Article Text

Abstract
Idiopathic intracranial hypertension (IIH) is more common in women of reproductive age who have obesity, yet there is little information on its management specifically in pregnancy. Women with IIH should plan their pregnancy including discussing contraception before pregnancy, recognising that hormonal contraceptives are not contraindicated. Potentially teratogenic medications including acetazolamide and topiramate are not recommended during pregnancy or in those with immediate plans to conceive; prescribing acetazolamide in pregnancy must only follow discussion with the patient and their obstetrician. Ideally, patients should aim to achieve disease remission or control before pregnancy, through optimising their weight. Although weight gain is expected in pregnancy, excessive weight gain may exacerbate IIH and increase maternal and fetal complications; evidence-based recommendations for non-IIH pregnancies may help in guiding optimal gestational weight gain. The vast majority of women with IIH can have a normal vaginal delivery, with spinal or epidural anaesthesia if needed, provided the papilloedema is stable or the IIH is in remission.
- BENIGN INTRACRAN HYP
- OBSTETRICS
- METABOLIC DISEASE
- NEUROOPHTHALMOLOGY
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Introduction
Idiopathic intracranial hypertension (IIH) is characterised by raised intracranial pressure that frequently causes chronic headaches and visual loss. It predominately affects women of reproductive age with obesity.1 Its exact pathophysiological mechanisms are not yet fully established.2 IIH is associated with central adiposity3 and recent weight gain4 and IIH adipocytes appear transcriptionally and metabolically primed towards lipogenesis and adipose accumulation.5 Other features of metabolic dysregulation in IIH include a doubled risk of cardiovascular disease,6 androgen excess,7 and insulin resistance.5 The document ‘IIH: the international consensus guideline’ is a useful source of information for its management.8
Reproductive health in patients with IIH can be complex and there is currently limited guidance to support clinical care. We aim to provide practical guidance for managing women with IIH when approaching and during pregnancy. We discuss its medical and surgical management in relation to pregnancy and suggest limits on gestational weight gain.
Prepregnancy
Contraception
Hormonal contraceptives are not contraindicated in IIH8 and there is no preferred contraceptive method. Previously, case reports have linked oral contraceptives to secondary causes of raised intracranial pressure (pseudotumour cerebri); however, more recent literature has shown that they are not associated with increased incidence of raised intracranial pressure.9–11 We have noted that weight gain can be associated with starting oral contraceptives, and this may be something to explore sensitively with patients. Advice to withhold contraception may put women at risk of unplanned pregnancy. Where there is a clear temporal relationship between a patient starting the contraceptive and developing raised intracranial pressure, our pragmatic approach is to withdraw the contraceptive initially (with discussion about alternative methods) and to investigate for secondary causes, that is, coagulopathies.12 If the intracranial hypertension does not remit and no secondary cause is identified, then it is unlikely to be driven by the contraceptive, and so we would restart the medication with monitoring.8
Medical management
When a woman with IIH wishes to conceive, the aim is to achieve disease remission or stable disease with mild papilloedema. The International IIH Guideline details this management and follow-up dependent on papilloedema severity and visual function.8 We recommend using optical coherence tomography (OCT) imaging to monitor papilloedema and to track disease activity.13 The increased monitoring needed in pregnancy is discussed later.
Medication
Women of childbearing age need to have a careful risk–benefit discussion about medications that may be teratogenic. Several medications are used off label in IIH aiming to reduce intracranial pressure.
Acetazolamide, a carbonic anhydrase inhibitor, is the most commonly used medication in IIH. It can modestly improve visual function in IIH patients who have mild visual loss14, and improve quality of life.15 However, there is a high (48%) likelihood of discontinuation due to adverse effects when using a mean daily dose of 1.5 g.16 Animal studies have shown teratogenicity and so in the UK it is not recommend for those planning a pregnancy or during pregnancy.8 However, opinion internationally varies8 17 and a retrospective series of 50 pregnancies found no increase in adverse events.18 Women should be counselled that acetazolamide is potentially teratogenic (table 1) and its prescription in pregnancy must only follow discussion with the patient and their obstetrician.
