Article Text

Abstract
Background Cerebral venous sinus thrombosis (CVST) is an uncommon form of stroke that, when severe, can be a therapeutic challenge. Endovascular mechanical thrombectomy (EMT) techniques have significantly evolved over the past decade, but data regarding the efficacy and safety of EMT for CVST are poorly defined.
Objective To summarize the large number of case series on this relatively rare condition and establish trends in the outcomes of EMT for CVST.
Methods A literature review was performed using PubMed and Medline to identify reports of three or more patients with CVST treated with EMT. Baseline and outcomes data, including radiographic resolution, neurological outcome, recurrence, and treatment-related complications, were extracted for analysis.
Results A total of 17 studies comprising 235 patients treated with EMT were included for analysis. Based on pooled data, 40.2% of patients presented with encephalopathy or coma. Concurrent endovascular thrombolysis was employed in 87.6% of patients. Complete radiographic resolution of CVST was achieved in 69.0% of patients. At follow-up (range 0.5–3.5 years), 34.7% of patients were neurologically intact and the mortality rate was 14.3%. CVST recurrence was evident in 1.2%. Worsening or new intracranial hemorrhage (ICH) occurred in 8.7% of cases. ORs of good outcome (modified Rankin Scale score 0–2) and development of ICH with sole EMT versus concurrent thrombolytic therapy were 1.51 (95% CI 0.29 to 8.15, p=0.61) and 1.15 (95% CI 0.12 to 10.80, p=0.90), respectively.
Conclusions EMT is an effective salvage therapy for refractory CVST, with a reasonable safety profile. Chemical thrombolysis, in conjunction with EMT, did not appear to result in additional harm or benefit. Further analysis is warranted to determine predictors of success after EMT for CVST.
- Thrombectomy
- Intervention
- Vein
- Stroke
Statistics from Altmetric.com
Introduction
Cerebral venous sinus thrombosis (CVST) is an overall uncommon cause of venous cerebral infarction that accounts for approximately 0.5–1% of all strokes.1 Although low overall, the incidence of CVST is much higher in women taking oral contraceptives and in children.1 Management of symptomatic CVST remains a challenge.2 The initial treatment for CVST is systemic anticoagulation, which has been associated with improved neurological outcomes in small randomized studies.3 However, with anticoagulation alone, large and extensive thrombi are unlikely to dissolve, and thus approximately one-third of patients with severe presentation have a high risk of incomplete recovery.2 ,4 Endovascular intervention is an alternative option for patients with neurological deterioration despite the use of anticoagulation or with development of new or worsening intracerebral hemorrhage (ICH) on anticoagulation.5–13 Current endovascular techniques include direct catheter thrombolysis, balloon-assisted thrombectomy, rheolytic catheter thrombectomy, aspiration thrombectomy, and stent retriever thrombectomy.7 ,8 ,13 ,14 The variation in endovascular mechanical thrombectomy (EMT) techniques for CVST intervention has made a comprehensive assessment of its outcomes difficult. The aim of this systematic review is to summarize the inherently heterogeneous, large number of case series on this relatively rare condition to establish trends in the outcomes of EMT for CVST.
Methods
Literature search and inclusion criteria
This systematic review follows the guidelines set forth by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (figure 1). A literature review was performed using PubMed (September 10, 2016) and Medline (January 20, 2016), with the following search phrase: “venous thrombectomy AND sinus thrombosis AND intracranial”. The studies underwent screening by title and abstract to ascertain fulfillment of the inclusion criteria, which were as follows: (1) the number of patients with CVST treated with EMT must be reported; (2) each treated patient must be represented only once among all of the studies included for analysis; (3) the study must include three or more patients who had undergone EMT; (4) patients may be treated with any form of EMT, including direct catheter thrombolysis, balloon-assisted thrombectomy, rheolytic catheter thrombectomy, aspiration thrombectomy, or stent retriever thrombectomy; and (5) the study must be written in English. Studies with overlapping published data from the same institution in a more recent study were excluded.

Flow diagram showing the selection process for the studies included in the analyses of endovascular mechanical thrombectomy for cerebral venous sinus thrombosis.
