Article Text

Abstract
Idiopathic normal pressure hydrocephalus (NPH) was described in 1965 as a syndrome in which hydrocephalus develops but with a normal cerebrospinal fluid (CSF) pressure, causing shunt-responsive gait apraxia, cognitive impairment and urinary incontinence. Not all patients respond to shunting despite having the clinical syndrome with appropriate radiological features. This has led to considerable debate over subsequent decades regarding idiopathic NPH. It is now understood that asymptomatic communicating hydrocephalus can develop in many healthy older people, and that over time this can develop into a symptomatic state that sometimes responds to CSF shunting, but to a variable extent. This review looks at the historical background of NPH, the use of predictive tests, the current state of clinical evidence for the diagnosis and treatment of idiopathic NPH and the possible underlying causes, to provide a contemporary practical guide for assessing patients with the radiological features of idiopathic NPH.
- GAIT
- COGNITION
- DEMENTIA
- MOVEMENT DISORDERS
Data availability statement
Data are available upon reasonable request. Not applicable.
Statistics from Altmetric.com
The birth of a contentious syndrome
In 1965, Hakim and Adams (Massachusetts General Hospital) described normal pressure hydrocephalus.1 They reported three patients with cognitive impairment, gait apraxia and urinary incontinence (Hakim’s triad) who each had communicating hydrocephalus on pneumoencephalography and a normal cerebrospinal fluid (CSF) pressure. All three were relatively young (aged 16, 42 and 53 years)1 and each had a cause for their hydrocephalus: two followed a traumatic brain injury and one had a low-grade lymphocytic process. The patients sometimes declined after pneumoencephalography, an investigation where gas (eg, air or oxygen) was infused into the subarachnoid space using a spinal needle, making the ventricles and subarachnoid spaces visible on skull X-ray.2 All three patients dramatically improved after ventriculoatrial shunting.1 Hakim and Adams hypothesised that an initial increase in CSF pressure led to ventricular enlargement until an equal and opposite pressure was exerted between the ventricles and adjacent brain matter and the CSF pressure relatively normalised (figure 1). A further increase in CSF pressure decompensated this balanced state leading to the Hakim’s triad of symptoms, which could be improved by diverting CSF to an area of lower pressure (CSF shunting).1

Reproduced with permission from Elsevier.
In the same year, Hakim and Adams published another paper describing idiopathic NPH. They reported three slightly older (63, 66 and 62 years old) people with no apparent underlying cause.3 These patients had the Hakim symptom triad but did not always improve after lumbar puncture. They usually declined with pneumoencephalography and all dramatically improved after CSF shunting.3 Importantly, the index case declined after a fall when her ventriculoatrial shunt fractured but then improved after shunt repair, demonstrating an ongoing shunt-dependent condition.3
Not everyone is shunt responsive
Hakim and Adams’ original report of idiopathic NPH was a proof-of-concept paper representing their ‘most striking’ cases. However, when the wider neurological community treated larger numbers, although some responded dramatically to shunting, many showed only modest improvement, and others (up to half in some series) did not respond.3–8 Those who did respond usually had prominent gait disturbance, with all three symptoms of Hakim’s triad, and clinically they declined after pneumoencephalography, which showed a ‘lack of filling of the subarachnoid spaces over the cerebral convexity’. Invariably those with secondary causes of NPH more frequently responded to shunting.4–6 However, there were no reliable and specific radiological findings that identified people who were ‘shunt responsive’.4 5 Isotope brain scanning (scintigraphy) with intrathecal radiolabelled iodine revealed the presence of the tracer in the ventricles in patients with communicating hydrocephalus (but not in controls), and ventricular clearance over time was slow, suggesting obstruction to CSF resorption.7 While this technique was less hazardous than pneumoencephalography, it still could not predict ‘shunt responsiveness’ reliably.4 6 8 9
There were usually high complication rates during investigation and treatment (~30%–40%) with many early series having a significant postoperative mortality of ~7%.4 10–12 Computed tomography (CT) imaging became available in the early 1970s and superseded pneumoencephalography, providing a non-invasive way of showing communicating hydrocephalus (and the cortical atrophy caused by neurodegenerative disease).4 13 Intracranial pressure monitoring in patients with idiopathic NPH who responded to shunting confirmed Hakim and Adam’s hypothesis that CSF pressure was transiently raised in this condition, with abnormal pressure ‘B’ waves. However, even when using both CT imaging and intracranial pressure monitoring to investigate idiopathic NPH, not all patients responded to therapy.14
Some authorities suggested that patients with typical clinical and imaging findings who did not respond to shunting must have had the intervention too late to avoid irreversible disease.14 Others proposed that idiopathic NPH copresents with neurodegenerative disease and those in whom the ‘hydraulic’ component was prominent would respond to shunting, but those with neurodegeneration would not11; Jacobs noted that some cases had both Parkinson’s disease and idiopathic NPH and postulated that these two disease processes interacted, such that idiopathic NPH ‘precipitated or accelerated’ the parkinsonism; shunting could improve the gait, continence and cognition, but patients still needed levodopa to treat the parkinsonism.8
Provocative testing
