Article Text

Abstract
Objectives The RITUXVAS trial reported similar remission induction rates and safety between rituximab and cyclophosphamide based regimens for antineutrophil cytoplasm antibody (ANCA)-associated vasculitis at 12 months; however, immunosuppression maintenance requirements and longer-term outcomes after rituximab in ANCA-associated renal vasculitis are unknown.
Methods Forty-four patients with newly diagnosed ANCA-associated vasculitis and renal involvement were randomised, 3:1, to glucocorticoids plus either rituximab (375 mg/m2/week×4) with two intravenous cyclophosphamide pulses (n=33, rituximab group), or intravenous cyclophosphamide for 3–6 months followed by azathioprine (n=11, control group).
Results The primary end point at 24 months was a composite of death, end-stage renal disease and relapse, which occurred in 14/33 in the rituximab group (42%) and 4/11 in the control group (36%) (p=1.00). After remission induction treatment all patients in the rituximab group achieved complete B cell depletion and during subsequent follow-up, 23/33 (70%) had B cell return. Relapses occurred in seven in the rituximab group (21%) and two in the control group (18%) (p=1.00). All relapses in the rituximab group occurred after B cell return.
Conclusions At 24 months, rates of the composite outcome of death, end-stage renal disease and relapse did not differ between groups. In the rituximab group, B cell return was associated with relapse.
Trial registration number ISRCTN28528813.
- B cells
- Cyclophosphamide
- Granulomatosis with polyangiitis
- Systemic vasculitis
- Treatment
Statistics from Altmetric.com
Introduction
Two randomised controlled trials, ‘RITUXVAS’1 and ‘RAVE’2 demonstrated similar efficacy and safety between the B cell depleting monoclonal antibody rituximab and cyclophosphamide for remission induction of antineutrophil cytoplasm antibody (ANCA)-associated vasculitis assessed at 12 months and 6 months, respectively. Non-randomised studies have indicated a high relapse rate after rituximab, especially when used for relapsing disease.3 Following rituximab, no relapse prevention strategy was employed in RAVE where all therapy was withdrawn by 6 months, and in RITUXVAS only low dose glucocorticoids were continued after 6 months. In the RAVE study, of patients with relapsing and newly diagnosed disease and overall better renal function (estimated glomerular filtration rate (eGFR) ∼85 mL/min/m2), relapse rates were high and similar between groups; only 39% of the rituximab group and 33% of the cyclophosphamide/azathioprine group maintained remission at trial end.4 Uncertainty remains as to the duration of remission following rituximab for patients with newly diagnosed ANCA-associated vasculitis with renal involvement and their need for relapse prevention therapy (see online supplementary text).
Methods
Study design and outcomes
RITUXVAS was a 24-month, two parallel limb, randomised controlled trial involving 44 patients with newly diagnosed ANCA-associated renal vasculitis. Patients were randomly assigned in a 3:1 ratio to rituximab (n=33) or cyclophosphamide/azathioprine (control) groups (n=11) (see online supplementary text, figure S1 and table S2).
The predefined 24-month primary efficacy outcome was a composite of death, end-stage renal disease (ESRD) and relapse, ESRD and relapse representing failure to maintain remission and death being an early competing factor for subsequent ESRD and relapse. Secondary efficacy outcomes were time to death, ESRD and relapse. For safety and other efficacy outcomes and results see online supplementary text, table S3, and figures S2 and S3.
Statistical analysis
Results are expressed as values and percentages for categorical variables and medians and IQRs for continuous variables. Proportions were compared using the χ2 or Fisher's exact tests. Continuous variables were compared using analysis of covariance or Mann-Whitney U test. The logrank test was used for time-to-event analyses. All tests were two-sided and performed with IBM SPSS Statistics V.20, with p<0.05 to indicate statistical significance.
Results
Primary and secondary efficacy outcomes
The composite outcome of death, ESRD and relapse occurred in 14 of 33 in the rituximab group (42%) and 4 of 11 in the control group (36%) (p=1.00) (table 1, figure 1A). Median time from study entry to a first event was 246 days (0–648 days) in the rituximab group and 363 days (8–610 days) in the control group. Cumulative ESRD and relapse-free survival at 24 months was 58% in the rituximab group and 73% in the control group (p=0.37).
