Article Text

Abstract
The management of patients with suspected viral encephalitis has been revolutionised in recent years with improved imaging and viral diagnostics, better antiviral and immunomodulatory therapies, and enhanced neurointensive care. Despite this, disasters in patient management are sadly not uncommon. While some patients are attacked with all known antimicrobials with little thought to investigation of the cause of their illness, for others there are prolonged and inappropriate delays before treatment is started. Although viral encephalitis is relatively rare, patients with suspected central nervous system (CNS) infections, who might have viral encephalitis, are not. In addition, the increasing number of immunocompromised patients who may have viral CNS infections, plus the spread of encephalitis caused by arthropod-borne viruses, present new challenges to clinicians. This article discusses the Liverpool approach to the investigation and treatment of adults with suspected viral encephalitis, and introduces the Liverpool algorithm for investigation and treatment of immunocompetent adults with suspected viral encephalitis (available at www.liv.ac.uk/braininfections).
Statistics from Altmetric.com

Virions of herpes simplex virus within the neuron, from a patient who died of herpes simplex encephalitis. From Oppenheimer’s Diagnostic Neuropathology, Third Edition, Hodder Arnold 2006 © Margaret Esiri and Daniel Perl
There can be few things more frightening than seeing an adult or child who was perfectly fit and well, progress from a flu-like illness to confusion, coma and death within a few days, despite the best treatment efforts. Even when treatment is successful and patients survive apparently intact, in many cases the family say that the person they took home with them is not the same as the one they brought to hospital, with changes in personality, irritability, and poor short-term memory. The management of patients with suspected encephalitis has been revolutionised in recent years with improved imaging and viral diagnostics, better antiviral and immunomodulatory therapies, and enhanced neurointensive care settings. Despite this, disasters in patient management are sadly not uncommon. Although viral encephalitis is relatively rare, patients with suspected central nervous system (CNS) infections, who might have viral encephalitis, are not. In addition, the increasing number of immunocompromised patients, who may have viral CNS infections, plus the spread of encephalitis caused by arthropod-borne viruses, present new challenges to clinicians. This review aims to provide a rational approach to the investigation and treatment of a patient with suspected viral encephalitis.
WHAT IS ENCEPHALITIS?
Encephalitis means inflammation of the brain parenchyma, and comes from the Greek enkephalon, brain. Encephalitis can be caused directly by a range of viruses, the herpes viruses and some arboviruses being especially important (table 1). Other microorganisms can also cause encephalitis, particularly protozoa such as Toxoplasma gondii, and bacteria such as Listeria monocytogenes and Mycobacterium tuberculosis (table 2). For viruses such as HIV that infect the brain but without causing inflammation, the term “encephalitis” is not usually used. Encephalitis can also occur as an immune-mediated phenomenon—for example, acute disseminated encephalomyelitis (ADEM, which follows infections or vaccinations), paraneoplastic limbic encephalitis, and voltage gated potassium channel limbic encephalitis.1
Causes of acute viral encephalitis (modified from Solomon and Whitley58)
Diseases that may mimic viral meningoencephalitis (modified from Solomon and Whiteley58)
Strictly speaking, encephalitis is a pathological diagnosis that should only be made if there is tissue confirmation, either at autopsy or on brain biopsy. However, in practice most patients are diagnosed with encephalitis if they have the appropriate clinical presentation (febrile illness, severe headache reduced consciousness (see below)) and surrogate markers of brain inflammation, such as inflammatory cells in the cerebrospinal fluid (CSF), or inflammation shown on imaging, especially if an appropriate organism is detected. Encephalitis must be distinguished from encephalopathy, the clinical syndrome of reduced consciousness, which can be caused by viral encephalitis, other infectious diseases, metabolic disorders, drugs and alcohol. Metabolic and toxic causes of encephalopathy can usually be distinguished from viral encephalitis by the lack of any acute febrile illness, more gradual onset, lack of a CSF pleocytosis and absence of focal changes on brain MRI.2
Some of the organisms that cause encephalitis often also cause an associated meningeal reaction (meningitis), spinal cord inflammation (myelitis), or nerve root involvement (radiculitis); these terms are sometimes used in various combinations to reflect whichever part of the neuraxis is affected—for example. meningoencephalitis, encephalomyelitis, meningoencephalomyelitis, myeloradiculitis, meningoencephaloradiculitis. The term “limbic encephalitis” refers to encephalitis of the temporal lobes (and often of other limbic structures), while rhombencephalitis means hindbrain, or brainstem encephalitis.