Pneumoencephalography was used as both a diagnostic and a provocative test; after it went out of use several groups looked for less invasive provocative tests. Katzman and Hussey described the lumbar infusion study, in which fluid is infused into the lumbar CSF space while the pressure is measured at another lumbar level, thus allowing the measurement of ‘CSF absorption’.15 16 Børgesen and Gjerris used this technique in patients with NPH to measure the compliance of the CSF space and showed that those with increased resistance to a lumbar infusion of Ringer’s solution were usually shunt responsive.17
Some patients with idiopathic NPH improved after lumbar puncture. Thus, Wikkelsø et al. developed the CSF tap test, which involves standardised assessments of gait and cognition before and after a large volume (40 mL) lumbar puncture. They showed that this test could identify a population of shunt-responsive idiopathic NPH cases.18 However, not all shunt-responsive patients have a positive tap test. This led to the development of the external lumbar drain test, which resembles a CSF tap test except patients had a larger volume of CSF removed via a lumbar drain over a fixed period (usually a few days).19–21
Several well-designed clinical studies have compared these provocative CSF tests. Kahlon et al performed either the lumbar infusion study or the CSF tap test consecutively in 68 suspected NPH cases (primary and secondary) and gave a definitive CSF shunt to anyone positive for either test.22 Overall, 7 were positive for both tests and 81% improved at 6 months: 84% of these had positive lumbar infusion study but only 42% had a positive CSF tap test. Those with a positive CSF tap test were almost always shunt responsive (positive predictive value 94%); the lumbar infusion study had a positive predictive value of 80% but was more sensitive. Unexpectedly, 5 of 21 (24%) non-shunted cases improved at 6 months (2 had prior traumatic brain injury and 1 had aneurysmal subarachnoid haemorrhage) and at follow-up there were no differences between shunted and non-shunted people on gait or cognitive measures. Reassuringly provocative testing caused no complications, but three patients developed a subdural collection and one developed meningitis following ventriculoperitoneal shunting (8.5% complication rate).
Walchenbach undertook a CSF tap test on 49 NPH patients; all non-responders then had an external lumbar drain and all patients (regardless of response) had definitive CSF shunting.23 This experimental design allowed sensitivity and specificity calculations for each test although there was no non-shunted control group to assess shunt efficacy. As in Kahlon et al.’s study, CSF tap test was not very sensitive (26%) but was highly specific (100%). Meanwhile, an external lumbar drain had benefit similar to a lumbar infusion study, with a sensitivity of 50% and good specificity 80%. Once again, an external lumbar drain was associated with complications, with bacterial meningitis occurring in 4%. Subdural haemorrhage occasionally followed shunt surgery but the authors did not report its frequency.
Meta-analyses have subsequently confirmed that the CSF tap test has a high positive predictive value and that external lumbar drainage also has a high specificity (~85% with wide confidence intervals) but there is no perfect predictive test for shunt responsiveness.24 25
An existential crisis
Postmortem findings of patients with shunt-responsive NPH commonly show meningeal fibrosis and deep white matter microvascular changes but with no unique or pathognomonic features.26–28 NPH was an unusual syndrome in which a response to the proposed treatment was also the primary diagnostic criterion. By the early 21st century, there was still no explanation for the lack of a consistent response to CSF shunting. Some meta-analyses of the available evidence showed CSF shunting had a positive effect but systematic reviews of randomised, controlled studies found no evidence to support CSF shunting in NPH.29–31 Some clinicians questioned the existence of NPH at all, and the field became radically polarised to ‘believers’ and ‘non-believers’.32
Clinical guidelines
Around 20 years ago, two groups produced clinical guidelines for the diagnosis and classification of idiopathic NPH that are still used today. Ishakawa’s 2004 Japanese Hydrocephalus Society guidelines classified patients as having ‘possible idiopathic NPH’ if they were >60 years of age with imaging features of hydrocephalus and at least two of Hakim’s symptom triad, and with no alternative explanation for their symptoms.33 Patients with a normal lumbar puncture opening pressure and a response either to CSF tap test, external lumbar drain or lumbar infusion study, are classified as ‘probable idiopathic NPH’. Those who respond to surgery are classified as ‘definite idiopathic NPH’. Relkin et al published joint American, German and Swedish guidelines in 2005 and defined ‘probable’ idiopathic NPH strictly as occurring in people aged over 40 years who have all three of Hakim’s triad with hydrocephalus on imaging and a normal CSF opening pressure.34 The Relkin criteria for ‘possible idiopathic NPH’ are more permissive, including patients with isolated gait disorder or cognitive decline if they have imaging findings of ventriculomegaly. Relkin et al were not prescriptive about the use of provocative tests but noted that those with ‘probable idiopathic NPH’ were likely to have positive predictive tests, further increasing the likelihood of a positive response to shunt.34 The Japanese Hydrocephalus Society updated their guidelines in 2021 to allow for those with more specific radiological and gait criteria to be considered ‘probable’ idiopathic NPH without needing affirmative provocative testing.35 Both sets of guidelines acknowledge the lack of prospective evidence on which to base guidance.