Data extraction
Summary data and, when available, individual patient data regarding patient demographics, CVST characteristics, endovascular and adjuvant treatment details, and data on outcomes and complications were extracted from each study. Demographic data included the number of patients with CVST treated with EMT, gender, and age. CVST characteristics included risk factors, thrombus location, and presenting symptoms. Data on treatment details included type of EMT, use of preoperative anticoagulation, and use of adjuvant therapy. When appropriate, the size of stent retriever used was recorded. Outcome and complication data included degree of sinus recanalization at last follow-up, thrombus recurrences, periprocedural complications, degree of neurological deficit at last follow-up, and death. Neurological deficit was categorized as mild, moderate, or severe, which corresponded to a modified Rankin Scale (mRS) score of 1–2, 3–4, and 5, respectively. When the mRS score was not available, mild neurological deficit corresponded to an independently communicative and ambulatory patient with mild weakness; moderate deficit corresponded to a patient with impaired ambulation and moderate weakness; and severe deficit corresponded to a patient who required assistance in activities of daily living.15 ,16 A good outcome was defined as an mRS score of 0–2, whereas a poor outcome was defined as an mRS score of 3–5. Recurrence was defined as the presence of both clinical (new or relapse of previous symptoms) and radiologic evidence of re-thrombosis during follow-up after complete or partial recanalization.16 ,17
Statistical analysis
Descriptive statistics were calculated for baseline, treatment, and post-EMT outcomes data using Matlab (version R2016a, MathWorks). Meta-analysis of individual data was performed using RevMan (V.5.3, The Cochrane Collaboration). ORs were computed for each study with sufficient individual patient data to determine the association of good neurologic outcome (mRS 0–2) with demographic features, patient presentation, treatment characteristics, and complications. ORs were collectively analyzed for each association using the Mantel–Haenszel method. Statistical heterogeneity was examined with the I2 statistic. A random-effects model was used. The 95% CI was reported for each analysis. Two-tailed p values of <0.05 were considered significant.
Results
Study selection
The literature search yielded a total of 78 studies, of which 31 were excluded after review of abstracts. Of the remaining 47 studies, 17 met the inclusion criteria and were included in our analysis (figure 1). The reasons for exclusion of 30 studies after full-text article review included failure to report number of patients treated with EMT (N=6), duplication of patients treated with EMT (N=2), cohort size less than three patients (N=21), and failure to specify type of EMT used (N=1).
Demographics and CVST presentation
Patient demographics of the 17 studies that met our inclusion criteria, which comprised a total of 235 patients with CVST who were treated with EMT, are summarized in online supplementary table S1. Among those who underwent EMT, 62.9% (132/210 patients) were female. The median age ranged from 5 to 58 years. Acquired prothrombotic states, including pregnancy, puerperium, and nephrotic syndrome, were identified as CVST risk factors in 23% of cases; infection was identified in 17% of cases; hematologic causes, including polycythemia, severe anemia, and history of deep vein thrombosis, were identified in 16% of cases; oral contraceptive use was identified in 6% of cases; smoking was identified in 2% of cases; genetic prothrombotic states including factor V Leiden mutation and mutations leading to homocysteinemia were identified in 6% of cases; malignancy was identified in 5% of cases; mechanical causes, including head trauma and neurosurgical procedures, were identified in 5% of cases; inflammatory and autoimmune diseases, including ulcerative colitis and Sjögren's syndrome were identified in 4% of cases; and other causes, including severe dehydration and congenital heart disease, were identified in 7% of cases. No identifiable risk factor was found in 20% of the patients.
