Article Text

Abstract
Radiation therapy is widely used for benign and malignant brain tumours as it is effective and well tolerated. However, damage to the surrounding healthy nervous system tissue leads to a variety of complications both in the short term and long term, ranging from mild and self-limiting to irreversible and fatal. Radiation neurotoxicity is due to a combination of early inflammation and oligodendroglial damage followed later by brain tissue necrosis, white matter damage, accelerated vascular disease and the development of secondary tumours. This article explains the basic principles of radiation physics, the different modalities used in clinical practice, how radiotherapy is planned and delivered and the scientific basis of radiation damage. The main body of the article focuses on the clinical features of radiation toxicity in the brain, spinal cord, cranial and peripheral nerves with an emphasis on the distinction between early and delayed complications.
- radiotherapy
- cerebrovascular disease
- clinical neurology
- cognition
- dementia
Data availability statement
No data are available.
Statistics from Altmetric.com
Introduction
Radiation therapy is used to treat a range of malignant and benign conditions of the brain, skull base and adjacent structures with curative and palliative intent. The treatment can be delivered using various techniques, taking advantage of the specific characteristics of the different modalities and platforms for delivery. The most commonly used modality is external beam radiation with photon therapy, in the form of X-rays or gamma rays. X-ray photon treatments can easily penetrate through tissues and are usually prescribed in daily sessions (fractions) using a linear accelerator, with the total radiation dose being delivered over several weeks. The precise dose fractionation depends on the type of target and clinical indication. Some smaller tumours, such as vestibular schwannomas and meningiomas, can be treated with radiation therapy in a single treatment session (stereotactic radiosurgery) or a number of sessions (stereotactic radiotherapy), while larger tumours such as gliomas require multiple fractions, usually over 3–6 weeks. Alternative delivery platforms include Gamma Knife (Elekta, Stockholm, Sweden) or Cyberknife (Accuray, California), which can provide more conformal radiation dose distributions to smaller targets. However, techniques for undertaking stereotactic treatments on standard linear accelerator platforms have also been developed and continue to evolve.
Proton beam therapy uses the specific physical properties associated with the dose deposition of a particle beam in tissue, namely, that most of the energy is delivered at the distal end of its range, immediately before the particle comes to rest—known as the Bragg peak. When planned accordingly, this can increase the dose deposited in the clinical target and minimise the dose to normal tissues beyond the Bragg peak. There are two main indications for proton beam therapy in clinical practice1: for dose escalation to radioresistant tumours such as skull base chordoma or chondrosarcoma, at sites where standard photon radiotherapy cannot deliver the necessary dose due to the proximity of critical structures2; to reduce radiation therapy toxicities to the brain and surrounding soft tissues, particularly in children, teenagers and young adults, for whom the negative effects of irradiating the developing brain are more pronounced.
Mechanisms of radiation damage
Irradiation of tissue causes different types of DNA damage through the production of highly reactive free radicals: single-strand break, double-strand break (the major lethal lesion), base damage and DNA crosslinks. A range of DNA damage repair mechanisms operate to help maintain genomic stability. However, some lesions fail to repair adequately, and it is the accumulation of these lesions that may eventually lead to cell death, either by a programmed mechanism such as apoptosis or autophagy or via mitotic catastrophe at a future cell division. If the damage does not cause cell death, it may lead to a late manifestation of radiation such as the development of a secondary tumour, sometimes several years or decades after radiation exposure.1
The precise mechanisms responsible for radiation toxicity of the nervous system are incompletely understood. For example, several processes have been hypothesised to explain radiation-induced neurocognitive decline with a range of preclinical and clinical data to support them. There is evidence that radiation reduces neurogenesis in the hippocampus, with preclinical models showing a depletion of neural progenitor cells occurring over the course of multiple cell divisions. Changes in the cellular microenvironment are also a major factor in the determination of cell fate and reduction in neurogenesis. The oxidative stress induced by radiation results in upregulation of proinflammatory pathways and an increase in number of activated microglia, which act as potent inhibitors of neurogenesis. Radiation can also trigger the death of endothelial cells, causing thrombus formation on the exposed matrix and small vessel occlusion. Furthermore, accelerated atherosclerosis and microangiopathy after radiation can lead to vascular insufficiency and infarction.2
Radiotherapy treatment planning
There are multiple linked processes involved in the planning and delivery of a course of radiation therapy. Initially, the patient undergoes CT imaging while immobilised in the treatment position, usually via a thermoplastic head shell. Diagnostic MR images obtained previously are coregistered with the planning CT scan and used to delineate the treatment targets and relevant organs at risk. This is known as the gross target volume. Depending on the underlying tumour histology, the radiotherapist will delineate an appropriate margin around the visible tumour to account for possible microscopic infiltration (Clinical Tumour Volume), and a small additional margin is then added to account for small movements that can occur even within the immobilisation device. This final volume is called the planning target volume. The radiotherapy dosimetrists and physicists create a treatment plan that delivers the prescribed dose homogenously to the planning target volume, while ensuring that the organs at risk do not receive more than the maximum allowed. Figure 1 shows an illustrative case.

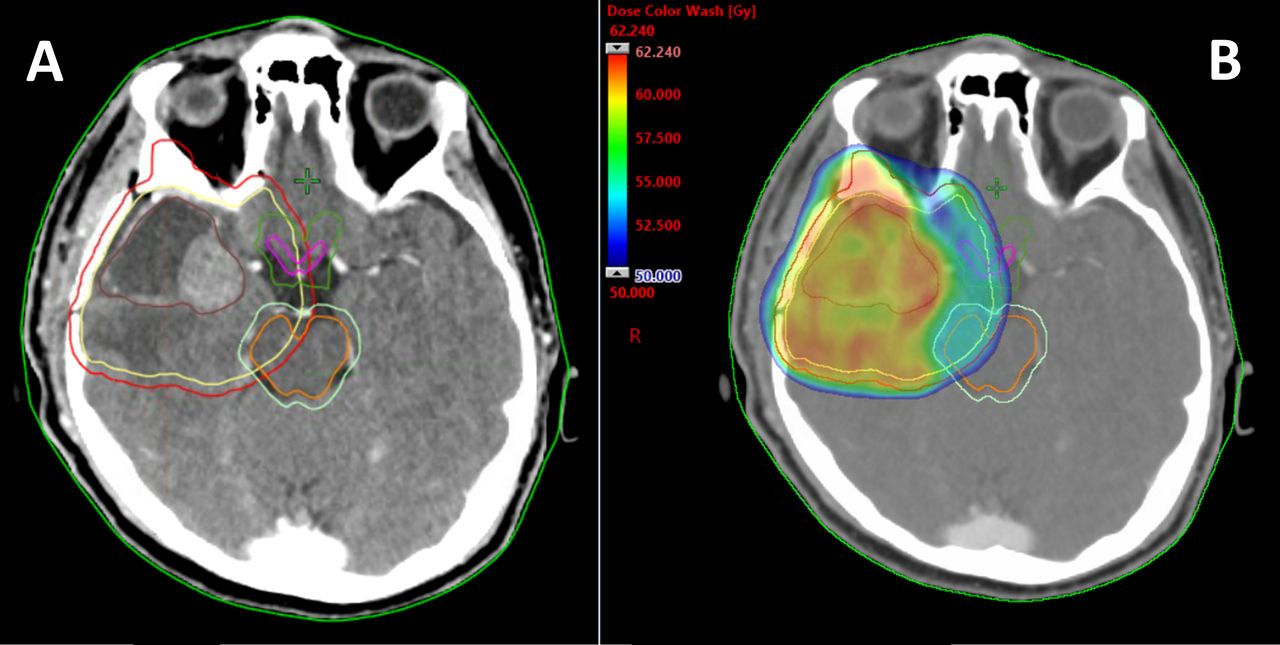
Radiation treatment planning CT scan of head showing a right temporal glioblastoma. (A) Volume delineation of target and organs at risk (OARs): brown=postoperative tumour bed and residual enhancing gross tumour (GTV); yellow=clinical target volume (CTV), area at risk of microscopic disease infiltration, defined as GTV+2 cm for glioblastoma, edited off barriers to spread (eg, bone); red=planning target volume (PTV), CTV+geometric 3 mm margin for positional inconsistencies within immobilisation device; pink=optic chiasm; dark green=3 mm margin around chiasm for positional inconsistencies; orange=brainstem; light green=3 mm margin around brainstem for positional inconsistencies. (B) Radiotherapy dose distribution >50Gy: prescription dose to PTV of 60 Gy. Note compromise of PTV dose coverage medially due to the location of the brainstem and optic chiasm within the high dose volume. This radiotherapy plan was designed to ensure that no dose >55 Gy was delivered to these critical OARs.