Outcomes at trial end

Death, end-stage renal disease (ESRD) and relapse according to study group. All analyses were calculated from the trial entry. (A) Time to composite outcome. Events were death, ESRD and first relapse. (B) Time to death. (C) Time to ESRD. ESRD censored for death. ESRD was defined as dialysis for ≥6 weeks without recovery. (D) Time to first relapse. First relapse censored for death. One further relapse occurred in the control group at 25.5 months.
There were six deaths in 33 patients in the rituximab group (18%) and three deaths in 11 patients in the control group (27%) (p=0.66). The median time to death was 85 days (22–330 days) in the rituximab group and 601 days (2–610 days) in the control group (figure 1B). Median age at death was 76 years in both the groups. Cumulative survival rates at 24 months were 82% in the rituximab group and 73% in the control group (p=0.56).
ESRD occurred in 2 of 33 in the rituximab group (6%) (at 42 days and 425 days following a renal relapse) and none in the control group (p=1.00) (figure 1C). Cumulative renal survival rates at 24 months were 93% in the rituximab group and 100% in the control group (p=0.39).
Relapses occurred in 7 of 33 in the rituximab group (21%) (1 major renal relapse resulting in ESRD and 6 minor relapses) and 2 of 11 in the control group (18%) (2 major relapses) (p=1.00). Proportionally more patients in the rituximab group had proteinase 3 ANCA (PR3-ANCA) at entry (61% vs 45% control group). Relapses in the rituximab group did not occur preferentially in PR3-ANCA patients as is the case with conventional immunosuppressants. However, this trial was not powered for subgroup analysis on the effect of ANCA on relapse. At the time of relapse four of seven in the rituximab group and one of two in the control group had positive myeloperoxidase ANCA (MPO-ANCA), while two of seven in the rituximab group and one of two in the control group had positive PR3-ANCA. Four of seven in the rituximab group (12%) had a second relapse (all minor relapses) (table 1, figure 1D). At 24 months, cumulative disease-free survival rates were 73% in the rituximab group and 90% in the control group (p=0.32). A further relapse was captured in the control group at 25.5 months, making a control group disease-free survival rate of 78% at trial end. Median time to the first relapse was 378 days in the rituximab group, and relapses in the control group occurred at 363 days and 775 days.
B cells and ANCA
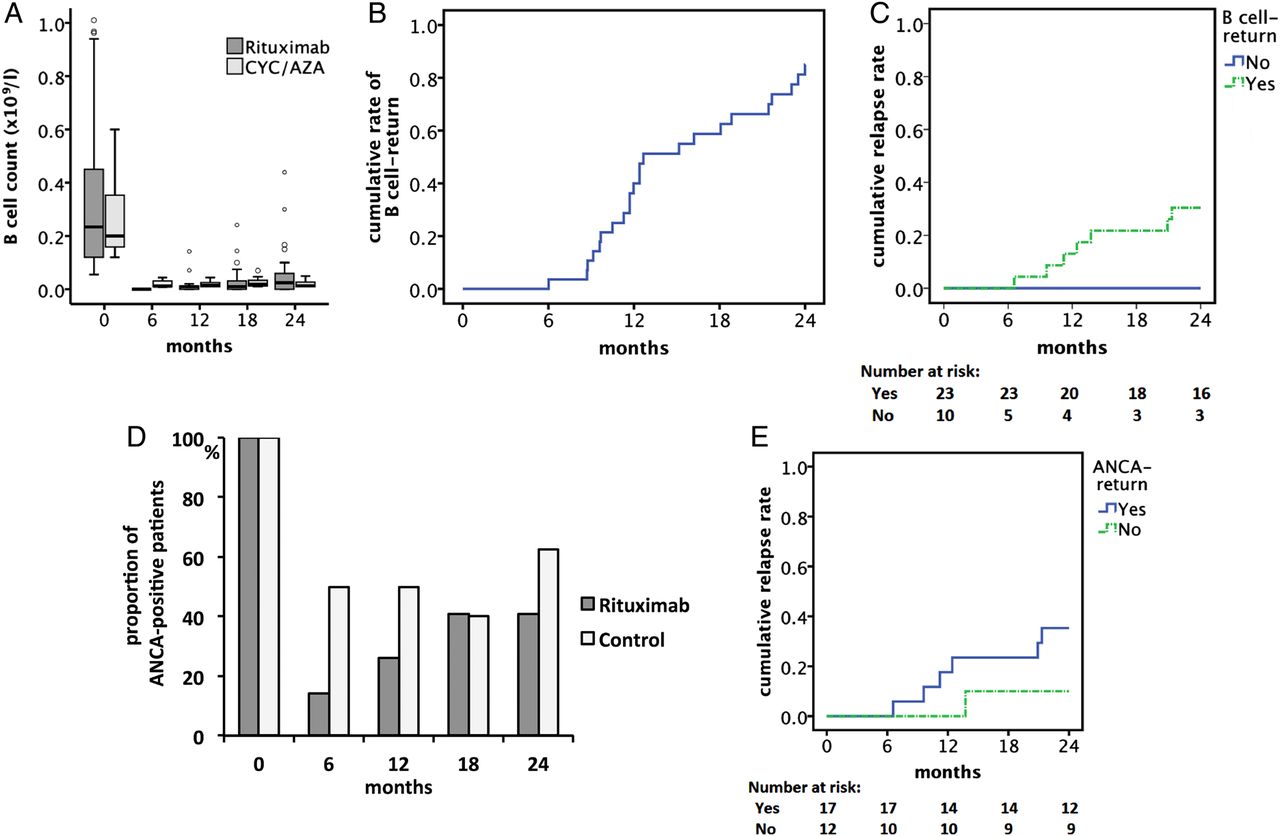