Main adverse effects and teratogenic risks of acetazolamide and topiramate
Topiramate is used off label in IIH supported by in vivo19 and open-label study evidence.20 It is also effective in migraine prevention19 and sometimes can drive weight loss through appetite suppression.8 Human pregnancy registry studies have highlighted its teratogenicity21 (table 1) and so topiramate should be avoided in women actively planning to conceive. It is also important to counsel patients that at higher doses (>200 mg/day) it can reduce the efficacy of the combined contraceptive pill.22 23
Folic acid supplementation ≥400 μg daily is recommended for all women wishing to become pregnant, starting at least 1–3 months before conception and continuing during the first trimester. In line with the International Federation of Gynaecology and Obstetrics guidelines we recommend considering a higher dose (5 mg) for women with IIH and obesity, as obesity in pregnancy is a risk factor for fetal neural tube defects.24
Weight management
Body weight is a potentially modifiable risk factor in IIH; thus, women ideally should achieve a healthy body weight before conception.25 The WHO defines obesity as a body mass index (BMI) ≥30 kg/m2; however, in ethnic minorities this is lower at 27.5 kg/m2 due to their associated higher risks.26–28 Increased weight is a stigmatised area of healthcare and clinicians should broach this topic sensitively and with the patient’s permission. Local weight management services can offer practical support for first-line interventions8 with diet, physical activity and behaviour change. The target for initial weight loss in women with obesity planning a pregnancy is typically 5%–10% of preconception weight;29 a normal BMI (18.5 to 24.9 kg/m2) target,24 29 although ideal, may not be realistic. Bariatric surgery can achieve lower and sustained reductions in intracranial pressure and put IIH into remission but is not appropriate for all.30 Following bariatric surgery, guidance suggests women wait at least 18 months before conceiving to enable optimisation of weight management and management of nutritional deficiencies.31 Dietary supplementation may be required, and we recommend consulting with a physician or dietician with expertise in the management of bariatric surgery patients for those planning conception or are newly pregnant.
During pregnancy
Medical management
Most pregnant women with IIH come under obstetric consultant care. Patients with existing stable IIH typically do very well during pregnancy; those newly diagnosed with IIH while pregnant can be more challenging as their disease may be more aggressive.
During pregnancy, we aim to review patients who are in ocular remission every trimester, for the reassurance of both the patient and healthcare professionals involved in their care. This allows information to be passed to the obstetric team regarding safe delivery methods. For those not in ocular remission, the frequency of visits depends on their papilloedema and field status and is based on clinical judgement and experience. In the vast majority we review as frequently as every 6–8 weeks; however, some visits maybe done to evaluate visual assessment alone, with remote virtual review by the consultant with OCT imaging and visual fields.
Medication
Patients ideally should stop potentially teratogenic drugs (eg, acetazolamide, topiramate) before pregnancy, in order to avoid their use during the critical stages of embryogenesis in the first trimester. Pregnancies detected after the first trimester, may not benefit from rapid withdrawal and therefore should be based on IIH disease control. We recommend having individual patient discussions where there is ongoing actively raised ICP and if a patient is unable or unwilling to delay pregnancy. We understand that there are multifactorial reasons behind this decision and as clinicians our role is to enable an informed choice (table 1). We cannot, however, recommend their routine use in pregnancy. Teratogenicity in humans has not been reported for acetazolamide unlike topiramate, however, this is based on a small case series of 50 patients and not by large data, therefore, this should be factored into a risk–benefit assessment. From our experience, where use of these medications would be indicated during pregnancy, our patients can be managed by alternative methods outlined later in this article.
Headache management during pregnancy is important. When there is a new or changed headache in pregnancy, it is essential to identify red flag symptoms or signs32 33 and to investigate accordingly. The headache phenotype in IIH is typically migraine-like34 35 and, therefore, its management during pregnancy is based on migraine management. Clinicians should weigh the risks and benefits of headache medication taken during pregnancy. Table 2 summarises appropriate treatments, based on published reviews and guidance.33 36 Unrestricted acute treatment of headache symptoms increases the risk of medication overuse headache in IIH during pregnancy; this should be discussed and managed appropriately.
Acute headache recommendations in pregnancy
Weight management
Weight management is a key issue in IIH. Weight loss is disease-modifying and can put IIH into remission30 37 whereas weight gain can exacerbate it.38 39 Pregnancy leads to weight gain and consequently risks exacerbating IIH. Excessive weight gain during pregnancy also increases the risk of complications for baby and mother.40–42 Providing advice to pregnant women with IIH on how to approach weight gain in pregnancy is essential.