The constraints on radiation dose owing to organs at risk are defined from the literature based on clinical and preclinical radiobiological data. Each major structure within the nervous system has a particular dose constraint associated with it, and these constraints are often given greater priority in the radiotherapy planning process than treating the target, meaning that planning target volume dose coverage is compromised to avoid the risk of significant radiation-induced toxicities. For example, the dose constraint to the optic chiasm is 55 Gy. Published data reveal that doses above 55 Gy lead to an incrementally higher risk of radiation-induced optic neuropathy: <3% at 5-year postradiation therapy when <55 Gy delivered rising to 7% at 5 years at 55–60 Gy.3
Radiotherapy dose fractionation
The relationship between radiation dose and cell survival varies between tissues. Cells may be killed by a single lethal radiation hit or by a succession of sublethal hits. In addition to the overall radiosensitivity of certain tissues, there is also a difference in sensitivity to treatment fraction size. For example, the difference in biological effect of treating to a dose of 20 Gy in 10 daily fractions (2 Gy per fraction) versus 20 Gy in 5 daily fractions (4 Gy per fraction) will vary between tissues depending on their sensitivity to fraction size.4 This fraction size sensitivity is most commonly expressed using the alpha–beta ratio, which incorporates a linear component (alpha) of lethal cell kill and a quadratic component (beta) of sublethal cell kill. Fractionating treatment, that is, splitting the total dose up into multiple smaller radiation doses, allows for repair to sublethal damage between fractions. This is more effective in normal tissues than in tumour tissue, so fractionating treatment can increase the therapeutic ratio between tumour control and normal tissue damage. Unlike many tumour cell types, the normal tissues of the nervous system are particularly sensitive to changes in fraction size. Therefore, splitting radiation treatment into multiple fractions over several weeks facilitates more sublethal damage repair in these normal tissues than if the same overall radiation dose was delivered over a shorter overall treatment time.5
Radiation complications in the brain
Early complications
Acute radiation encephalopathy
Acute radiation encephalopathy appears within 2 weeks of the start of brain radiation therapy and occasionally a few hours after the first fraction. The most common symptoms are drowsiness, headache, nausea and vomiting together with a worsening of pre-existing neurological deficits. The main risk factor is the size of the tumour and the dose per fraction (usually >3 Gy/fraction). It rarely occurs nowadays as dose fractionation is restricted and large tumours are routinely debulked before radiation therapy. Patients usually recover quickly although herniation and death have been reported. In an older series, acute radiation encephalopathy occurred in half of patients with brain metastases treated with 15 Gy in two fractions.6 As the conventional dose fractionation for whole brain radiotherapy nowadays is either 20 Gy in five fractions over 1 week or 30 Gy in 10 fractions over 2 weeks,7 this complication almost never occurs.
Sometimes patients report nausea and moderate headache on the evening after the first fraction of radiation therapy. Corticosteroids may help especially in patients with large tumours or with considerable oedema particularly at risk of herniation. Where surgical debulking is not possible, these patients should be prescribed dexamethasone 16 mg per day 2–3 days before the first fraction and the dose per fraction ideally limited to 2 Gy. The pathophysiology of acute radiation encephalopathy probably results from radiation-induced blood-brain barrier disruption, accounting for a rise in intracranial pressure.
Early-delayed radiation encephalopathy
Early-delayed radiation encephalopathy is so called as it starts from 2 weeks to 6 months after completing radiation therapy. The pathophysiology is probably transient demyelination caused by blood-brain barrier disruption and/or oligodendroglial injury. The most common symptoms include fatigue, drowsiness, lethargy, memory and attentional deficits. At its worst, patients may be asleep for most of the day. Somnolence syndrome, characterised by hypersomnolence, nausea and anorexia, was first described in children receiving low-dose radiation therapy for scalp ringworm and after prophylactic cranial radiation therapy for leukaemia; it occurs less commonly in adults. The diagnosis is clinical as neither MR imaging nor EEG shows specific changes. Patients usually improve within a few weeks. There may be a biphasic course with symptoms appearing from days 11 to 21 and then again from days 31 to 35.8 As a result, many oncologists continue corticosteroids during and after radiotherapy.
Pseudoprogression
About 6–12 weeks after the end of radiation therapy, patients may experience worsening of pre-existing neurological deficits, leading to the suspicion of tumour progression. Imaging is usually unhelpful as the MRI may show appearances of tumour progression that resolve over the next few months without any specific antitumour intervention. This phenomenon is known as ‘pseudoprogression’ and occurs in up to 30% of patients with glioblastoma treated with concomitant temozolomide and radiotherapy. Ironically, pseudoprogression may be associated with a better tumour response.9 Patients usually improve within a few weeks or months associated with slow radiological improvement. Advanced imaging techniques such as perfusion-weighted imaging and MR spectroscopy may help to distinguish pseudoprogression from true progression but interpretation is limited by the presence of residual tumour within the irradiated area.
Some patients report poor attention and memory for up to 6 months following brain radiation therapy, which reassuringly does not predict the development of long-term cognitive decline. We, therefore, warn patients who are keen to resume work immediately after radiation therapy that they should inform employers about the possibility of a delayed or phased return.
Brainstem syndrome
An early-delayed subacute brainstem syndrome can occur 1–3 months after radiation therapy for pituitary or head and neck cancer, where the treatment fields overlap the brainstem. Clinical features include ataxia, dysarthria, diplopia and/or nystagmus as well as hearing loss. MR brain scan sometimes shows high signal change within the white matter of the brainstem and the cerebellar peduncles, which may enhance. This condition usually responds to corticosteroids within a few weeks; very rarely it results in coma and death.
Late complications
Late complications usually start 6–12 months after completing radiation therapy but can be delayed by many years or even decades. The two main complications are radionecrosis and late-delayed radiation encephalopathy.
Radionecrosis
Radionecrosis is the most common late complication and was first described pathologically in 1948 in a series of patients, one of whom had a recurrent ‘rodent ulcer of the scalp’ and a normal brain.10 It can be difficult to distinguish from tumour recurrence both clinically and radiologically. Nowadays, radionecrosis most commonly follows focal radiation therapy for a brain metastasis but can also occur in patients who have had radiation therapy for extracranial and extra-axial tumours, in whom normal brain was included within the radiation field (eg, head and neck cancer, skull osteosarcoma, pituitary adenoma, clival chordoma). A typical example is bilateral medial temporal lobe necrosis following radiation therapy for pituitary tumours (figure 2) or nasopharyngeal cancer. It is seen less often nowadays due to reduction in dose per fraction and improvements in the delivery of radiation therapy. It is now recognised that the upper limits of a ‘safe dose’ of 55–60 Gy administered to a focal field with fractions of 1.8–2 Gy per day are associated with a less than 5% risk of radionecrosis. Patients with vascular risk factors such as hypertension, diabetes and old age are at higher risk of radionecrosis, as are those who have concomitant chemotherapy. Some patients without any particular risk factors may develop radionecrosis, probably because of increased sensitivity to radiation, such that they develop this complication at conventional dose fractionation.11

Radiation necrosis. A 37-year-old patient presenting with severe amnesia 4 years following proton beam therapy for a pituitary adenoma. Axial T2W (A), T1W+gad (B) images show bilateral temporal signal change and oedema with irregular enhancement in medial temporal lobes, typical of radiation necrosis. There was no improvement with corticosteroids and the patient remained severely incapacitated by fatigue and amnesia.