PATHOGENESIS
Depending on the virus, the pathogenesis consists of a mixture of direct viral cytopathology (that is, viral destruction of cells) and/or a para- or post-infectious inflammatory or immune-mediated response (fig 1). For most viruses, the brain parenchyma and neuronal cells are primarily infected, but for some the blood vessels can be attacked giving a strong vasculitic component. Demyelination following infection can also contribute. Herpes simplex virus (HSV) for example, primarily targets the brain parenchyma in the temporal lobes, sometimes with frontal or parietal involvement. Mumps virus can cause an acute viral encephalitis, or a delayed immune mediated encephalitis. Measles virus causes a post-infectious encephalitis, which can sometimes have a severe haemorrhagic component (acute haemorrhagic leukoencephalitis). With influenza A virus, diffuse cerebral oedema is a major component in the pathogenesis, while for varicella zoster virus (VZV), vasculitis is a major pathogenic process.

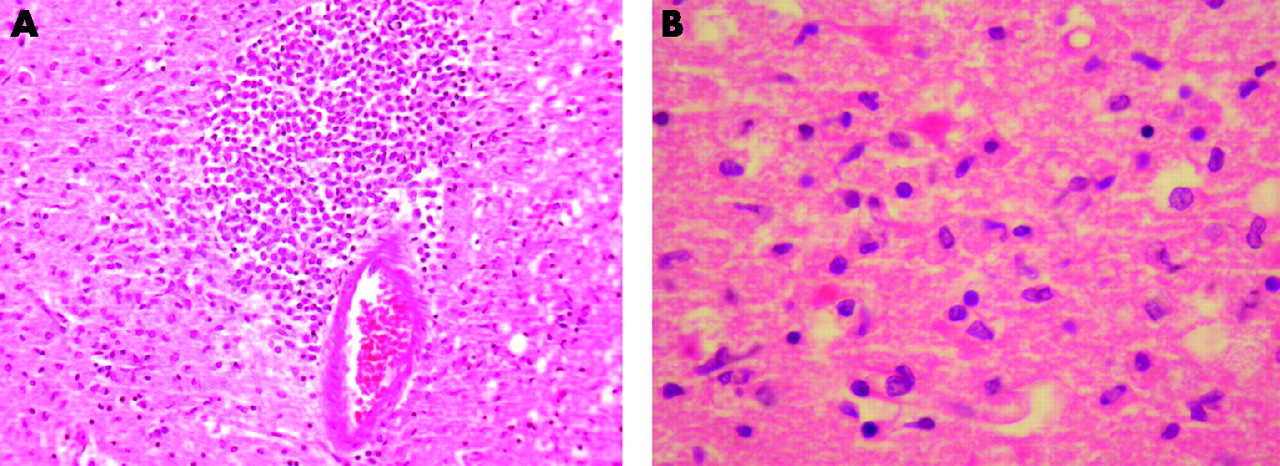
Histopathological picture of the temporal cortex of a man who died from herpes simplex virus encephalitis. (A) Intense perivascular inflammatory infiltrate consisting of activated microglia, macrophages and lymphocytes (H&E staining, ×20). (B) High power view showing microglia and dead neurons with nuclear dissolution (karyolysis) and hypereosinophilia within the cytoplasm retaining the original pyramidal contour (H&E ×40). (Pictures courtesy of Dr Daniel Crooks.)
How and when the virus crosses the blood brain barrier is a key issue in the pathogenesis of any viral encephalitis.