NPH has a specific radiological identity
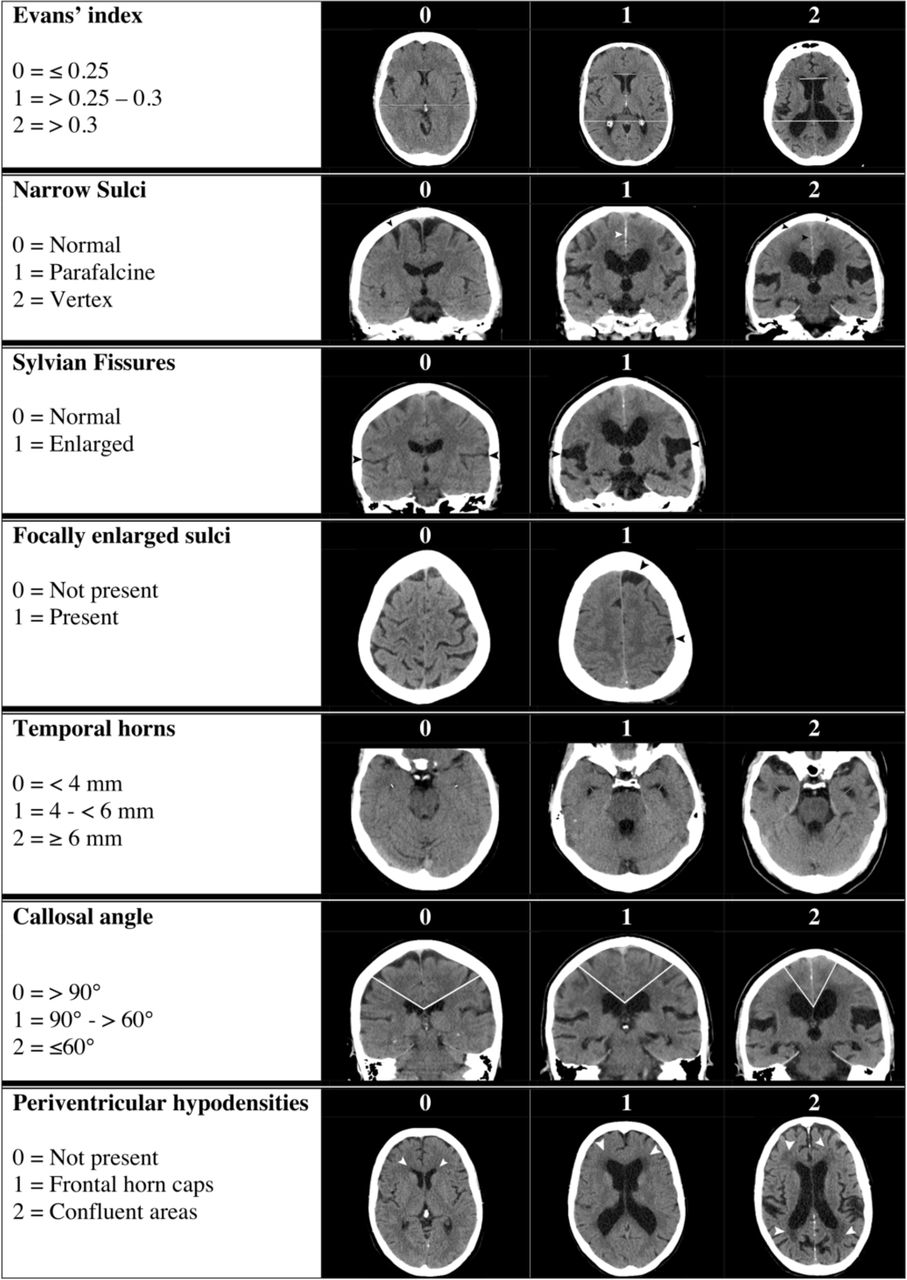
Hakim and Adams observed that patients with a tight callosal angle on pneumoencephalography usually responded to shunting.5 When CT scanning superseded pneumoencephalography, the Evans' index (ratio of the widest width of the frontal ventricles to the widest width of the brain on an axial plane) of >0.3 was used as a surrogate.33 34 However, we now know that 20% of those aged over 70 years have a raised Evans’ index.36 More specific features of hydrocephalus have since been described: specifically, disproportionate enlargement of the subarachnoid space hydrocephalus (DESH) and a callosal angle below 90°.37 Many of these features form the ‘probable idiopathic NPH’ criteria for the Relkin NPH guidelines. Practically, the updated Japanese Hydrocephalus Society guidelines allow a DESH pattern with a higher-level gait pattern (locomotor and balance difficulties that cannot be explained by peripheral motor, sensory, pyramidal, cerebellar, or basal ganglia lesions) to qualify as ‘probable NPH’ without an external lumbar drain or lumbar infusion study.34 35 38 Further, Kockum et al developed a grading scale—‘The idiopathic NPH Radscale Score’—by ‘weighing’ the importance of its specific radiological features39 (figure 2), and found that a score of>4 distinguished patients with shunt-responsive idiopathic NPH from their age-matched controls.40

The idiopathic normal pressure hydrocephalus (NPH) Radscale Score Atlas showing the different imaging features of hydrocephalus. A combined score of >4 differentiates shunt-responsive idiopathic NPH cases from normal controls. Reproduced with permission from Kockum et al.40
‘No placebos, please’: clinical trial evidence
Patients with idiopathic NPH may be reluctant to enrol into clinical trials in which they might not receive shunt therapy. In 2011, Tisell et al sidestepped this problem by using a ‘one-arm crossover’ trial design in which all patients received CSF shunts but only half had these activated on insertion41; all patients had an operation (or sham) halfway through the study and those whose shunts had initially been tied closed had them opened, so all patients ended the trial with active shunts. The trial was double blinded and neither assessors nor patients knew their shunt activation status until the final intervention. Although this trial was a small study of a specific population who had severe vascular disease and idiopathic NPH unresponsive to a CSF tap test, the design is now the gold-standard in clinical trials for this condition.42 In 2015, Kazui et al used a similar design in SINPHONI-2, a prospective, randomised control trial of immediate vs delayed lumboperitoneal shunt in probable idiopathic NPH. They found that lumboperitoneal shunts modestly reduced disability, cognitive and gait impairment.43 Toma and Watkins performed a prospective randomised, double-blind one-arm cross-over trial with programmable ventriculoperitoneal shunts in probable idiopathic NPH. This trial was ended due to incomplete enrolment; the full dataset has not been published but a brief report on a sample size of only 14 patients showed an improved primary outcome (gait speed) at 3 months after the shunt.44 Two further prospective, double-blinded randomised controlled trials in the USA using ventriculoperitoneal shunts and a ‘one-arm crossover’ trial design, the ARCS-NPH and the PENS feasibility study, have completed but the results are not yet published.45 46 A larger scale version of PENS is due to recruit in the USA in 2022.47 A Cochrane systematic review is currently evaluating the pooled analysis of these studies.48 A limitation of the ‘one-arm crossover’ trial design is that it sacrifices outcome data from the long-term control arm. Large-scale prospective follow-up data for shunted patients suggest that the benefit of ventriculperitoneal shunting persists for years before decline.49 50 While complication rates remain relatively high at 20–30%, most are now managed non-surgically.43 49 51