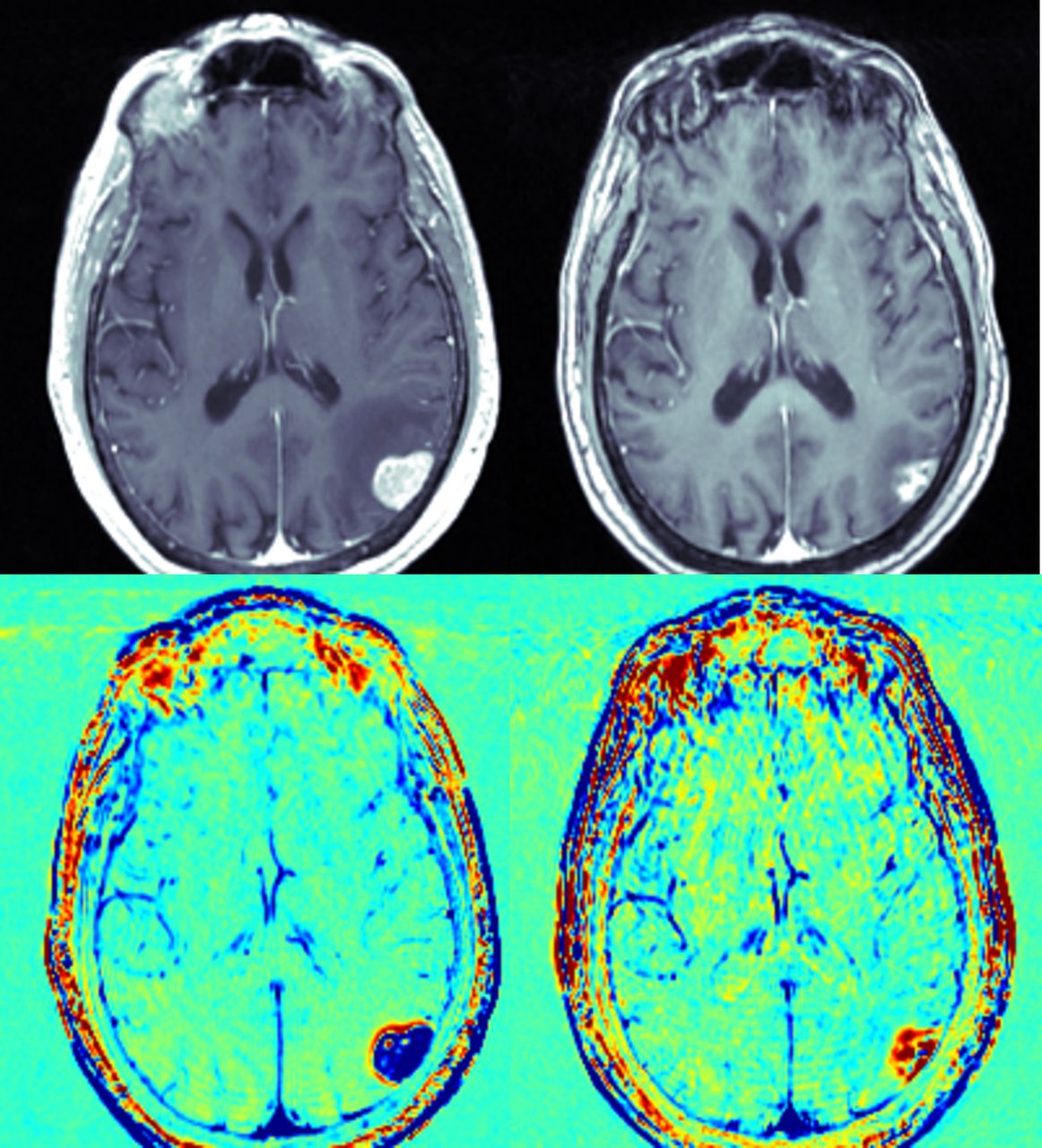
Radionecrosis nowadays most commonly occurs after stereotactic radiosurgery, for example, Gamma Knife treatment for brain metastases (5%–25% of cases) and also for non-neoplastic conditions such as arteriovenous malformations (up to 20% of cases). Symptoms of radionecrosis are indistinguishable from those of tumour recurrence or progression and brain imaging is likewise similar. More recently, an MRI sequence with delayed contrast sequences known as TRAMS (treatment response assessment maps) or contrast clearance analysis has become routinely available in clinical practice as it is both sensitive and specific.12 It requires the acquisition of two standard 3D T1-weighted MR brain scans—one 5 min after injection of gadolinium and another after an hour. The first series is digitally subtracted from the second. The analysis results in high-resolution, volumetric maps that can distinguish regions of contrast clearance (blue) from contrast accumulation (red). Radionecrosis shows up as red due to the poor clearance of contrast in non-viable tissue-containing irradiated vessels, while tumour recurrence shows up as blue due to the rapid clearance through tumour vasculature (figure 3).

Treatment response assessment maps (TRAMS)/contrast clearance analysis maps contrast-enhanced T1-weighted MRI (T1-Gd, top) and the calculated TRAMS image (bottom) of a patient receiving stereotactic radiosurgery for a malignant melanoma brain metastasis. Before the radiosurgery (left) the enhancing lesion on T1-Gd appears blue in the TRAMS scan. Follow-up MR scan of brain 10 months following stereotactic radiosurgery (right) shows significant shrinkage of the enhancing lesion on T1-Gd, appearing red, suggesting radiation necrosis. (Courtesy of Prof Yael Mardor, Sheba Medical Centre, Israel).