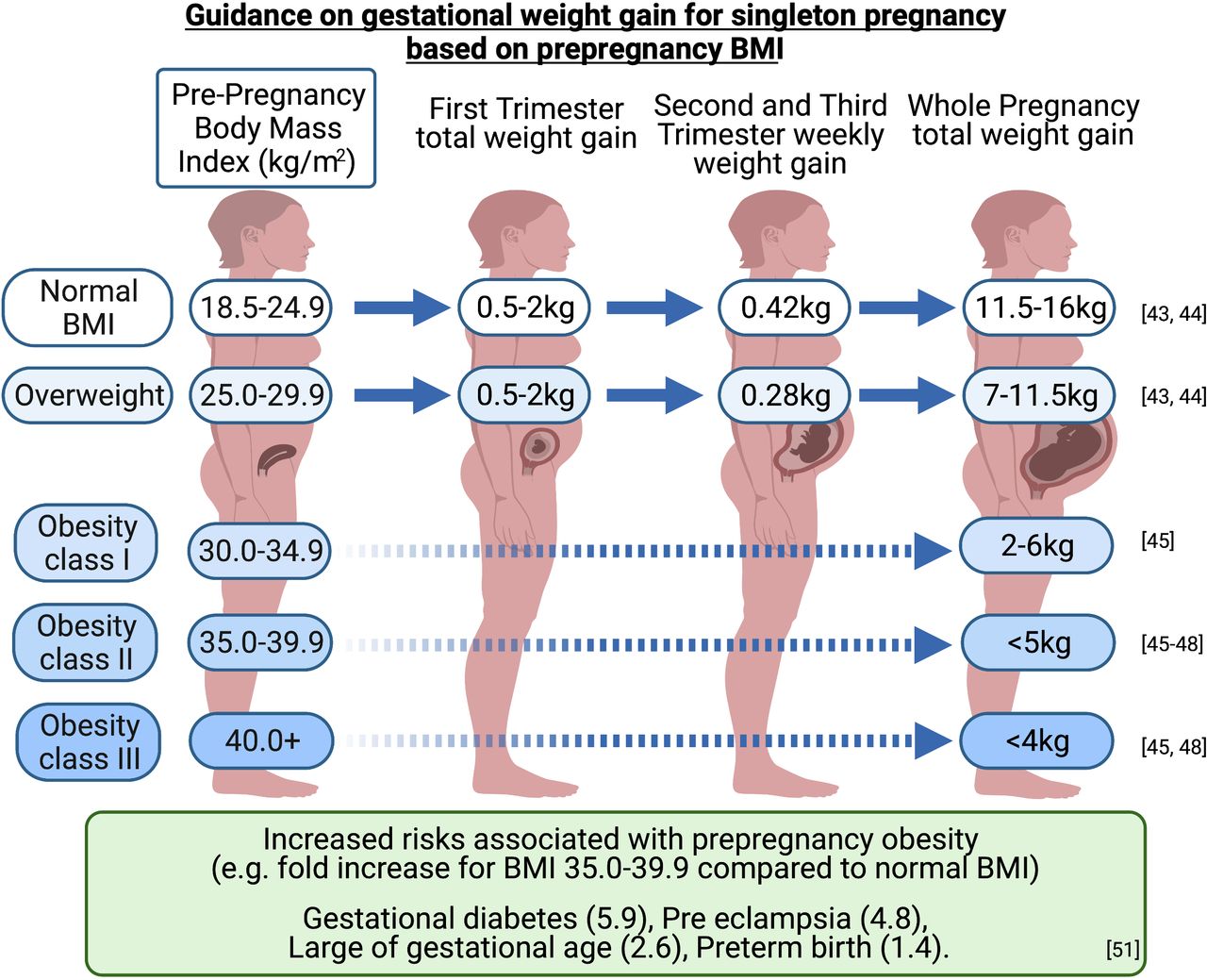
There are currently no evidence-based guidelines for limiting weight gain in pregnancy for women with IIH. The US Institute of Medicine (IoM) guidelines (2009) are used internationally to guide weight gain in pregnancy for women with a BMI ≤30 kg/m2.24 43 44 Those with a BMI ≥30 kg/m2 are recommended to gain less weight during pregnancy than patients with lower BMIs. The IoM suggests a gain of 5–9 kg during a singleton pregnancy in women with obesity, however, does not differentiate by obesity class.43 44 Subsequent studies suggest (figure 1) that those with a preconception BMI of:
30.0–34.9 kg/m2 should aim to gain 2–6 kg45.