What causes idiopathic NPH?
There have been several plausible disease mechanisms proposed for NPH, including direct cortical mass effect, reduced CSF absorption, reduce periventricular blood flow and reduced glymphatic clearance.7 52–54 However, the underlying cause of the hydrocephalus remains uncertain, although genetic cases may hold a clue. Several family pedigrees have been described with inherited idiopathic NPH .55–57 In 2019, Morimoto et al identified a CFAP43 mutation in a Japanese kindred with autosomal dominant hydrocephalus.58 cfap43 knockout mice have a hydrocephalic phenotype; mutations in this protein appear to cause primary ciliary dyskinesia.58 Subsequently, Yang et al have identified CWH34 mutations in 15% of a non-familial idiopathic NPH cohort.59 CWH43 is a glycosylphosphatidylinositol anchor protein expressed in the ventricular epithelia, and CWH43 mutation knock-in mice have reduced ventricular cilial density and function, providing further evidence that cilial function may be linked to the development of hydrocephalus. SFMBT1 is a protein of uncertain function that is expressed in the choroid; patients with idiopathic NPH (several cohorts) have a higher rate (10–26%) of heterozygous copy number loss in SFMBT1 than age matched controls (4–5%).60 61 Although multiple genetic factors influence the development of hydrocephalus, there are also environmental associations. For example, prospective studies have shown that 90% of people with idiopathic NPH have obstructive sleep apnoea, and the prevalence of idiopathic NPH is much higher in people with schizophrenia and diabetes than in age-matched controls.62–64
Idiopathic NPH and the role of ageing and neurodegenerative disease
Prospective screening population studies suggest that up to 6% of people aged over 65 years fulfil clinical and radiological criteria for possible idiopathic NPH, and that this percentage increases with age.65 There are also reports of asymptomatic patients with radiological features of idiopathic NPH. With long-term follow-up, many become symptomatic, consistent with Hakim and Adams' original hypothesis that hydrocephalus develops asymptomatically before causing clinical symptoms.66 Some people with asymptomatic hydrocephalus probably develop Hakim’s triad from underlying neurodegenerative disease that is not shunt-responsive. In particular, patients with progressive supranuclear palsy develop imaging features of hydrocephalus more than those with Parkinson’s disease, Alzheimer’s dementia or normal controls.67 The few available postmortem studies in idiopathic NPH show that many cases have Alzheimer’s dementia or vascular pathology at time of death but progressive supranuclear palsy pathology occurs more frequently than expected.28 68–70 Frontal or parietal cortical biopsies taken at the time of ventriculoperitoneal shunt insertion or intracranial pressure monitoring show that Alzheimer’s dementia develops in 30%–60% of cases; there are contrasting reports about whether this influences the effect of CSF shunting.71–73 Recent studies suggest that patients with low CSF neurofilament light, total tau, abeta 1–40 and pTau181 are more likely to respond to shunting. It may be that people with higher markers of neurodegeneration have asymptomatic hydrocephalus and an underlying neurodegenerative disease.74 75
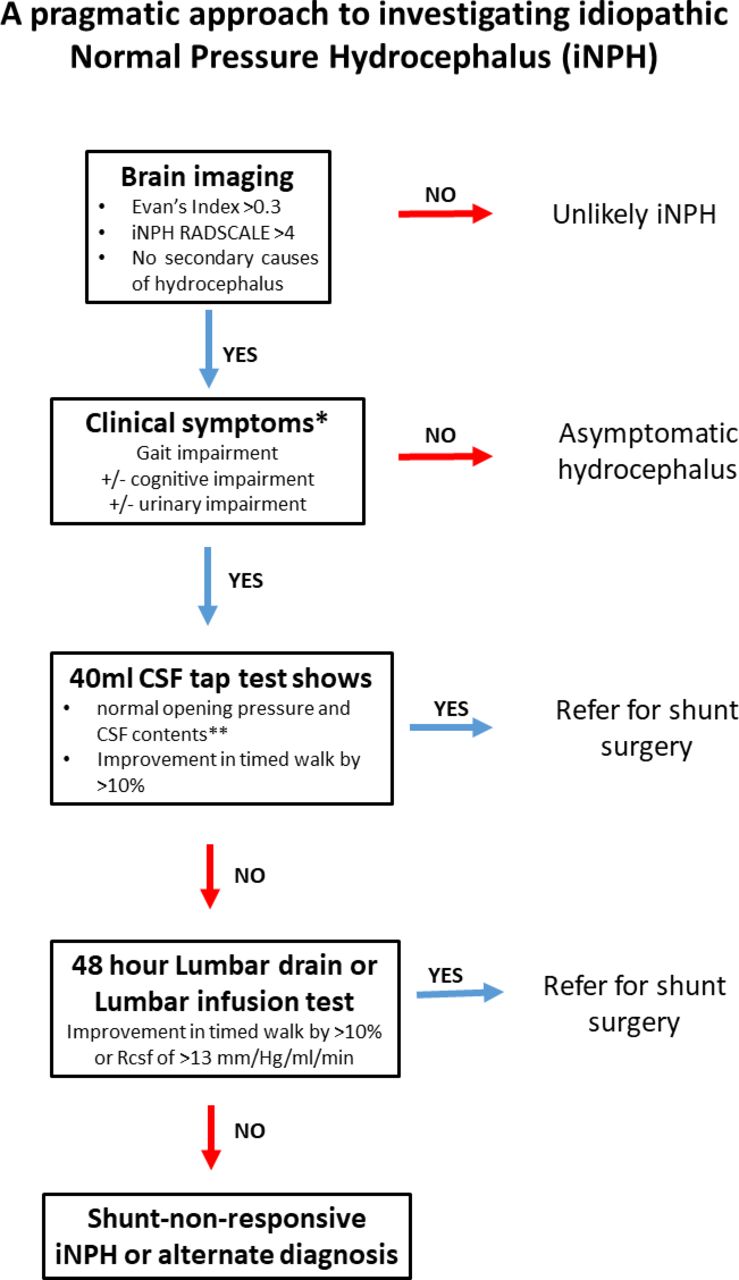
A pragmatic approach to assessing idiopathic NPH
Large case series have shown that many patients presenting with idiopathic NPH have an alternative cause for their symptoms.76 In a large prospective US idiopathic NPH register, 26% of cases did not undergo provocative testing and 46% of patients had shunted surgery.77 Thus, a careful neurological history and examination is required to exclude NPH mimics and alternative explanation for patient symptoms.