Refractory cases of radionecrosis are treated with dexamethasone and resection of necrotic foci. Corticosteroid dependence can occur. Other treatments such as hyperbaric oxygen or drugs such as pentoxifylline, alpha-tocopherol and pentobarbital have also been tried but without clear evidence of efficacy. A recent systematic review concluded that bevacizumab appeared to be more effective and just as safe as corticosteroids.13
Late-delayed radiation encephalopathy
It has been known for many years that radiotherapy can cause delayed cognitive impairment that varies from mild memory loss to a severe dementia.14 This complication develops more frequently in adult survivors of childhood brain tumours and in patients with low-grade gliomas where the tumour remains in remission for many years.15 MRI shows variable degrees of high T2W signal change in the subcortical white matter and brain atrophy. Some patients deteriorate slowly while most remain stable. Cerebral atrophy may also be strikingly focal where specific lobes of the brain have been irradiated (figure 4). This syndrome has no recognised treatment although some authors have advocated using anticholinesterases for symptomatic benefit.16

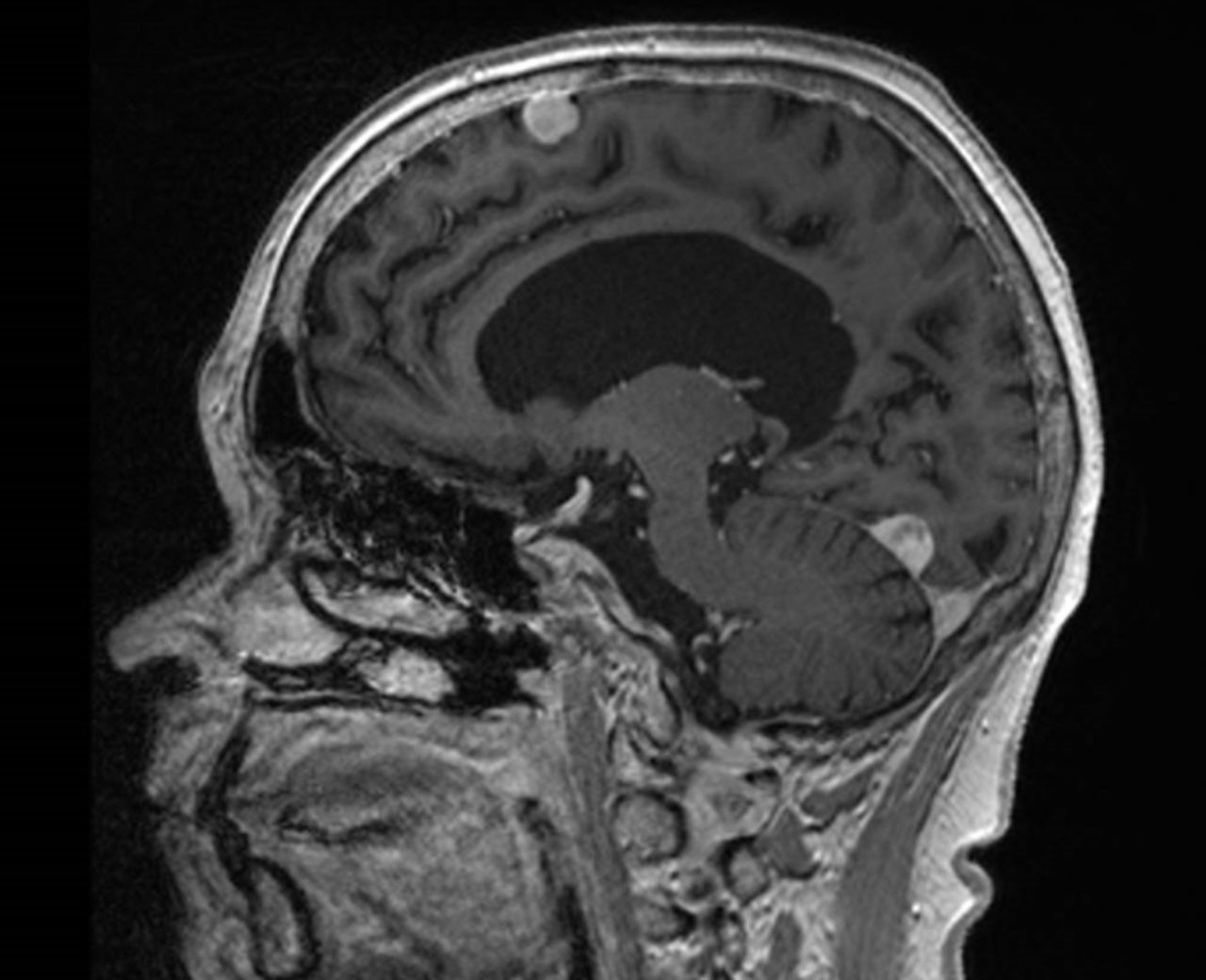
Delayed radiation encephalopathy. A 55-year-old patient treated with bifrontal parallel fields to a right frontal glioma in 1997, presenting with progressive cognitive and behavioural decline 25 years later. Sagittal (A) and coronal T1W (B) shows striking bifrontal and perisylvian atrophy with relative preservation of the parietal and occipital lobes. Note the enhancing residual tumour.
The long-term cognitive effects of radiotherapy in patients with low-grade gliomas have been reported in a study comparing 195 patients with low-grade glioma (of whom 104 had been treated with radiotherapy) with a matched series of patients with low-grade haematological malignancies and healthy controls, followed up for at least 6 years. Patients with low-grade glioma experienced significant problems across a range of Health-Related Quality of Life domains, including neurocognitive deficits, but these were associated with tumour changes. Only high dose per fraction (>2 Gy) resulted in significant added cognitive decline.17 Interestingly, the same group published their findings after a follow-up of 12 years and found that the patients who had received radiotherapy even at doses less than 2 Gy/fraction showed a progressive decline in attentional and executive functioning and speed of information processing. Fifty-three per cent patients who had radiotherapy developed cognitive deficits in at least five of 18 neuropsychological test areas compared with 27% patients who had not received radiation therapy.18
Whole brain radiotherapy was the standard treatment for brain metastases until the last decade but causes cognitive decline in over 60% of patients within 2–6 months of treatment. It has now been replaced by stereotactic radiosurgery for fit patients with stable or controlled extracranial disease and a reasonable prognosis from their underlying cancer (at least 6 months).19 Hippocampal sparing techniques are gaining in popularity for patients with brain metastases who are not suitable for treatment with stereotactic radiosurgery, but these techniques have not yet been shown to provide a consistent cognitive advantage
In patients with primary CNS lymphoma who have been traditionally treated with combined high-dose intravenous methotrexate chemotherapy followed by whole brain radiotherapy, the incidence of severe cognitive impairment increases with age, reaching 83% in patients over 60 years.20 Based on the results of a randomised phase 2 study by a European consortium (the IELSG-32 study), the standard of care across Europe for fit patients with primary CNS lymphoma aged under 70 years is now a chemotherapy regimen known as Methotrexate, Ara-C, Thiotepa and Rituximab (MATRIX) followed by autologous stem cell transplantation, a strategy that avoids using whole brain radiotherapy altogether, thus reducing potentially fatal neurotoxicity.21
Radiation-induced secondary normal pressure hydrocephalus
Radiation-induced dementia is characterised by a ‘subcortical dementia’ pattern associated with diffuse white matter injury, usually starting within 2 years of treatment. Patients may present with a picture similar to normal pressure hydrocephalus and develop progressive memory loss, reduced attention, gait difficulties, urinary incontinence and fatigue. There may be emotional lability and apathy that is difficult to distinguish from depression. Antidepressants are frequently tried but do not improve cognitive function. Eventually, patients may develop akinetic mutism. MR scan of brain shows ventricular enlargement, diffuse confluent subcortical white matter change, with cortical and subcortical atrophy.
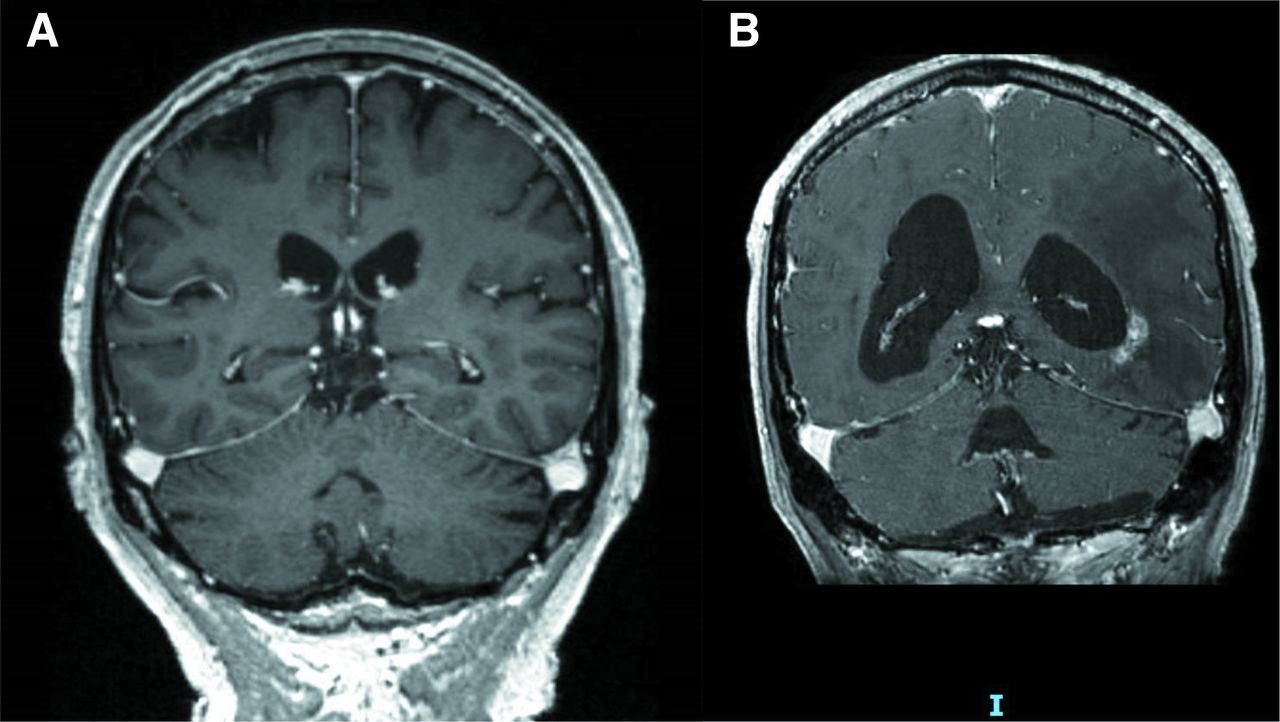
There is no specific treatment for radiation-induced dementia. However, ventriculoperitoneal shunting is sometimes tried with incomplete and short-lived improvement (figure 5).22 Deterioration occurs in about 80% of cases and death generally occurs within 4 years after the onset of the disorder.