For example, primary infection with HSV type 1 (HSV-1) occurs in the oral mucosa, and may cause herpes labialis (vesicles and ulcers around the mouth) or be asymptomatic (serological studies show that up to 90% of healthy adults have been infected with HSV-1). Following primary infection the virus travels centripetally along the trigeminal nerve to give latent infection in the trigeminal ganglion, in most if not all those infected. About 30% of infected people have clinically apparent herpes labialis, but even asymptomatic individuals have episodes or viral shedding. About 70% of cases of HSV-1 encephalitis already have antibody present, indicating that reactivation of virus must be the most common mechanism;3 however, it is not clear whether this is due to reactivation of virus in the trigeminal ganglion, or virus that had already established latency in the brain itself.4 Why HSV sometimes reactivates is not known. In contrast to adults, in younger patients, particularly children, HSV-1 encephalitis occurs during primary infection.
HSV type 2 (HSV-2) is usually transmitted via the genital mucosa, causing genital herpes in adults. In the USA approximately 20% of individuals are sero-positive for HSV-2. The neurological syndromes it causes include meningitis, especially recurrent meningitis, encephalitis, particularly in neonates, and lumbosacral radiculitis. Most cases of recurrent meningitis that were previously called Mollaret’s meningitis are now thought to be due to HSV-2, although some feel the term Mollaret’s should still be reserved for those with recurrent meningitis in whom the cause is still not known. Neonates can also be infected with HSV-2 during delivery to cause neonatal herpes, a disseminated infection—often with CNS involvement.
The other major route by which viruses enter the nervous system is during a viraemia and subsequent spread across the blood brain barrier. This occurs with enteroviruses such as poliovirus and arboviruses such as West Nile virus.
EPIDEMIOLOGY OF VIRAL ENCEPHALITIS
Changing epidemiology
While HSV-1 encephalitis occurs with dependable regularity across the globe, there have been notable changes in the epidemiology of other viral causes:
-
Cytomegalovirus (CMV) and Epstein-Barr virus (EBV), and to some extent human herpes virus (HHV)-6, are being seen more often because they occur in patients immunocompromised by HIV, transplant or cancer chemotherapy.
-
Arboviruses such as West Nile virus and Japanese encephalitis virus are spreading to new areas.5 West Nile virus has caused outbreaks in the Americas and southern Europe, and there is evidence suggesting the virus has reached the UK,6 although it has not yet caused human disease there. The contribution of climate change to the spread of these viruses is not clear. Other viruses that have caused large unexpected outbreaks in Asia and are spreading include enterovirus 71, and Nipah virus. Enterovirus 71 has caused massive outbreaks of hand foot and mouth disease in Asia in recent years, which is often associated with aseptic meningitis, encephalitis or myelitis.7 Nipah virus is a morbillivirus (in the same family as measles) that was recognised for the first time in 1998 when it caused encephalitis in humans in Malaysia.8 This virus has also caused disease in Bangladesh and appears to be spreading.
-
Encephalitis caused by vaccine preventable viruses such as measles and mumps is less common in industrialised nations; however, in the UK reduced vaccine uptake in recent years has been associated with a resurgence of these viruses.9
Incidence of viral encephalitis
It is difficult to determine the incidence of encephalitis because the various studies have used different case definitions and viral diagnostic capabilities. However, most studies report an annual incidence of 5–10 per 100 000,10,11 highest in the young and elderly. Higher incidences are found in areas with arthropod-borne viruses. A lower annual incidence of 1.5 per 100 000 has been reported in England, based on hospitalisation data,12 although this was probably an underestimate. HSV encephalitis is the most commonly diagnosed viral encephalitis in industrialised nations, with an annual incidence of 1 in 250 000 to 500 000.13 Most HSV encephalitis is due to HSV-1, but about 10% are HSV-2. The latter typically occurs in immunocompromised individuals, and neonates, in whom it causes a disseminated infection.
WHEN SHOULD ENCEPHALITIS BE SUSPECTED?
The classical presentation of viral encephalitis is generally as an acute flu-like prodrome, developing into an illness with high fever, severe headache, nausea, vomiting and altered consciousness, often associated with seizures and focal neurological signs (fig 2). Eighty five (91%) of 93 adults with HSV-1 encephalitis in one recent study were febrile on admission.14 Disorientation (76%), speech disturbances (59%) and behavioural changes (41%) were the most common features, and one third of patients had seizures.14 Alterations in higher mental function include lethargy, drowsiness, confusion, disorientation and coma. With the advent of CSF PCR more subtle presentations of HSV encephalitis have been recognised;15 low grade pyrexia rather than a high fever, speech disturbances (dysphasia and aphasia), and behavioural changes which can mistaken for psychiatric illness, or the consequences of drugs or alcohol, occasionally with tragic consequences. Seizures can sometimes be the initial presenting feature of a patient with encephalitis. Any adult with a seizure in the context of a febrile illness, or a seizure from which they do not recover, must be investigated for possible CNS infection.