B cell counts fell in both groups (figure 2A) but fell further in the rituximab group at 6 months, p<0.01). All in the rituximab group (n=33) and one in the control group achieved B cell depletion (<0.01×109/L). In 24 of 34 (71%), B cells returned (≧0.01×109/L) after a median of 12.6 months (figure 2B). In the rituximab group, 7 of 23 with B cell return (30%) relapsed; none of 10 without B cell return relapsed. The cumulative relapse rates at 24 months were 30% in those with B cell return and 0% in those without B cell return (p=0.22) (figure 2C).
{kind=link}
{kind=link}
Biomarkers and association with relapse. (A) B cell count according to study group. The median B cell counts at 0 month, 6 months, 12 months, 24 months were 0.234×109/L, 0.000×109/L, 0.010×109/L, 0.024×109/L in the rituximab and 0.200×109/L, 0.012×109/L, 0.014×109/L, 0.013×109/L in the control groups. All 33 patients in the rituximab group and 1 of 11 patients in the control group achieved complete B cell depletion. During the trial, 24 patients (23 in the rituximab group) had B cell return. The boxes describe the medians and IQR, vertical lines describe the 1.5 IQR, and outliers are indicated by circles. B cell counts were counted as 0 per litre when below the lower detection limit. (B) Time to B cell return in the rituximab group. Median time to B cell return was 12.6 months. (C) Time to relapse from trial entry in the rituximab group with or without B cell return. In the rituximab group, 7 of the 23 patients (30%) with B cell return relapsed and none of the 10 patients (0%) without B cell return relapsed. Relative risk for relapse in the patients with B cell return compared with patients without B cell return was 3.84 (95% CI 0.54 to 27.35). (D) Proportion of the patients with positive antineutrophil cytoplasm antibody (ANCA) by ELISA. At trial entry, all the patients in this study were ANCA-positive by ELISA. Twenty-nine of 33 in the rituximab group (88%) and 8 of 11 in the control group (73%) became ANCA-negative by ELISA at any time during the trial (p=0.34). Overall 22 of 37 patients (59%) who initially became ANCA-negative by ELISA, subsequently became ANCA-positive by ELISA. Fifteen of 37 (41%) remained ANCA-negative until trial end. (E) Time to relapse from trial entry in the rituximab group for patients with or without ANCA return by ELISA. In the rituximab group, 4 of 33 did not become ANCA-negative; follow-up in all 4 patients was limited by death within 1 year from trial entry. Of 29 rituximab patients who initially became ANCA-negative, 17 (59%) subsequently became ANCA-positive by ELISA again. Twelve of 29 (41%) remained ANCA-negative by ELISA. Six of the 17 rituximab patients with ANCA return (35%) and 1 of the 12 patients (8%) without ANCA return relapsed. Relative risk for relapse in rituximab patients with ANCA return comparing with the patients without ANCA return was 4.23 (95% CI; 0.58 to 30.79).