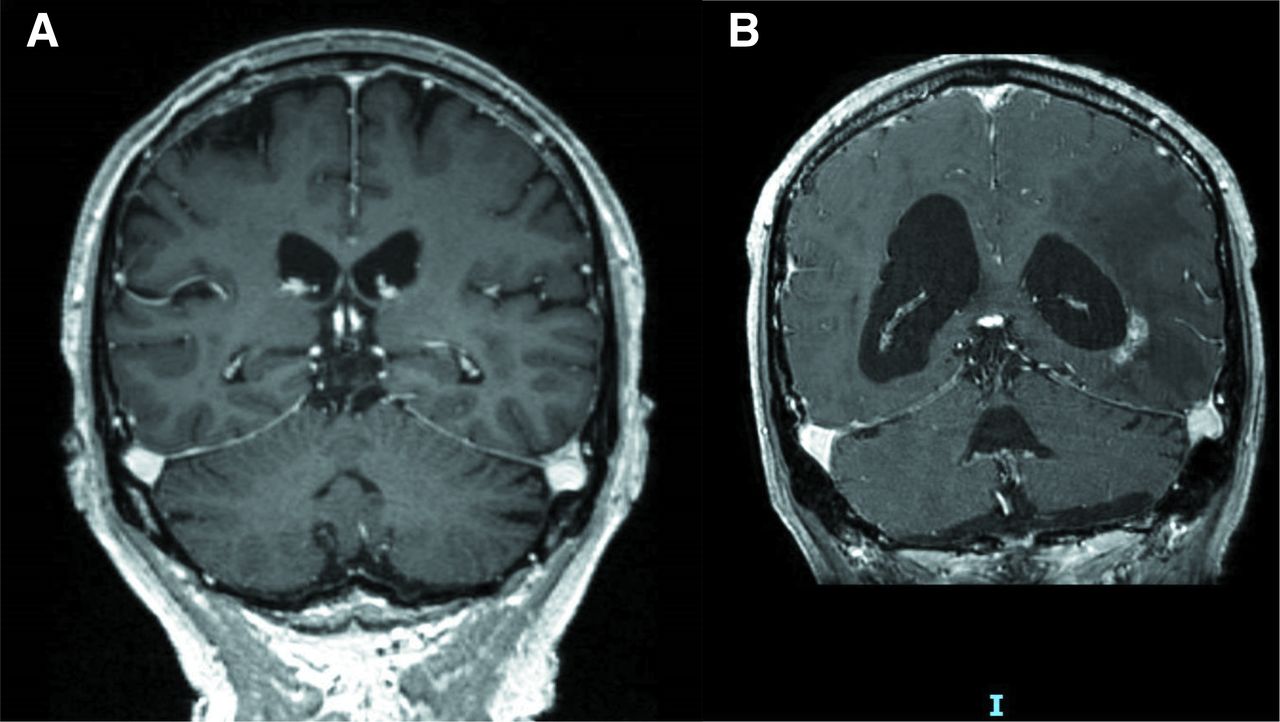
Secondary normal pressure hydrocephalus. A 66-year-old with left occipital glioblastoma treated with concomitant chemoradiation. Within a year of radiotherapy (54 Gy in 30 fractions) she became increasingly unsteady due to an apraxic gait with urinary incontinence and mild memory loss. Her condition improved with ventriculoperitoneal shunting but the improvement was short-lived and she died of progressive disease 9 months later. Coronal T1W post-Gd immediately after radiotherapy (A) showing normal ventricular dimensions and 1 year later (B) showing dilatation of posterior horns and fourth ventricle and sulcal effacement. Note tumour recurrence around the left lateral ventricle with surrounding oedema.
Radiation-Induced brain tumours
Irradiated patients are more prone than the general population to developing second brain and spine tumours. Meningiomas (70%) (figure 6), gliomas (20%) and sarcomas (10%) are the most common tumours and develop many years (mean onset 12 years) or decades after treatment. In a study of over 10 000 patients treated for tinea capitis with low-dose (1.5 Gy) radiation, the relative risk for all tumours was 6.9 and the risk for glioma was 2.6.23 This has been confirmed in several other studies. In patients treated for childhood acute lymphoblastic leukaemia, the relative risk is so high22 as to justify screening MR brain imaging for adult survivors.24
Radiation induced meningiomas. A 48-year-old patient presenting with new onset generalised seizures; she had received whole brain radiotherapy 30 years previously for a pineal germinoma. Coronal contrast-enhanced T1W image shows two meningiomas both within the midline, one arising from the falx and one from the tentorium, with no evidence of tumour recurrence in the pineal gland.
In order to diagnose a radiation-induced tumour, there must be a long interval between the treatment and the occurrence of the second tumour (there have been cases developing over 60 years later), the tumour has to grow within the radiation field or at its margins, and be of a different histological subtype to the primary tumour. These tumours have a poor prognosis as such patients have limited reserve for further radiotherapy. However, the longer the gap between the original treatment and the secondary tumour, the more scope there may be due to normal tissue recovery.
Radiation-Induced vasculopathy
Radiation can damage the intracranial vasculature leading to ischaemic stroke or haemorrhage. The carotid artery can become stenotic after cervical radiotherapy for lymphomas or head and neck cancers and occasionally can rupture a few weeks after radiation therapy causing death. However, late-delayed complications are more frequent and generally occur many years after treatment (median time about 20 years for extracranial arteries, 7 years for intracranial arteries). Radiation-induced vasculopathy is an accelerated form of atherosclerosis and often occurs in unusual locations, for example, the distal internal carotid artery. It has been described within 2 years of proton beam therapy for childhood brain tumours.25 The lesions consist of one or more arterial stenoses or occlusions of the carotid or cerebral arteries within the radiation portal. Pathological findings include destruction of the internal elastic lamina and replacement of the normal intima and media with fibrous tissue. Treatment includes managing vascular risk factors and, where appropriate, carotid endarterectomy. However, surgery may be more difficult because of vascular fibrosis and poor wound healing. If a patient with previous radiation therapy develops a stroke, it should not be assumed to be due to radiation vasculopathy unless it is within the radiation portal, and other risk factors should be sought.
Moyamoya disease
Moyamoya disease is a progressive occlusive cranial vasculopathy characterised by abnormal anastomoses and netlike blood vessels at the apices of the intracranial internal carotid arteries, the proximal anterior cerebral arteries and middle cerebral arteries.26 It results in decreased cerebral blood flow with an increased risk of stroke, transient ischaemic attacks and focal seizures. It often develops in patients who had cranial radiation therapy as young children, particularly those treated for optic chiasm glioma, a condition often associated with neurofibromatosis type 1, which is a risk factor for vasculopathy in itself. The strong association between neurofibromatosis type 1 and moyamoya is one of the reasons why radiation has been replaced with chemotherapy in younger children with optic pathway gliomas. Treatment is aimed at preventing further strokes through surgical revascularisation procedures.