supplementary tables
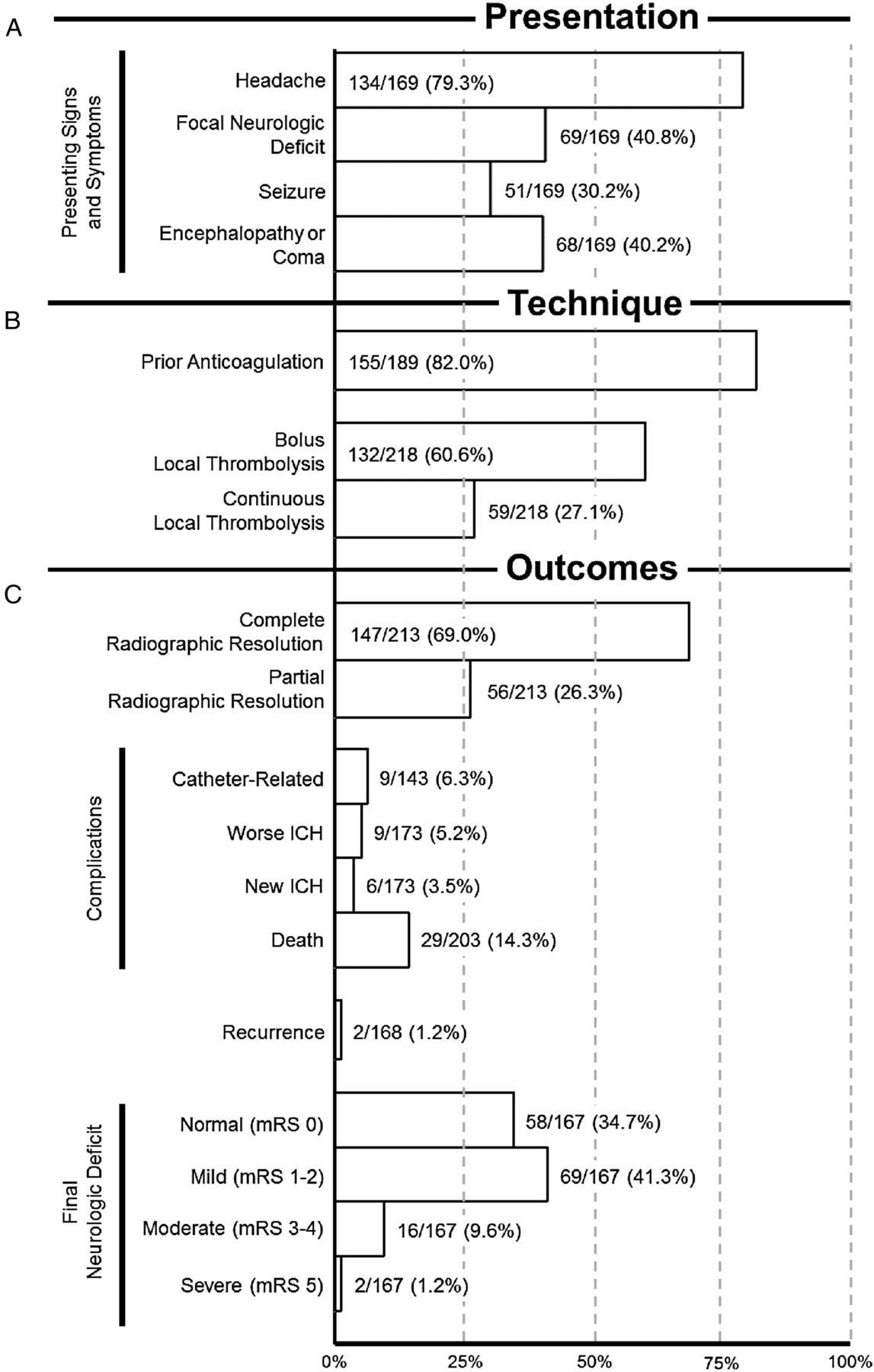
Figure 2A summarizes the reported presenting signs and symptoms of 169 patients. Headaches were present in 134 (79.3%) cases, focal neurologic deficit in 69 (40.8%), seizure in 51 (30.2%), and altered mental status in 68 (40.2%). The median symptom duration before treatment ranged from 1.5 to 21 days. The superior sagittal sinus was involved in 72.2% (130/180) of cases, straight sinus (StS) in 30.3% (30/99), transverse sinus (TrvS) in 78.0% (110/141), and sigmoid sinus (SgS) in 45.7% (59/129).

Bar graph summarizing pooled data from 17 studies related to (A) patient presentation, (B) endovascular technique and use of adjunctive therapy, and (C) outcomes. ICH, intracranial hemorrhage; mRS, modified Rankin Scale.
Treatment characteristics
Data regarding EMT type and use of associated adjuvant therapies are summarized in online supplementary table S2. Indications for EMT were available in 16 studies, including failure of systemic anticoagulation, extensive clot burden, cerebral edema, elevated intracranial pressure, altered mental status, and progressively worsening neurological symptoms. Information about prior systemic anticoagulation was available in 82.4% (14/17) of studies. Prior to EMT, 82.0% (155/189) of patients received anticoagulation therapy (figure 2B).