35.0–39.9 kg/m2 should aim to gain less than 5 kg.45–48
>40 kg/m2 should aim to gain less than 4 kg.45 48

{kind=link}
Weight gain in pregnancy guide. Pregnancy complications/risks are higher with higher BMIs. Figures for obesity class II (BMI 35.0–39.9 kg/m2) are provided as a guide. Infographic created with BioRender.com. BMI, body mass index.
These targets must balance the risks of having large-for-gestational-age infants, small-for-gestational-age babies, preterm births and postpartum weight retention.44 49–51
The foundations of weight management during pregnancy are diet, physical activity and behavioural interventions. Weight loss programmes are not recommended during pregnancy, as the inadequate nutrition may harm the unborn child’s health.29 While some neurologists may not feel confident to provide general nutrition advice during pregnancy, all clinicians can dispel myths around ‘eating for two’. Women have no increased energy needs in the first and second trimesters, and only a slight increase in the third trimester—even then, it is only around 200 calories per day.29 52 Women may need advice about the benefits of physical activity for managing gestational weight gain, and its other health benefits during pregnancy. Pregnant women should be supported to reduce sedentary time and incorporate 150 min per week of moderately intense physical activity into their daily life,53 for example, walking or swimming. However, it is important to consider a woman’s baseline level of physical activity and build this up gradually according to capabilities.
We recommend an individualised approach so as not to obscure important biocultural factors, including socioeconomic status, ethnicity and comorbidities.54–56 We recommend referral to a dietitian (if resources permit) or an appropriately trained health professional to provide personalised advice on healthy eating and physical activity during pregnancy.29 This may be a referral initiated by the IIH clinic or liaising with maternity services or the general practitioner/family physician.
Many factors may influence management decisions, including IIH disease activity, risk of deterioration and prepregnancy BMI. A combined approach of diet, physical activity and behaviour change approaches has good evidence to reduce gestational weight gain.57 This is important as excessive gestational weight gain is also associated with increased postpartum weight retention. This can significantly increase the long-term weight gain trajectory of a woman of childbearing age,58 particularly if she has multiple pregnancies,59 and therefore, potentially increases the risk of IIH deterioration or recurrence.
Serial lumbar punctures
These are not usually recommended for management of IIH,8 but our experience suggests that in pregnancy they can sometimes provide short-term treatment.60 61 It is useful to note that in a commonly cited pregnancy publication, single lumbar punctures (LPs) were only needed in 25% (3/12).60 From our experience, although serial LPs or a lumbar drain may be required in severe papilloedema, these can often be avoided in those with mild papilloedema and stable visual function. Hence, we would not recommend routinely using serial LPs in pregnancy. If it is done, an LP in pregnancy could be performed with a Quincke (cutting) needle, which is more likely to lead to a cerebrospinal fluid (CSF) leak than an atraumatic needle. The patient should be counselled regarding exacerbation of headache.62 63 The volume drained is not as important as the type of needle as CSF will be replaced within a few hours.64–66 We would aim to normalise the CSF pressure (approx. 18 cmH2O) or by half if the opening pressure >40 cmH2O. We use OCT imaging to guide the impact of this intervention on papilloedema 24–48 hours later, however, this is based on clinical judgement.13 If the papilloedema is reduced or stabilised, we continue to monitor using OCT depending on papilloedema severity.
If the papilloedema increases and again poses a risk of rapidly declining vision, we would repeat the lumbar puncture. Our experience is that this type of bridging is most useful in the first trimester, since thereafter things often naturally start to improve. The timing of this intervention is judged primarily on the severity of the papilloedema, aided by OCT measures, including retinal nerve fibre layer (RNFL) thickness and optic nerve head volume; and on the impact of the visual function as measured by formal visual fields.67 Active IIH in the context of pregnancy should have specialist oversight, either a neuro-ophthalmologist or neurologist who regularly manages IIH. We would proceed to a more permanent surgical intervention only if the severity of the disease dictates it or if repeated lumbar punctures, or indeed a lumbar drain, could not hold the disease.