Radiation-induced cavernomas, angiomatous malformations and aneurysms
Vascular malformations such as telangiectasias and cavernomas are increasingly being recognised as a long-term complication of brain radiotherapy, due to the routine inclusion of gradient-echo and susceptibility weighted sequences in modern MRI protocols. When present, their main risk is intracranial haemorrhage, but this is rare.27 There have been occasional cases of radiation-induced intracranial aneurysms reported with fatal outcomes.
SMART syndrome
Stroke-like migraine attacks after radiation therapy (SMART syndrome) is a poorly understood late complication of brain radiation therapy for both primary and secondary brain tumours. It presents with a combination of migraine-like headaches and cortical dysfunction including seizures and focal neurological deficits, for example, aphasia, neglect and hemiparesis. Seizures may be prolonged and respond poorly to antiseizure medication. Corticosteroids do not seem to help. It has a distinctive radiological appearance with pial enhancement and cortical high signal change within the radiotherapy field. It is now recognised that neurological deficits can persist even after radiological improvement.28 There is imaging evidence (from CT perfusion studies) that SMART syndrome is caused by reversible hemispheric hypoperfusion,29 but there is often elevated relative cerebral blood volume in the acute phase on dynamic susceptibility contrast perfusion MR imaging (figure 7). There is no known treatment for SMART syndrome although anecdotally, L-arginine has been used to good effect in two reported acute cases. One of our patients who had four previous severe attacks of SMART every 15 months has not had an attack for 3 years since taking L-arginine, which is available without prescription and non-toxic.

SMART syndrome. A 68-year-old patient who had received radiation therapy 8 years previously for a left frontal astrocytoma. He subsequently developed a rapid onset of continuous focal motor aware seizures, loss of speech and right hemiparesis that gradually improved over the next 3 months, leaving him with moderate dysphasia and mild hemiparesis. There was no response to high-dose intravenous corticosteroids. Imaging at the onset shows swollen left hemisphere with diffuse high signal and sulcal effacement on axial T2W (A) and pial enhancement (B) with high relative cerebral blood volume on perfusion-weighted imaging (C). The appearances had resolved and returned to baseline 3 months later (D and E).
Radiation complications in the spinal cord
Radiation therapy damages the cord in much the same way as with the brain although is less commonly encountered, due to the relative rarity of spinal cord tumours compared with brain tumours. However, the spinal cord is a critical organ at risk in the planning and delivery of radiation therapy for non-CNS tumours, including head and neck and paravertebral cancers. Early and late-delayed myelopathy, lower motor neurone disorder and spinal haemorrhage have all been described.
Early-delayed radiation myelopathy
This usually follows radiation to the cervical or thoracic cord, most commonly after mantle radiation therapy for Hodgkin’s disease within the cervical cord. The clinical symptoms include Lhermitte’s phenomenon, presumably caused by transient demyelination in the posterior columns, secondary to oligodendroglial cell loss. There is no specific treatment for this condition and recovery is the norm. It is important to reassure patients that this does not evolve to a progressive myelopathy.
Late-delayed radiation myelopathy
Late-delayed radiation myelopathy occurs 1 to 10 years after exposure to radiation therapy and, as with brain neurotoxicity, risk factors include older age, total radiation dose (above 60 Gy), higher dose per fraction and the volume of cord irradiated. Late-delayed radiation myelopathy presents with a combination of slowly progressive sensorimotor deficits, a hemicord (Brown-Séquard) syndrome, with bladder involvement eventually leading to paraparesis or tetraparesis. MR imaging may be initially normal but usually the cord becomes swollen and, in about half of cases, there is gadolinium enhancement. Eventually, there is cord atrophy with occasional cystic cavitation. The diagnosis can be made only if the cord signal change lies within the radiation-exposed area and if having excluded all other potential causes of myelopathy. The natural history varies—in some patients, the symptoms stabilise, in others, they progress to a complete deficit.
Neuropathological findings include demyelination, focal necrosis and axonal loss, together with fibrinoid necrosis of the vessel walls, perivascular fibrosis and sometimes vasculitis.
Corticosteroids can help in the subacute stages to reduce the inflammatory component of the disorder; however, patients often become steroid dependent and only a few experience long-term improvement. There is no current proven treatment although hyperbaric oxygen and anticoagulation have both been tried in small series.
Lower motor neurone syndrome
A lower motor neurone syndrome resembling motor neurone disease has been described after radiation therapy to the distal spinal cord and cauda equina, mainly as treatment for testicular cancer and lymphoma. It presents with progressive proximal and/or distal symmetrical leg weakness associated with muscle fasciculation and wasting, but with normal sensation.30 Sphincter disturbance and sensory loss may appear much later. MR imaging is usually normal, but contrast enhancement of the roots of the cauda equina occasionally occurs. The CSF is usually acellular, with a high protein concentration. Electromyoagraphy shows denervation with preserved sural action potentials. This is best regarded as a motor neuronopathy rather than a radiculopathy based on the neurophysiology.
Radiotherapy complications in the cranial nerves
Late-delayed complications of radiation therapy in the cranial nerves arise in fewer than 1% of cases after conventional radiotherapy (60 Gy in 2 Gy daily fractions). Having said that, patients who have previously received more than 50 Gy to the posterior fossa have a higher likelihood of developing hearing impairment. Current radiotherapy planning techniques allow for this risk to be minimised.
Optic nerve
The most clinically important cranial nerve implicated in delayed radiation toxicity is the optic nerve, which can be damaged many years after treatment for orbital, pituitary or suprasellar tumours. The optic nerve apparatus is regarded as a major organ at risk when planning treatment to nearby targets. Radiation therapy-induced optic neuropathy usually presents with subacute painless visual loss, progressing to monocular or binocular blindness with optic atrophy. Funduscopy of anterior lesions shows papilloedema and peripapillary haemorrhage, sometimes associated with radiation-induced retinal lesions, but is usually normal in posterior lesions. MR imaging of the anterior visual pathways with fat saturation can help in these cases, showing enlargement and signal change in the optic nerve and chiasm, with contrast enhancement.
As with late-delayed radiation myelopathy, steroids are useful in the acute setting, but there are no proven treatments for progressive optic neuropathy. Optic nerve sheath fenestration has been used in a few patients with some success.31
Eye movement disorder
Transient sixth nerve palsy occasionally follows radiation to the pituitary gland and cavernous sinus and very occasionally to the nasopharynx. Neuromyotonia may also occur, characterised by spontaneous eye muscle spasm and intermittent diplopia, usually lasting a few seconds, occurring up to several times an hour. This may respond to phenytoin or carbamazepine.
Trigeminal nerve
Facial numbness due to trigeminal neuropathy has been reported after radiosurgery for trigeminal neuralgia, trigeminal and vestibular schwannomas.
Facial nerve
Patients irradiated for head and neck cancer commonly report ageusia. Facial motor neuropathy almost never develops after fractionated radiation therapy and its development should prompt suspicion of perineural invasion. Facial palsy follows stereotactic radiosurgery for vestibular schwannoma in fewer than 5% of cases.
Vestibulocochlear nerve
Early–delayed hearing loss is usually due to otitis media, caused by oedema of the eustachian tube and temporary build-up of fluid within the middle ear. In contrast, late-onset hearing loss due to cochlear damage is characterised by high-frequency hearing loss and tinnitus.