Of the 235 patients who underwent EMT, catheter thrombolysis was performed in 76 cases (32.3%), balloon-assisted thrombectomy in 56 (23.8%), AngioJet (Possis Medical, Minneapolis, Minnesota, USA) in 60 (25.5%), stent retrievers in 27 (11.5), Penumbra aspiration system (Penumbra Inc, Alameda, California, USA) in 21 (8.9%) cases, and Merci retriever (Stryker, Kalamazoo, Michigan, USA) in 2 (0.9%) cases. The use of specific stent retrievers was as follows: Solitaire stent retriever (Covidien, Irvine, California, USA) in 26 (11.1%) cases and Trevo stent retriever (Stryker, Kalamazoo, Michigan, USA) in 1 (0.4%) case. Endovascular bolus chemical thrombolysis was used in 60.6% (132/218 patients) of cases, while continuous thrombolysis was employed in 27.1% (59/218). Duration of continuous thrombolysis ranged from 1 hour to 5 days.
Outcomes and complications
Table 1 summarizes the outcomes and complication data following EMT for CVST.
Summary of follow-up and outcome data for all 17 studies presented individually and pooled
The outcomes data are depicted in figure 2C. Postoperative complete radiographic resolution of CVST was achieved in 69.0% (147/213) of cases, while partial resolution was achieved in 26.3% (56/213). The CVST could not be recanalized in 4.7% (10/213) of patients, resulting in death in 83% (5/6) of such cases. Procedural complications included catheter-related complications (eg, catheter-tip fracture, groin/retroperitoneal hematoma, and sinus perforation) in 6.3% (9/143) of cases, worsening intracranial hemorrhage (ICH) in 5.2% (9/173), and new ICH in 3.5% (6/173).
The follow-up duration ranged from 5 to 42.3 months, with CVST recurrence noted in 1.2% (2/168) of cases. At last follow-up, 34.7% (58/167) of patients had no neurological deficit, 41.3% (69/167) had mild neurological deficits, 9.6% (16/167) had moderate neurological deficits, and 1.2% (2/167) had severe neurological deficits. The mortality rate was 14.3% (29/203 patients died).
A meta-analysis of good neurologic outcome in patients with CVST treated with EMT is presented in figure 3A. The OR of a good outcome was significantly reduced in patients treated early (OR=0.12; 95% CI 0.02 to 0.86; p=0.03). The likelihood of good outcome tended to be lower in comatose patients (OR=0.32; 95% CI 0.06 to 1.71; p=0.18) and those with preoperative ICH (OR=0.46; 95% CI 0.17 to 1.25; p=0.13). Concurrent use of chemical thrombolysis, use of newer devices, younger age, less and only superficial sinus involvement, absence of postoperative ICH complication, and complete recanalization did not significantly affect good outcome ORs. Neither concurrent use of chemical thrombolysis nor newer device affected the likelihood of new or worsening ICH development or complete recanalization (figure 3B, C).

{kind=link}
{kind=link}
{kind=link}
(A) Summary of meta-analyses for the association of various factors with good neurologic outcome (modified Rankin Scale score 0–2) at last follow-up. Summary of meta-analyses for the association of endovascular mechanical thrombectomy (EMT) alone versus combined EMT and chemical thrombolysis and association of the use of newer versus older EMT devices with the development of (B) new or worsening intracranial hemorrhage (ICH) and (C) complete recanalization. New devices: stent retrievers, Penumbra aspiration system, and Merci retriever. Old devices: catheter thrombectomy, balloon-assisted thrombectomy, AngioJet.
Discussion
Although more common in a subset of the population (eg, in women taking oral contraceptives), CVST is an overall rare cause of stroke; thus, its diagnosis requires a high index of suspicion, and patient presentation is often non-specific.1 ,24 Based on the cumulative data of 915 patients from large multicenter studies, several factors have been identified that increase the risk for poor neurological outcomes, including male gender, mental status disorder at presentation, Glasgow Coma Scale <9, and thrombosis of more than two major venous sinuses.25 ,26 The patients included in this analysis included a higher proportion of patients with altered mental status (AMS), as well as a higher proportion of involvement of major intracranial sinuses (ie, superior sagittal and transverse sinuses) and multiple sinuses.25 ,26 Therefore, patients undergoing EMT represent a subset of patients with CVST with more severe clinical presentation and larger intracranial thrombus burden, both of which portend a worse prognosis.