At the NPH clinic in Imperial College Hospital, London, we accept the limitations of the current evidence and follow the Japanese Hydrocephalus Society and Relkin guidance, broadly incorporating idiopathic NPH Radscale imaging scores. Multidisciplinary working with neurologists, neuroradiologists, neurotherapists and neurosurgeons is key. It is important to note that the investigation and treatment of idiopathic NPH is highly invasive. We are explicit about this in initial discussions with the patient and family so they can make an informed decision about proceeding. Equally it may not be appropriate to perform invasive testing or shunt surgery on frail patients with multiple co-morbidities and this must be considered at the early stages of the assessment. We do not usually consider a diagnosis of idiopathic NPH if the idiopathic NPH Radscale Score is <4 (figure 3). Patients with imaging features of idiopathic NPH referred to our neurology-led clinic are assessed clinically and with subsequent discussion of their imaging in a specialist dementia neuroradiology multidisciplinary team meeting.78 Patients may then have dopamine transporter (DaT), single-photon emission CT (SPECT), amyloid positron-emission tomography (PET) and fluorodeoxyglucose (FDG)-PET imaging as indicated on a case-by-case basis. We do not investigate asymptomatic patients further but counsel them to return if they develop Hakim’s triad symptoms (figure 4). If patients have a higher-order gait dysfunction with no other identified cause then they have a 40 mL CSF tap test with a therapist-led 10 m timed walk. The timed walk is performed in triplicate immediately before and at a minimum of 4 hours after the CSF tap test. Our experience suggests that some people’s triplicate values vary with fatigue effects, and so we compare the lowest values acquired. Out of interest, we screen cognition before and after the CSF tap test but do not require cognitive improvement to define shunt responsiveness, as cognition can to take many months to improve following definitive ventriculoperitoneal shunt surgery.50 It is important to note that the original 1982 Wikkelsø CSF tap test protocol showed that gait speed can improve up to a week following the test, but in our practice it is not possible to repeat carefully observed gait assessments over this period, so we instead consider subjective reports of improvements in the week following the CSF tap test.18 At the time of CSF tap test we also carry out neurodegenerative biomarker assessment including CSF neurofilament light. We refer patients who improve by >10% with a CSF tap test for CSF shunt surgery (figure 5). Those who do not improve are usually referred to the CSF-disorder neurosurgeons and have either an external lumbar drain or a lumbar infusion study. Those who improve with these tests have a ventriculoperitoneal shunt. Those who do not improve following a shunt are reviewed in the NPH clinic to reconsider diagnosis (figure 6). If patients have a clear neurodegenerative copathology but it is unclear if this is causing dominant gait apraxia we do investigate further with provocative testing, as this can tangibly infer the degree of potential improvement with shunt surgery (figure 7). We are cautious to advise shunt surgery in these cases without a positive predictive CSF test but we discuss the potential risks with the patient, their family, neurologist and neurosurgeons. Patients who do not improve after definitive ventriculoperitoneal shunt surgery are investigated by our CSF disorder neurosurgeons, who exclude surgical compications, ensure shunt patency and adjust shunt settings as appropriate. Shunt-unresponsive patients and those who develop recrudescence of Hakim’s triad are re-referred to the NPH clinic for further assessment.