Lower cranial nerves
The glossopharyngeal, vagus, spinal accessory and hypoglossal nerves can all be damaged by large radiation doses for head and neck cancer; this damage typically arises months to years after treatment. The hypoglossal nerve is the most commonly involved nerve presenting with unilateral asymptomatic or bilateral disabling paralysis with tongue atrophy. Unilateral vocal cord and palatal palsy give rise to dysarthria and dysphagia. Spinal accessory nerve palsy presents as painless shoulder drop.
Dropped head syndrome may occur as a potential late-delayed complication of radiation therapy due to weakness of the neck extensors several years after irradiation involving the cervical region, for example, mantle radiation therapy for Hodgkin’s disease. The differential diagnoses include myasthenia gravis, motor neurone disease or isolated neck extensor myopathy. Such extensive radiotherapy fields are much less commonly used today.
Radiotherapy complications in the peripheral nerves
Plexopathy
Brachial and lumbosacral plexopathies are the most important late-delayed complications of radiation therapy in the peripheral nervous system but are rarely seen nowadays, with the use of smaller doses and a greater awareness of the long-term effects of radiation. Brachial plexopathy is the more common and occurs after radiation therapy to the supraclavicular, infraclavicular or axillary nodes, usually for breast cancer and sometimes Hodgkin’s disease. Lumbosacral plexopathy much less commonly develops after radiation therapy for pelvic or lower abdominal and pelvic cancer (uterus, ovary, cervix, testis, rectum or prostate).
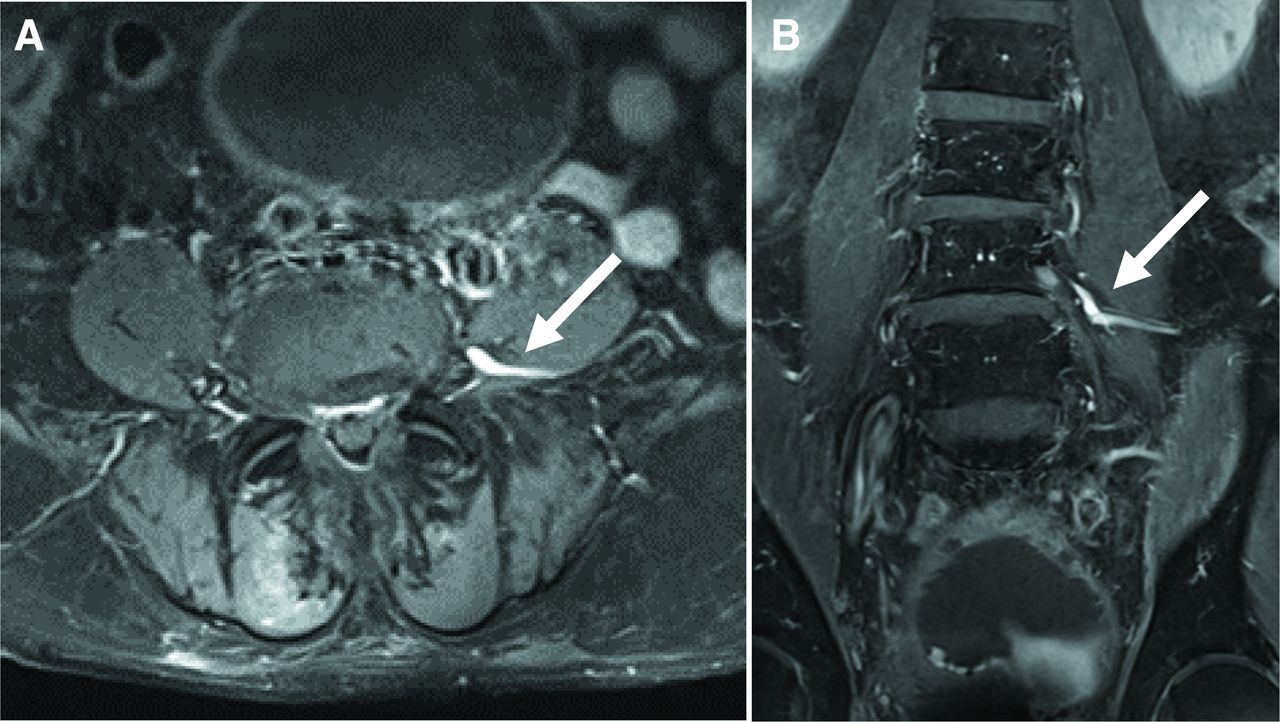
Occasionally, patients can present with an early–delayed plexopathy within a year of treatment, which usually improve within a few months, thought to be due to direct radiation toxicity on the Schwann cells inducing demyelination. This responds to corticosteroids (figure 8).

Early-delayed lumbosacral plexopathy. A 73-year-old man with subacute distal lower limb oedema, bilateral foot drop and loss of distal sensation, 4 months after completing radical radiotherapy for prostate cancer. EMG suggested a lumbosacral plexopathy rather than a sensorimotor neuropathy. Motor function improved completely with corticosteroids although a year later, there was persistent sensory impairment distally. Axial (A) and coronal (B) T1W post-gadolinium scans of lumbosacral spine showing diffuse contrast enhancement in the proximal L5 nerves, particularly on the left (arrow), in the lumbosacral plexus and the proximal S1 roots, again more on the left consistent with an early-delayed lumbosacral plexopathy. EMG, electromyography.
Late-delayed radiation plexopathies appear 3–20 years after treatment. As with other radiation therapy toxicity, the most important risk factors are the total radiation dose (>60 Gy) and dose per fraction (>2 Gy), the use of overlapping fields and combined chemoradiotherapy. There are two phases in the pathophysiology: during the first phase, direct radiation damage to the nerves causes acute inflammation that then resolves; later on, there is injury to the small arterioles and perineural fibrosis accounting for the severe and irreversible nerve damage.
Initial symptoms include distal paraesthesiae and dysaesthesiae, muscle weakness and atrophy confined to specific myotomes, dermatomal sensory loss and early loss of reflexes. The lack of pain and presence of myokymia, when present, strongly suggest the diagnosis and help to differentiate from malignant infiltration of the plexus. There may also be visible skin complications such as radiation dermatitis, painful induration of the axillary region and/or lymphoedema. During the later stages, there is progressive motor loss that can vary from localised muscle weakness to an almost complete paralysis of the limb.