There are several reasons why one may not think of encephalitis, particularly a failure to appreciate the importance of altered consciousness in the context of a febrile illness, or failure to investigate these symptoms properly when they are recognised (table 3). One of the commonest failings is delay in performing a lumbar puncture in patients with an acute confusional state, which has been incorrectly attributed to a systemic infection.16 Although most viral encephalitis presents acutely, subacute and chronic presentations can be caused by CMV, VZV and HSV, especially in patients immunocompromised as a result of HIV, or immunosuppressive drugs15 (table 4).
Why encephalitis may be missed
Causes of subacute and chronic viral encephalitis
IMPORTANT FEATURES IN THE HISTORY
As well as being crucial in determining who needs investigation for encephalitis, the history can provide useful clues to aetiology. Never accept that the “history is not available” for a confused patient; track down a relative or neighbour on the phone. Comments from relatives that a patient “does not seem right”, should not be ignored, even if the Glasgow Coma Score is 15; remember this is a very crude tool that was devised for assessing patients with head injuries.
Ask about recent rashes such as measles. Even if there is no such history in the patient, ask whether others in the family or in the community have been affected (these viruses occasionally cause encephalitis without the obvious stigmata). In children, a recent rash may suggest chickenpox, parvovirus or HHV-6. Parotitis, testicular pain or abdominal pain due to pancreatitis may suggest mumps virus as the causative organism. If the patient is conscious, ask about any strange smells, which may be olfactory hallucinations reflecting frontotemporal involvement in HSV-1 encephalitis.
A travel history is essential, as are vaccination details. Travellers from Asia with fever and reduced consciousness may be infected with dengue or Japanese encephalitis viruses; they may also have acquired meningoencephalitis from eating snails carrying the rat lungworm Angiostrongylus cantonensis. Cerebral malaria should also be considered in returning travellers, especially from Africa.17
Ask if there has been any contact with animals, or whether there are sick animals in the neighbourhood. In the USA some outbreaks of West Nile virus were heralded by sick birds falling from the sky.18 The history of a dog bite in a rabies endemic area may be important,19 as may a bite or scratch from a bat; in the UK and Europe, Daubenton’s bats carry rabies-like viruses (European bat lyssaviruses).20 Other risk factors are related to occupation and recreational activities:
-
leptospirosis can be acquired from rat urine during fresh water activities
-
lymphocytic choreomeningitis virus (LCMV) is transmitted in rodent faeces; humans are exposed when cleaning out barns, etc
-
hikers in the forests of Austria, Germany, and Eastern Europe are at risk of tick-borne encephalitis virus (TBEV)
-
a related virus, Louping ill virus, causes occasional encephalitis in sheep in the Scottish Highlands, and very rarely in humans
-
hikers in the New Forest in the UK are at risk of Lyme disease.
Ask about risk factors for HIV, including previous blood transfusions, and high-risk behaviours such as intravenous drug use, sex between men, and multiple sexual partners, especially with people from high-risk areas of the world such as sub-Saharan Africa and Thailand.
IMPORTANT EXAMINATION FINDINGS
On examination the first priorities are to check that the airway is protected, assess and document the level of consciousness, using a quantitative scale such as the Glasgow Coma Scale (GCS), and treat any immediate complications of infection such as generalised seizures. For patients with mild behavioural abnormalities or disorientation, document the odd behaviour, and record the mini-mental test score. The general medical examination should include a search for other possible explanations of the coma.
