
What will you be asked about?
Headache management is likely to be the most common request.5 7 Most commonly this relates to diagnosis and management advice relating to migraine. This varies from a GP wanting reassurance with the diagnosis of ocular migraine in an older patient, to advice about what is the third drug to try after amitriptyline has caused sedation and topiramate led to grumpiness. We might personalise advice on migraine management—including lifestyle, stopping daily painkillers, and which additional prophylactic agents to consider—and often attach our regionally agreed headache management flowchart to the response. We may also signpost to good patient self-help websites, for example, The Migraine Trust for migraine, or OuCH UK for cluster headache. Other queries include concerns regarding less common headaches such as possible trigeminal neuralgia.
Sensory symptoms often lead to queries, many relating to otherwise well patients with flitting, crawling feelings across the scalp and face; typically the GP is not anxious but the patient is. Among such requests will be recognisable syndromes, such as carpal tunnel syndrome, restless legs, meralgia paraesthetica and more rarely tarsal tunnel syndromes and notalgia paraesthetica.
Miscellaneous symptoms. There are many ‘other’ symptoms, for example, olfactory hallucinations are surprisingly high up in the list, even before COVID-19, and symptoms described in various ways that were likely either to be anxiety or adverse effects of polypharmacy with sedation and dizziness. Generally deprescribing is often recommended.
Where should this patient be referred? Is this the right clinic to refer to and is it urgent?
Does the patient need investigating? Does this patient simply need a scan, or do they need to see a neurologist first?
What do investigation results mean? Finding the ubiquitous ‘little white dots’ on MR scan of brain when a GP has arranged a scan to reassure the patient, but is then uncomfortable with a surprising but usually incidental finding.
Some movement disorders including benign eyelid myokymia and restless legs can often be recognised from history alone.
Inappropriate referrals. Despite clear requests to avoid using advice and guidance for patients who are acutely unwell, or need urgent review, inevitably on occasion these are referred. There needs to be an agreed timescale to answer responses to ensure appropriate requests are made.
What do neurologists get out of this?
This is about getting it right first time, providing rapid advice for patients with a neurological problem and directly from a neurologist. GPs really appreciate the rapid messaging and educational element, as otherwise they would have only access to the ever busy, on-call specialty trainee at best.
This approach is not something that suits all consultants. Those who triage should ideally choose to do so and be given time within job plans to do it. Developing a group of those triaging with different subspeciality interests and discussing cases will improve the service and provide peer support.
Neurologists traditionally have seemed remote from primary care. Well designed, interactive, quick advice and guidance makes us less so.
Key points
First talk to key stakeholders in primary care.
Understand the referral patterns in your service before starting advice and guidance, so that you can assess outcomes and assess its benefit later.
Recognise the time this takes for neurologists and include the work in their job planning.
Choose consultant colleagues who already do this in their practice.
It is essential to liase with information services, to help design the front page for your service, and to manage and update the information given out.
Further reading
Association of British Neurologists (ABN) Guidance on Neurology Active Referral Management (aka Advice and Guidance). ABN Executive and ABN Service Committee 2019–20. www.theabn.org/page/abnguidelines
National Health Service (NHS) Digital. Advice and guidance toolkit for the NHS e-referral service. Accessed 10/05/2021 https://digital.nhs.uk/services/e-referral-service/document-library/advice-and-guidance-toolkit
Ethics statements
Patient consent for publication
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors KNA conceived and wrote the manuscript, analysed complaints data. NW collected audit data, commented on manuscript. JM collected data and commented on manuscript. MD commented on manuscript. PM analysed data within e-RS.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned. Externally peer reviewed by Jon Sussman, Manchester, UK and Geraint Fuller, Gloucester, UK.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
Linked Articles
- Editors’ commentary
- Editorial
Other content recommended for you
- A neurological letter from UK general practice
- Incidence of common compressive neuropathies in primary care
- Implementing online consultations in primary care: a mixed-method evaluation extending normalisation process theory through service co-production
- Prospective analysis of the accuracy of diagnosis of carpal tunnel syndrome using a web-based questionnaire
- Use and usability of GP online services: a mixed-methods sequential study, before and during the COVID-19 pandemic, based on qualitative interviews, analysis of routine eConsult usage and feedback data, and assessment of GP websites in Devon and Cornwall, England
- Patients’ use and experiences with e-consultation and other digital health services with their general practitioner in Norway: results from an online survey
- Use of a primary care online consultation system, by whom, when and why: evaluation of a pilot observational study in 36 general practices in South West England
- The neurology of pregnancy
- UK consensus on pregnancy in multiple sclerosis: ‘Association of British Neurologists’ guidelines
- Restless legs syndrome