Previously reported rates of CVST recurrence are 2–4% at a median follow-up of up to 16 months.24–26 We found a lower rate in patients with CVST treated with EMT (1.2%). Recent diagnostic and therapeutic advances have reduced CVST mortality rates from 30–50% to 4.3–15%.24–27 At least partial recovery is expected in 87% of patients, while poor neurological outcome with permanent deficit occurs in approximately 9%.24 ,27 In a series by Ferro et al,25 62% of patients were neurologically non-focal, 32% had mild deficits, and 6% of patients had moderate or severe deficits at last follow-up. In the current analysis, most patients (83.3%) were treated with systemic anticoagulation, while very few were treated endovascularly (2.1%). Among patients undergoing EMT, we found that 76% had either complete neurological recovery or only mild deficits. Indeed, these results suggest that, despite worse presentation and more extensive disease progression in patients with CVST treated with EMT, the outcomes may be comparable to those of patients with CVST in general.
The optimal therapy for CVST is controversial, since there are limited studies that fulfill the criteria necessary for establishment of therapeutic guidelines.3 ,28 In addition to administrating antithrombotic therapy, efforts should be directed toward identification of predisposing factors or precipitating conditions, intracranial pressure management, seizure control, and headache treatment.24 Antithrombotic therapeutic options include systemic anticoagulation, endovascular chemical thrombolysis, and EMT.18 ,24 Systemic anticoagulation is the mainstay of treatment for CVST. Evidence for therapeutic anticoagulation comes from a number of small randomized trials, and a larger body of retrospective experience.3 ,29 ,30 In a randomized, placebo-controlled trial, significant benefits of IV heparinization for CVST were seen at up to 3 months’ follow-up.30 Although the results were not statistically significant, subcutaneous nadroparin, a low-molecular-weight heparin (LMWH), has demonstrated a trend towards improving CVST outcomes in a double-blind, placebo-controlled multicenter trial, and anticoagulation was found to be safe in patients with ICH secondary to CVST.3 However, another randomized controlled trial showed no improvement in the efficacy of LMWH compared with unfractionated heparin, but it did show decreased in-hospital mortality in the former group.29 The current European Federation of Neurologic Societies (EFNS) guidelines recommend therapeutic anticoagulation with either subcutaneous LMWH or IV heparin for the treatment of CVST; however, the duration of anticoagulant therapy has not been established.24 ,28
No randomized controlled trials have assessed the efficacy or safety of EMT for CVST. Most of the evidence for the use of EMT in patients with CVST is limited to small case series.2 ,10–12 ,18 ,21 ,22 Additionally, variations in endovascular techniques, as well as heterogeneity in patient selection criteria, follow-up, and outcome reporting methods confound the assessment of the risk to benefit profile of EMT.10 ,12–14 ,16 ,18 ,22 ,23 The Thrombolysis or Anticoagulation for Cerebral Venous Thrombosis (TO-ACT) trial is currently in the recruitment process (ClinicalTrials.gov NCT01204333) to investigate the functional outcomes of patients with severe CVST treated with endovascular thrombolysis.4 ,24 Consequently, endovascular therapy is generally reserved for patients who do not respond to, or have a contraindication to, systemic anticoagulation, those with severe neurological deficit, or those with extensive disease burden.2 ,12–14 ,18 ,20 ,31 Canhão et al 31 performed a systematic review of local thrombolytic therapy for 169 patients with CVST and found a 16% ICH rate, 48% complete recanalization rate, 79% good neurological recovery rate (mRS 0–1) at follow-up. Although local catheter thrombolysis is associated with reasonably good outcomes in published series, the significant risk of ICH has limited the use of this technique.24 ,31
As part of the acute management of CVST, the American Heart Association (AHA) considers full anticoagulation with LMWH or unfractionated heparin reasonable.2 Patients with major contraindications (eg, recent major surgery) must be evaluated on an individual basis to weigh up the risks and benefits of anticoagulation. Endovascular therapy may be considered if patients deteriorate despite medical therapy. Given the lack of randomized controlled trials, the AHA makes no recommendation as to the specific endovascular therapy to be employed in the treatment of CVST. We recommend use of EMT along with systemic anticoagulation in patients with heavy clot burden or with concurrent ICH. Although adjunctive use of chemical thrombolysis was not associated with new or worsened ICH development, it also did not yield better neurologic outcome or improved recanalization rates; therefore, EMT as a sole treatment modality is a reasonable therapeutic intervention for CVST. Patients with comatose presentation are unlikely to have good neurologic outcomes even with EMT, and this should be emphasized before intervention.