Surgical management
If a pregnant woman requires sight saving surgery, there are several options, as with women who are not pregnant. In reality, it is the local expertise and multidisciplinary team preferences that typically dictate which procedure is performed.
Ventriculoperitoneal shunting has been recommended by consensus as the optimal surgical procedure for CSF diversion as it has the most evidence of efficacy in IIH.8 68 However, there is an increased risk of ventriculoperitoneal shunt failure due to the increased intra-abdominal pressure in late pregnancy.69 For that reason, some surgeons prefer to use lumbar peritoneal shunts in pregnancy70 although they can be technically difficult with a gravid uterus.71 Of note, those with CSF shunts inserted before becoming pregnant can have a normal pregnancy and delivery.70 72
Optic nerve sheath fenestration is less commonly performed, as evidenced from data from the UK73 and in the USA74 due to limited local surgical expertise, the complication rate and scanty data on the longevity of the procedure.68 75 Furthermore, the procedure decompresses the optic nerves but does not necessarily help the headache. Given the possible problems with CSF shunting, optic nerve sheath fenestration may be preferable if there is local expertise.
Dural venous sinus stenting requires preprocedure and postprocedure anticoagulation, which would potentially further complicate pregnancy.75 It is rarely performed in the UK73 and its use remains controversial, with evidence only from case series and no randomised clinical trials.75 76 A randomised controlled trial comparing CSF shunting with venous sinus stenting in IIH is ongoing in the UK (IIH: Intervention). Therefore, in our opinion, we would not recommend this in pregnancy. Interestingly, one report noted that venous sinus stenting failed, with a recurrence rate of 10% following becoming pregnant.77
Delivery and peripartum
Patients with IIH do not need any specific mode of delivery and there is no clear evidence to support the reported trend towards caesarean section.78 The concern in theory is that a prolonged second stage of labour, with consequent Valsalva manoeuvre, could exacerbate optic nerve ischaemia and damage, but in reality the duration of contractions during the second stage of labour are relatively short. Our clinical impression (we have managed >50 cases) is that there no evidence of declining vision following labour. In practice, a normal vaginal delivery poses a negligible risk to women with IIH and in addition caesarean sections are associated with their own risks both intra and post operatively. The mode of delivery should therefore be decided by obstetric factors only.8 70 However, we would advise caution in those rarer cases with severe papilloedema who have rapidly declining vision at delivery; such patients should be managed in a specialist centre.
Lumbar punctures and spinal anaesthesia are safe in pregnancy. We do recommend caution, and where possible avoidance, if there is a lumbar peritoneal shunt in situ.
Conclusion
Pregnancy in IIH requires additional considerations. Ideally women should achieve disease remission or stabilisation before pregnancy. Drugs including acetazolamide and topiramate have teratogenic risks and we avoid these during pregnancy. An important aspect is the risk of weight gain during pregnancy, as this can exacerbate IIH. There are useful guidelines on weight gain targets in pregnancy for those with obesity; these should be actively discussed with the patient and supported. We recommend increased frequency of IIH outpatient reviews during pregnancy to identify any clinical deterioration early and provide reassurance.
Case vignettes
Scenario 1
A 28-year-old woman with mildly active IIH (normal visual fields). Her headache frequency has improved following topiramate monotherapy (100 mg nocte). Her BMI is 36 kg/m2 with only minimal weight reduction since presentation. She is not using any contraception, is in a relationship and now has plans for children.
Bespoke recommendations would include a sensitive discussion regarding weight management and family planning. We would recommend weaning the topiramate before trying to conceive and suggest folic acid supplementation. Should pregnancy occurs while on topiramate, we would stop topiramate or wean over a week if on higher doses, with close monitoring of the ocular status.