Twenty-nine of 33 in the rituximab group (88%) and 8 of 11 in the control group (73%) became ANCA-negative during follow-up (p=0.34) (figure 2D). In the rituximab group, 17 of 29 (59%) had a return of MPO/PR3-ANCA, while 12 of 29 (41%) remained ANCA-negative. Relapses occurred in 6 of 17 (35%) with ANCA return and 1 of 12 (8%) without ANCA return and 40% of those with ANCA return and B cell return. The cumulative relapse rates at 24 months in rituximab patients were 35% in those with ANCA return and 10% in those without ANCA return (p=0.15) (figure 2E). In the control group, five of eight (63%) had a return of ANCA while three (38%) remained ANCA-negative. Relapses occurred in two (40%) with ANCA return and none without ANCA return (see online supplementary table S2).
Discussion
Rituximab-based regimens are effective remission induction therapy for ANCA-associated vasculitis as observed at 12 months in this study (RITUXVAS) and 6 months in the RAVE trial.1 ,2 Defining longer-term outcomes after rituximab induction regimens is now important. In the RITUXVAS study we continued follow-up until 24 months to assess the need for immunosuppression maintenance after a rituximab-based induction regimen for patients with newly diagnosed ANCA-associated renal vasculitis. No differences were observed at 24 months in the primary composite outcome of death, ESRD and relapse between the rituximab-based induction regimen without maintenance therapy and the conventional cyclophosphamide regimen with azathioprine maintenance therapy. The proportion of patients that were alive, dialysis independent and in sustained remission at trial end was 58% in the rituximab group and 64% in the control group. This study was powered for the previously reported 12-month primary end point of sustained remission,1 rather than the currently reported 24-month composite remission maintenance outcome.
ANCA-associated vasculitis is a life-threatening and organ-threatening disease. With current treatments, 10–25% develop ESRD and over 90% suffer irreversible damage.5–7 Mortality rates are highest in the 1st year of diagnosis and death is a competing risk factor for ESRD and relapse, making it an important component of long-term efficacy. Mortality in this trial was high (20% overall), consistent with the level of renal dysfunction and patient age, and similar to that observed in the MEPEX trial of severe ANCA-associated renal vasculitis (methylprednisolone versus plasma exchange, creatine >500 µmol/L at entry) where mortality was 26% at 1 year.6 The majority of deaths in this trial occurred within the first 3 months when patients were most vulnerable due to active disease, poor renal function and high glucocorticoid exposure.
Rapid improvements in eGFR were observed in both groups, which were maintained at 24 months. At entry more than a third of patients were dialysis dependent or near dialysis dependent (eGFR <15 mL/min/1.73 m2), of whom, 53% in the rituximab group survived and recovered renal function (achieving an eGFR >15 mL/min/1.73 m2). Again, this rate of renal recovery is similar to that observed in the MEPEX trial (59% overall).6
Conventional cyclophosphamide/azathioprine regimens are associated with relapse rates of 20–30% at 2 years.5 Granulomatosis with polyangiitis, PR3-ANCA positivity and good renal function are risk factors for relapse. ESRD is associated with a reduction in peripheral B cell counts which may contribute to the lower relapse rates associated with renal impairment.8 Relapse rates were similar between groups and relatively low, consistent with all patients having renal disease. Eighteen per cent of the cyclophosphamide/azathioprine group and 21% of the rituximab group relapsed, which in the absence of maintenance therapy and only low-dose prednisolone in the rituximab group, may be due to a prolonged effect on disease activity by rituximab. Rituximab was accompanied by B cell depletion in all patients. However, B cell depletion was not maintained and 85% of rituximab patients alive at trial end had B cell return with B cell counts trending towards normal.