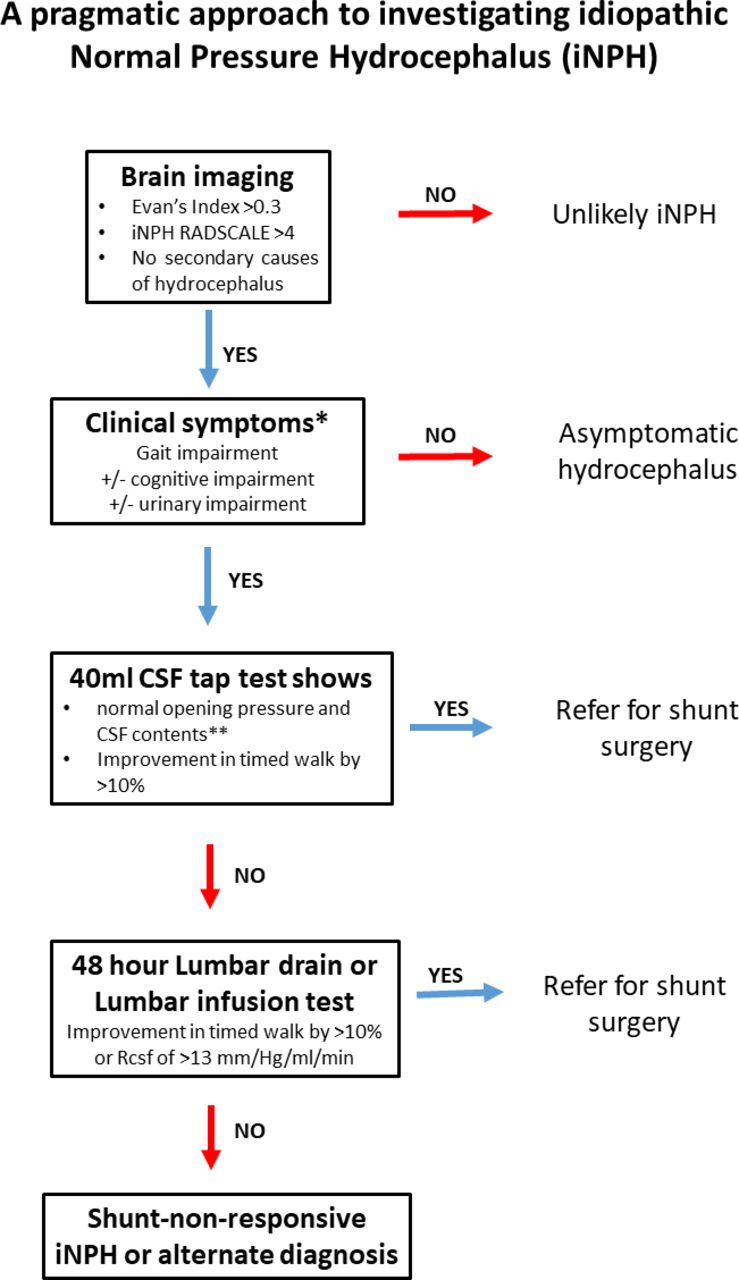
The investigation and management pathway of idiopathic NPH at Imperial College London Healthcare NHS Trust. **Not explained by another neurological condition, for example, PSP. **Patients with abnormal CSFcontencts and/or raised CSF neurofilament light should be further evaluated before further NPH provocative testing. CSF, cerebrospinal fluid; iNPH, idiopathic normal pressure hydrocephalus;, PSP progressive supranuclear palsy.