Scenario 2
A 26-year-old woman with IIH, 25 weeks pregnant has a 2 week history of deteriorating vision, with transient visual obscurations and increased pulsatile tinnitus. She undergoes a full assessment of visual function including visual fields and OCT imaging. Her visual acuity is 6/7.5 bilaterally, perimetric mean deviation −3 dB right eye and −2.75 dB left eye (in a well performed Humphrey visual field). The global peripapillary RNFL thickness is 220 µm (right eye) and 200 µm (left eye), in properly segmented scans. Given her symptoms, if left she will be at risk of potential visual loss. We recommended emergency lumbar puncture with a cutting needle. She was re-evaluated 2 days later and the papilloedema had reduced on OCT examination (RNFL 188 µm right eye and 172 µm left eye). One week later, there had been a further reduction, no further intervention was organised, and she remained under close observation until she had a normal delivery.
However, if her OCT had shown that the papilloedema was increasing beyond what was noted the previous week we would have considered a lumbar drain. If we determined that she had rapidly declining vision with increasing papilloedema on OCT imaging and that this approach was unsuccessful, we would escalate to an emergency CSF diversion procedure.
Key points
Prepregnancy care should aim for remission or stability of idiopathic intracranial hypertension (IIH); hormonal contraception is not contraindicated.
Acetazolamide and topiramate have teratogenic risks and we advise avoiding them in women actively planning a pregnancy or those who become pregnant.
Women with IIH require frequent and active monitoring throughout pregnancy.
Pregnancy weight gain can exacerbate IIH; those with a prepregnancy body mass index (BMI) ≥30 kg/m2 should be guided to gain less weight in pregnancy than those with lower BMIs.
Further reading
Mollan SP et al. Idiopathic intracranial hypertension: consensus guidelines on management. J Neurol Neurosurg Psychiatry 2018 89(10):1088–1100.
Santos S et al. Impact of maternal body mass index and gestational weight gain on pregnancy complications: an individual participant data meta-analysis of European, North American and Australian cohorts. BJOG 2019 126(8):984–995.
Mollan SP, A.A. Tahrani and A.J. Sinclair. The Potentially Modifiable Risk Factor in Idiopathic Intracranial Hypertension: Body Weight. Neurology Clinical Practice 2021, doi:10.1212/CPJ.0000000000001063.
Ethics statements
Patient consent for publication
References
Footnotes
Twitter @MarkHeadache, @AbdTahrani, @DrMollan, @DrIIHBirmingham
Contributors All authors have contributed to the creation and review of this manuscript.
Funding AJS is funded by a Sir Jules Thorn Award for Biomedical Science.
Competing interests BRW—Invex therapeutics consultancy AAT—I have received support for research and meetings, honorarium for advisory work and equipment support from: ANSAR, Aptiva, AstraZeneca. Bristol-Myers Squibb, Boehringer Ingelheim, Eli Lilly, ImpetoMedical, Janssen, Merck Sharp & Dohme, Napp, Novo Nordisk, Philips Resporinics, Resmed, Sanofi Aventis. SPM—Invex therapeutics, advisory board (2020) and consulting fees (2021); Heidelberg engineering, speaker fees (2021); Neurodiem, advisor (2019, 2020, 2021); Novartis, speaker fees (2020); and Scope Ophthalmics, speaker fees (2021). AJS - Novartis and Allergan Advisory board. Speaker fees Novartis. Invex therapeutics, company director with salary and stock options (2019, 2020) No other authors contributing have a conflict of interest in the subject matter.
Provenance and peer review Provenance and peer review. Commissioned. Externally peer reviewed by Angela O’Neal, Boston, USA.
Linked Articles
- Editors’ commentary
Other content recommended for you
- Idiopathic intracranial hypertension: consensus guidelines on management
- A practical approach to, diagnosis, assessment and management of idiopathic intracranial hypertension
- Evolving evidence in adult idiopathic intracranial hypertension: pathophysiology and management
- Venous sinus stenting shortens the duration of medical therapy for increased intracranial pressure secondary to venous sinus stenosis
- Dural venous sinus stenting for treatment of pediatric idiopathic intracranial hypertension
- Detection of intracranial hypertension in children using optical coherence tomography: a systematic review
- Guiding follow-up of paediatric idiopathic intracranial hypertension with optical coherence tomography
- The impact of gestational weight gain in different trimesters of pregnancy on glucose challenge test and gestational diabetes
- Risk factors associated with progression from papilloedema to optic atrophy: results from a cohort of 113 patients
- Negative impact of COVID-19 lockdown on papilloedema and idiopathic intracranial hypertension