All relapses in the rituximab group occurred after B cell return, suggesting that sustained B cell depletion is required for remission maintenance and that the prolonged benefit of the rituximab regimen was predominately due to rituximab rather than the initial cyclophosphamide or plasma exchange (24%). In the control group, reductions in peripheral B cells also occurred, which were sustained until trial end.
PR3 and MPO-ANCA are implicated in the pathogenesis of ANCA-associated vasculitis, inducing vasculitis in animal models.9 ,10 In this trial, 88% of patients in the rituximab group and 73% in the control group became ANCA-negative by ELISA during follow-up. The majority of relapses in the rituximab group (71%) occurred after ANCA-return. The re-emergence of both ANCA subtypes prior to relapse suggests that the elimination of ANCA-specific B cells is required for long-term remission after rituximab in patients previously naïve to immunosuppression.
In summary, at 24 months a rituximab-based induction regimen without maintenance therapy and a cyclophosphamide induction regimen with azathioprine maintenance therapy were similar in the frequency of the composite outcome of death, ESRD and relapse and in the frequency of each composite component in ANCA-associated renal vasculitis. Relapses in rituximab patients were observed after B cell return and usually after ANCA return, suggesting that while the rituximab based induction regimen offers a potential alternative to cyclophosphamide/azathioprine over 24 months, it did not induce long-term remission or cure. Following rituximab, vigilance for relapse is therefore warranted particularly in patients with detectable peripheral blood B cells and ANCA. In order to improve on current remission maintenance outcomes, maintenance therapy following rituximab-based induction regimens requires investigation (see online supplementary text).
Acknowledgments
The authors thank the National Institute for Health Research Cambridge Biomedical Research Centre, Dr Afzal Chaudhry of Addenbrooke's Hospital for developing the trial database, Drs Annelies Berden and Ingeborg Bajema of Leiden University Medical Center for histological review of renal biopsy specimens, Mrs Dorothy Walsh for her contribution in data managing, all the physicians and nursing staff who contributed to this trial, especially Denise Brown of the Nuffield Orthopaedic Centre, Jo Gray and the Wellcome Trust Clinical Research Facility in Birmingham, Frances Skilton of the Royal Adelaide Hospital, Karen Dahlsveen of Addenbrooke's Hospital, and the primary and secondary care physicians who referred patients for this trial.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online figures
- Data supplement 3 - Online tables
Footnotes
Handling editor Tore K Kvien
SF is the shared first author.
Contributors DRWJ and RBJ were responsible for trial design, sponsorship and coordination. SF performed the statistical analysis. RBJ, SF and DRWJ were responsible for the first draft of the manuscript. All authors contributed to trial conduct and final manuscript preparation.
Funding The trial was sponsored by Cambridge University Hospitals National Health Service Foundation Trust and was conducted according to the European Union Clinical Trials Directive (Directive 2001 EU/20/EC) (EudraCT number, 2005-003610-15). Registration; ISRCTN28528813.
This study was supported by Cambridge Biomedical Research Centre, a research grant from F Hoffmann-La Roche, who also provided rituximab for the study. MW is supported by a New Investigator award from the Kidney Research Scientist Core Education and National Training Program.
Competing interests RBJ reports receiving lecture fees from F Hoffmann-La Roche and undertook an academic secondment to GlaxoSmithKline from 2011–2013; DRWJ, consulting and lecture fees from F Hoffmann-La Roche; JWCT, lecture fees and book royalties from F Hoffmann-La Roche; VT, travel support from F Hoffmann-La Roche; TH lecture fees and consulting fees from F Hoffmann-La Roche and GlaxoSmithKline; RL, consulting fees from Schering-Plough and F Hoffmann-La Roche and travel support from Wyeth, F Hoffmann-La Roche, and Abbott; and COS, consulting fees from Biogen Idec and GlaxoSmithKline and a paid sabbatical at GlaxoSmithKline after the completion of this study. Addenbrooke's Hospital has received grant support and lecture fees from F Hoffmann-La Roche for services provided by DRWJ. The University of Birmingham has received grant support from Biovitrum and Talecris for services provided by COS.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement Data from this paper has been presented in abstract format at international meetings.