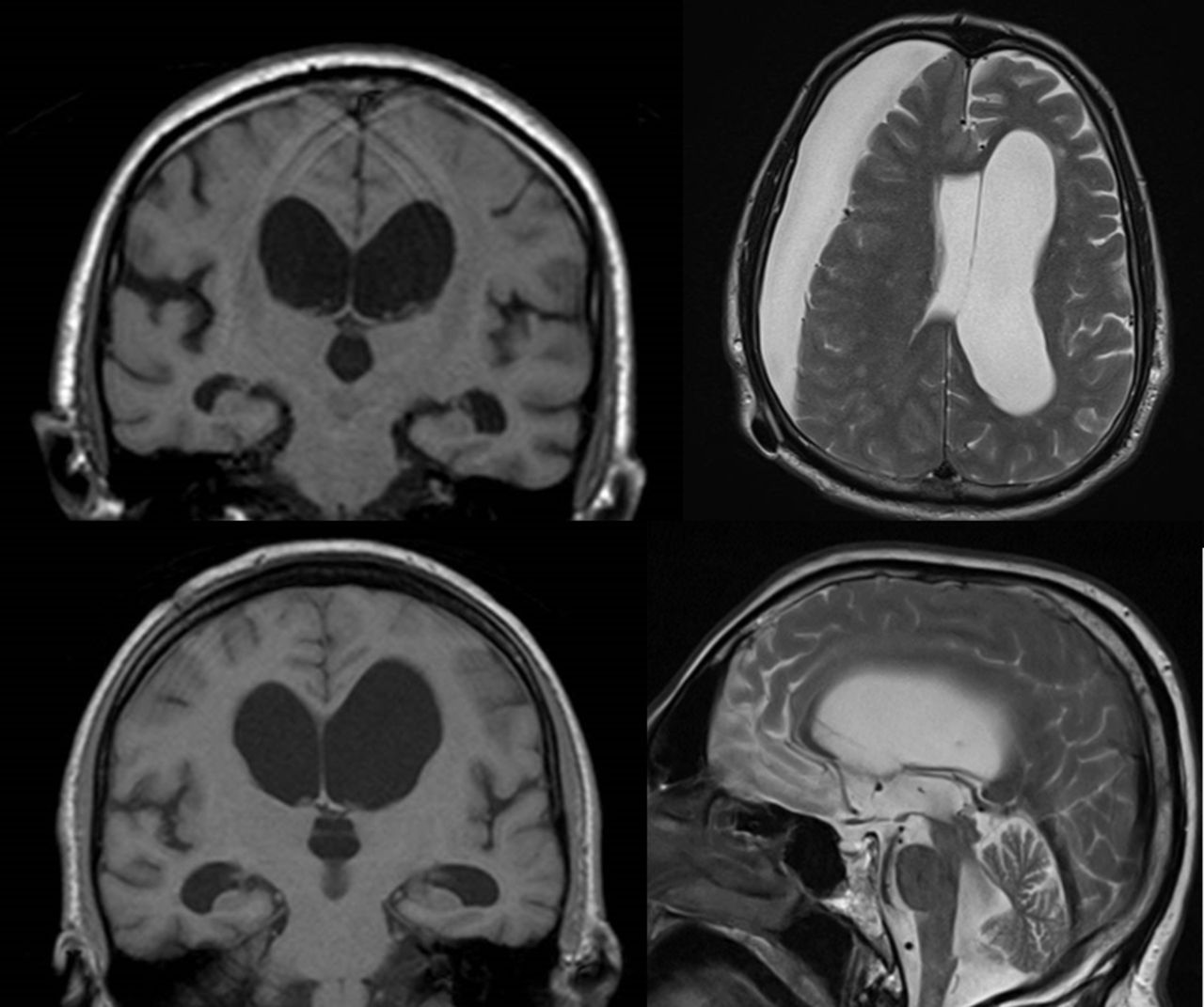
A 72-year-old woman presented to TIA clinic with a 5 min episode where she found it difficult to read and was mildly confused. She had a background of frequent migraine with visual aura but no traditional vascular risk factors. After investigations by TIA clinic, there was no clear diagnosis but she was referred to normal pressure hydrocephalus clinic regarding the relevance of her brain imaging. Clinically, she had no problems with gait and bedside cognitive testing was normal. She was discharged with an invitation to return if she developed relevant symptoms. TIA, tranient ischaemic attack.

A 60-year-old woman with a severe progressive gait impairment and imbalance was admitted to hospital unable to walk independently. She had bipolar disorder treated with antipsychotics since age 15 years. She also had urinary incontinence problems and previous pelvic floor surgery. She had attended the neurology clinic in 2014 with gait instability but MR scan of the brain and a dopamine transporter (DaT) scan were normal. Repeat MR of the brain imaging showed hydrocephalus. A cerebrospinal fluid tap test gave an opening pressure of 15 cm of water. Following the lumbar puncture, her 10 m walking time reduced from 1 min 42 s to 38 s, though her Montreal Cognitive Assessment remained unchanged at 15/30. Following ventriculo-peritoneal shunt insertion, her walking speed and stability improved dramatically. Two years later, she still has severe anxiety and subjective imbalance but she can walk independently with a stick and manages her household affairs independently. A repeat DaT scan was unchanged despite the 7-year interval.