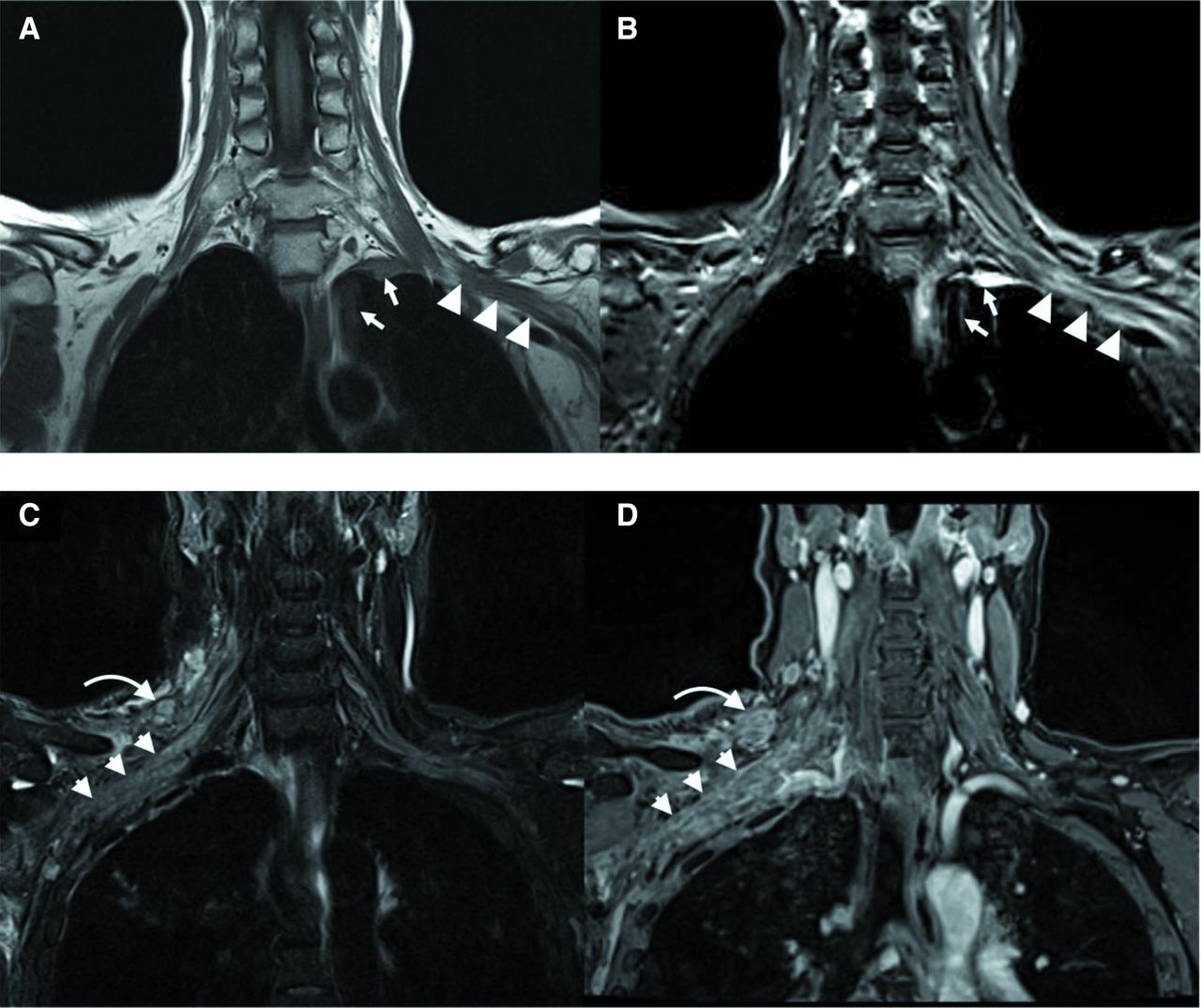
Neurophysiology shows normal motor and sensory conduction velocities. F waves may be absent or delayed. Electromyography shows fasciculation, fibrillations and positive sharp waves. The most important neurophysiological finding that favours radiation-induced plexopathy is the presence of myokymic discharges, present in about two-thirds of patients, but this almost never occurs with tumour infiltration. MR scanning is the imaging modality of choice in differentiating between radiation fibrosis—in which there is thickening of the brachial plexus with occasional contrast enhancement—and tumour infiltration, in which there are nodular mass lesions along the branches of the brachial plexus (figure 9). Rarely, MR imaging is inconclusive, and a biopsy may be indicated. In radiation plexopathy, this shows fibrosis and the absence of tumour infiltration.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Radiotherapy-related plexus changes versus malignant infiltration (Upper part)—radiation plexopathy. MR images of the brachial plexus (coronal T1W (A) and STIR (B)) showing STIR hyperintense signal changes predominantly involving the divisions and cords of the left brachial plexus with mild associated distortion and loss of the perineural fat planes (arrowheads). Note the pleural thickening and adjacent parenchymal scarring within the left lung apex (short arrows) secondary to previous radiotherapy. (Lower part) Malignant infiltration. MR images of the brachial plexus (coronal STIR (C) and fat-suppressed post-contrast T1w (D)) showing nodular thickening and enhancement of the right brachial plexus (arrowheads) and adjacent supraclavicular lymphadenopathy (curved arrow) consistent with metastatic infiltration in a patient with known breast carcinoma. (Courtesy of Dr Sachit Shah, Consultant Neuroradiologist, National Hospital for Neurology and Neurosurgery.) STIR, short inversion time inversion recovery.
The treatment is supportive involving physiotherapy, lymphoedema massage and bandaging and pain management.
Radiation-induced malignant peripheral nerve sheath tumours
Radiation-induced nerve malignant peripheral nerve sheath tumours can develop 4–40 years after radiation therapy, particularly in patients with neurofibromatosis type 1. Patients report localised pain followed by sensorimotor deficit, and diagnosis is made on imaging. Treatment is surgical with complete resection of the tumour. The prognosis of malignant peripheral nerve sheath tumours that result from radiation therapy is worse than those that develop de novo.32
Conclusion
Neurologists should be aware of the many early and delayed manifestations of radiation therapy neurotoxicity, as patients may present both to acute neurology and stroke services and to neurology outpatient clinics. However, radiation-induced neurotoxicity should be diagnosed only if the anatomical region lies within the radiation portal and is biologically consistent with what is known about the mechanisms and timing of radiation damage. Treatment options are limited for these complications and, therefore, it is essential (for patients’ quality of life) for clinicians to be aware of treatment modalities in other areas of neurology such as neurodegeneration.
Further reading
Wilke C, Grosshans D, Duman J, et al. Radiation-induced cognitive toxicity: pathophysiology and interventions to reduce toxicity in adults. Neuro-Oncology. 2017;20(5):597–607.
Dominguez M, Malani R. Stroke-like migraine attacks after radiation therapy (SMART) Syndrome: a comprehensive review. Curr Pain Headache Rep 2021; 25:33.
Kraik SF, Watson GA, Shih S-F, et al. Radiation-induced large vessel cerebral vasculopathy in pediatric patients with brain tumors treated with proton radiation therapy. Int J Radiat Oncol Biol Phys 2017;99:817–24
Key points
Radiation therapy for brain and spinal tumours is most commonly delivered as photons in the form of X-rays or gamma rays; proton beam therapy is used mainly for tumours in children to minimise long-term toxicity, and in adults for radioresistant tumours that require very high doses but adjacent to critical structures.
Precise dosimetry and treatment planning enable clear delineation of tumour treatment targets from organs at risk, to minimise collateral normal tissue damage.
Radiation toxicity in the brain, spinal cord or plexus can develop acutely but more commonly manifests shortly after completing radiation therapy (early delayed) and is usually reversible; in contrast, late-delayed radiation therapy toxicity is usually irreversible and presents with progressive neuronal loss, leukoencephalopathy and accelerated vasculopathy.
Neurologists may encounter acute presentations of radiation therapy toxicity months or years after completion of radiation therapy, including as stroke-like migraine attacks after radiation therapy (SMART) syndrome or radiation vasculopathy, presenting as a stroke-like episode, subacute myelopathy and delayed cognitive decline.
Second tumours can develop decades after radiation therapy in adult survivors of childhood tumours.
Data availability statement
No data are available.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
We thank Prof Yael Mardor, Sheba Medical Centre, Tel Aviv for supplying figure 3 and Dr Sachit Shah, Consultant neuroradiologist, NHNN for supplying figure 9.
References
Footnotes
Contributors MK contributed the section on Mechanisms of radiation damage, treatment planning and dose fractionation; JR designed the concept of the paper, wrote the section on radiation complications, key points, figures and legends and subsequent revisions.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Provenance and peer review. Commissioned. Externally peer reviewed by Robin Grant, Edinburgh, UK and Fiona McKevitt, Sheffield, UK.
Linked Articles
- Highlights from this issue
Other content recommended for you
- Malignant transformation and new primary tumours after therapeutic radiation for benign disease: substantial risks in certain tumour prone syndromes
- The neurofibromatoses
- Malignant peripheral nerve sheath tumour arising in the submandibular gland
- Further evidence of the increased risk for malignant peripheral nerve sheath tumour from a Scottish cohort of patients with neurofibromatosis type 1
- Radiation-induced optic neuropathy: a review
- Malignant peripheral nerve sheath tumours in neurofibromatosis 1
- Neurofibromatosis type 2
- Neurofibromatosis type 1: from genotype to phenotype
- Neuro-oncology
- Neurofibromatosis type 1 mosaicism in patients with constitutional mismatch repair deficiency