EMT offers several theoretical advantages compared with both medical therapy and local endovascular thrombolysis, as it rapidly achieves direct, immediate recanalization without the use of fibrinolytic agents.13 ,21 EMT may be effective in longstanding, hardened and calcified clots that do not resolve with systemic anticoagulation or local endovascular thrombolysis.18 Additionally, EMT may also be better suited in circumstances in which the fibrinolytic dosage should be minimized (ie, existing ICH) and in the setting of larger caliber, thicker-walled venous sinuses where intraluminal thrombolysis is more time-consuming and mechanical disruption is less likely to yield wall damage.13 ,18 EMT can be achieved by various modalities including catheter-mediated clot maceration, balloon dilatation, rheolytic systems (eg, AngioJet), micro-snaring (eg, Merci retriever), aspiration systems (eg, Penumbra aspiration pump), and stent retrievers (eg, Solitaire and Trevo). In small series, these have been associated with improvements in recanalization rates.7 ,12 ,13 ,16 ,18 ,20 ,32 Siddiqui et al 16 found a tendency toward increased direct, catheter-related complications in the EMT group compared with the local thrombolysis group; however, they point out that bulkier devices such as the AngioJet (which was used in 82% of cases) probably require more manipulation than smaller devices such as the Penumbra system. The new generation of stent retrievers may afford even better maneuverability, ease of deployment, and clinical outcomes.32 Further studies are needed to compare the efficacy and safety of individual types of EMT devices for CVST.
Study limitations
Insufficient power in our meta-analysis limits our ability to draw definitive conclusions about the effectiveness and safety of EMT for CVST. Although theoretically attractive in some cases of severe CVST with poor neurologic status at presentation, EMT has not been investigated as a primary treatment, and is therefore likely to remain primarily a salvage option for patients with CVST who are refractory to initial anticoagulation. Additionally, owing to the lack of individual patient data and combined use of different treatment modalities, stratification of outcomes for specific EMT techniques and devices was not possible. Given the novelty of these techniques, technical nature of the endovascular approach, and rarity of CVST, EMT results are likely to be influenced by neurointerventionalist experience and skill. In an attempt to mitigate this effect in our analysis, while still enabling recruitment of a sufficient number of cases for analysis, we required at least three patients with CVST to be treated with EMT as an inclusion criterion. Given the long timespan across studies in this analysis, evolution of technology also potentially affects outcome as older devices may have lower efficacy and safety profiles.
Various risk factors have been found to be associated with poor neurologic outcome in patients with CVST. Unfortunately, a lack of sufficient baseline individual patient data within the cohort studies, particularly for patients with CVST not treated with EMT, limited our ability to identify predictors of postoperative neurological outcome via meta-analysis. Specifically, a comparison of patients with severe presentation treated with conventional therapy versus EMT would have been informative. Insufficient data also prevented us from correlating clot chronicity and length to outcome. Furthermore, the lack of sufficient granularity with respect to individual patient data prevented us from performing a time-dependent analysis (eg, Kaplan–Meier method) of post-EMT outcomes. All studies were retrospective, and the concomitant risks of bias were assumed for retrospective studies.
Conclusions
Patients undergoing EMT for CVST tend to have worse initial clinical presentation and greater initial clot burden, portending a poorer prognosis. Despite these poor baseline characteristics, approximately 70–80% of patients achieved functional independence, with procedural complication and new or worsening ICH rates of <10%. Therefore, EMT represents a reasonably efficacious and safe salvage therapy for patients whose disease is refractory or who have contraindications to systemic anticoagulation. Further prospective, comparative trials will be necessary to more rigorously assess the outcomes of EMT for CVST. Additional studies comprising individual patient data should seek to determine predictors of successful radiographic and clinical outcomes in patients with CVST treated with EMT.
References
Footnotes
Contributors Conception and design: AI, DD. Search, screening, and quality assessment of articles: AI. Statistical analysis and data interpretation: AI, C-JC. Drafting of the article: AI. Critically revising the article: all authors. Reviewed submitted version of manuscript: all authors. Administrative/technical/material support: KCL. Study supervision: KCL.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.