A 69-year-old retired man had a 2-year history of cognitive impairment and slowed walking. His family felt that he has ‘lost his spark’. His MR scan of the brain showed communicating hydrocephalus and his DaT scan was negative. A CSF tap test improved his timed 10 m walk by 15.2%. Following a shunt procedure, he developed a large subdural haemorrhage that did not improve with conservative management or with shunt setting changes. After surgical evacuation of the subdural and a period of rehabilitation he could not transfer independently. He was referred to neurology at this stage and found to have abnormalities of phonemic fluency, tests of abstraction and Stroop testing. There was a vertical supranuclear palsy and upper limb ideomotor dyspraxia without increase in limb tone or bradykinesia. He was diagnosed with progressive supranuclear palsy and managed supportively.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A 77-year-old man with gait impairment was found to have hydrocephalus on imaging. Clinically, he had cognitive impairment with apathy and impaired executive function. Neurologically, he had a vertical supranuclear palsy. There was no clear bradykinesia or increase in tone but there was ideomotor dyspraxia of the upper limbs. He had a wide based, unsteady and slow gait with freezing and postural areflexia, which was disproportionate to his other symptoms. He fulfilled clinical criteria for progressive supranuclear palsy (PSP), but it was uncertain whether this completely explained his gait dysfunction. Cerebrospinal fluid tap-testing did not improve his walking speed and he was referred to cerebrospinal fluid disorder neurosurgeons who performed a 48-hour lumbar drain. This did not improve his condition when assessed by neurophysiotherapists. After mult-disciplinary discussion he was managed supportively for PSP.
Conclusions
Neurologists commonly encounter people with the syndrome of idiopathic NPH, which has specific radiological features and can be CSF shunt responsive. It is essential that such patients are assessed by clinicians with the experience to identify and manage NPH mimics and to perform standardised provocative tests to help to determine who will benefit from CSF shunting. There is little high-quality evidence on which to base practice and we need further work—including more randomised controlled trial evidence on the use of CSF shunting—to understand the cause and to characterise the radiological features associated with shunt-responsive idiopathic NPH. Going forward, we need to characterise patients with possible idiopathic NPH not just by the presence of vascular disease and amyloid status but also by synuclein, tau as well as non-specific markers of neuronal loss such as neurofilament light to understand the interaction between neurodegenerative disease and idiopathic NPH. Such an approach will need to be large scale, co-ordinated and collaborative. This approach will also open the door to potential disease-modifying trials in patients with shunt-unresponsive hydrocephalus who traditionally have been clinically neglected.
Further reading
Adams RD, Fisher CM, Hakim S, et al. Symptomatic occult hydrocephalus with 'normal' cerebrospinal-fluid pressure. A treatable syndrome. N Engl J Med 1965;273:117–26.
Kazui H, Miyajima M, Mori E, et al. Lumboperitoneal shunt surgery for idiopathic normal pressure hydrocephalus (SINPHONI-2): an open-label randomised trial. Lancet Neurol 2015;14(6):585–94.
Kockum K, Virhammar J, Riklund K, et al. Diagnostic accuracy of the iNPH Radscale in idiopathic normal pressure hydrocephalus. PloS One 2020;15(4):e0232275.
Kimihira L, Iseki C, Takahashi Y, et al. A multi-center, prospective study on the progression rate of asymptomatic ventriculomegaly with features of idiopathic normal pressure hydrocephalus on magnetic resonance imaging to idiopathic normal pressure hydrocephalus. J Neurol Sci 2020;419:117166.
Key points
Idiopathic normal pressure hydrocephalus (NPH) should be considered in patients who have dominant gait dysfunction with cognitive and urinary symptoms; there is some high-quality evidence to justify cerebrospinal fluid shunting in such cases.
Ventriculomegaly is a common and non-specific finding in elderly people but NPH has some specific radiological features.
The radiological features of NPH initially develop asymptomatically, so it is important to exclude alternative causes in patients whose symptoms suggest idiopathic NPH.
Data availability statement
Data are available upon reasonable request. Not applicable.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Acknowledgments
Thank you to Dr Paresh Malhotra for manuscript comments. Thank you to Elsevier for permission to republish figure 1 and to Dr Katrin Kockum for permission to republish figure 2.
References
Footnotes
Contributors CC conceived and wrote the article.
Funding The author has not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Provenance and peer review Commissioned; externally peer reviewed by Robin Corkill, Cardiff, UK, Anthony Jesurasa, Cardiff, UK, and Cath Mummery, London, UK.
Other content recommended for you
- Normal pressure hydrocephalus: long-term outcome after shunt surgery
- Magnetic resonance spectroscopic determination of a neuronal and axonal marker in white matter predicts reversibility of deficits in secondary normal pressure hydrocephalus
- Idiopathic normal-pressure hydrocephalus: clinical comorbidity correlated with cerebral biopsy findings and outcome of cerebrospinal fluid shunting
- Intracranial cerebrospinal fluid measurement studies in suspected idiopathic normal pressure hydrocephalus, secondary normal pressure hydrocephalus, and brain atrophy
- Idiopathic normal pressure hydrocephalus
- Incidence, diagnostic criteria and outcome following ventriculoperitoneal shunting of idiopathic normal pressure hydrocephalus in a memory clinic population: a prospective observational cross-sectional and cohort study
- Is normal pressure hydrocephalus a valid concept in 2002? A reappraisal in five questions and proposal for a new designation of the syndrome as “chronic hydrocephalus”
- Current epidemiology of cerebrospinal fluid shunt surgery in the UK and Ireland (2004–2013)
- Comparison between the lumbar infusion and CSF tap tests to predict outcome after shunt surgery in suspected normal pressure hydrocephalus
- Evidence that congenital hydrocephalus is a precursor to idiopathic normal pressure hydrocephalus in only a subset of patients