Look for a purpuric (meningococcal) rash and other exanthema, bites and stigmata that may suggest an aetiology; is there the rash of shingles? Are there injection sites that might indicate intravenous drug use? Look for seborrhoeic dermatitis, oral candida or oral hairy leukoplakia in the mouth, or Kaposi’s sarcoma on the skin indicative of undiagnosed HIV infection. In patients with HIV look for mouth ulcers or umbilicated skin papules suggestive of disseminated histoplasmosis or cryptococcosis. Look at the genitals for the ulcers of HSV and chancres of syphilis. Examine also the chest, ears and urine for infection. However, beware ascribing reduced consciousness to a urinary or chest infection, especially in someone who is otherwise fit and well. Such patients need a lumbar puncture to rule out a CNS infection.
Look for seizures including subtle motor seizures, and examine the side of the tongue or inside cheek for bites indicating that a seizure has occurred. Test for meningism, and look for focal neurological signs, including hemispheric signs that could indicate an abscess, or flaccid paralysis suggestive of spinal cord involvement. Tremors and abnormal movements are seen in some forms of encephalitis, particularly those that involve the basal ganglia, such as West Nile virus and other flaviviruses, or toxoplasmosis. An acute febrile encephalopathy with lower cranial neuropathies and myoclonus suggests a rhomboencephalitis or basal meningoencephalitis, as seen with some enteroviruses, or listeria (table 5). Deafness is quite common in mumps and some rickettsial infections. Upper limb weakness and fasciculation suggest a cervical myelitis, for example in tick-borne encephalitis. Encephalitis associated with radiculitis is seen in CMV and EBV.
Brainstem encephalitis (rhombencephalitis): clues and causes
INITIAL INVESTIGATIONS
-
A peripheral blood count may show a leukocytosis or leukopenia. Atypical lymphocytes are seen in EBV infection, and eosinophilia in eosinophilic meningitis.
-
Hyponatraemia due to the syndrome of inappropriate antidiuretic hormone (SIADH) is common in encephalitis.
-
A raised serum amylase is common in mumps virus infection.
-
If there has been a respiratory component to the presentation check for cold agglutinins, which occur in mycoplasma infection, and order appropriate serological investigations for mycoplasma and chlamydia (atypical respiratory infections).
-
Blood cultures should be taken as part of the investigation of possible bacterial causes, and PCR of the blood for meningococcus considered.
-
Bacterial antigen testing of CSF and urine may be helpful.
-
A chest x ray is essential to look for pulmonary infiltrates in atypical pneumonia, for example in mycoplasma pneumonia, legionella or LCMV.
-
HIV testing should also be considered, especially if the cause of CNS infection is uncertain. Our practice is to perform the test in all patients with undiagnosed CNS infection because if positive it makes such a difference to the differential and management.
THE LUMBAR PUNCTURE CONTROVERSY
Few topics have led to as much confusion, contradiction and controversy as the role of lumbar punctures in patients with suspected CNS infection.21 A lumbar puncture is an essential investigation because the initial CSF findings (especially the cell count, differential and glucose ratio) reveal firstly whether or not there is infection, and secondly whether it is likely to be bacterial or viral infection, which thus informs the initial antimicrobial therapy. Subsequent studies such as culture and PCR confirm precisely what the organism is, which allows the therapy to be tailored and appropriate public health measures, including disease notification, to be organised.
However, if patients have a space-occupying lesion, marked brain swelling, or brain shift (for example herniation across the midline, the tentorium or the foramen magnum), then a lumbar puncture may of course make things worse. Raised intracranial pressure itself is not a problem—indeed patients with idiopathic intracranial hypertension are treated by lumbar punctures, and in most patients with CNS infection the CSF opening pressure is raised to some degree.22,23 The problem is the swelling or shift which is sometimes associated with the raised pressure, so the pressure is not the same in all the CSF compartments. For this reason patients should be assessed for clinical features which might indicate a space-occupying lesion, brain swelling or shift, and who should then have computed tomography (CT) before lumbar puncture (fig 3); focal neurological signs (for example a hemiparesis), new onset seizures, papilloedema and deep coma. CT is also recommended for immunocompromised patients, who may lack the clinical signs of an inflammatory mass lesion.24 Opinions vary as to what level of “deep coma” necessitates a CT scan before lumbar puncture. To some extent it depends on how quickly imaging can be organised. If a CT scan can be performed promptly, so that it will not delay lumbar puncture for more than an hour or two, then it is reasonable to do this first. However, in a patient who is only mildly confused with no focal neurological signs, than a lumbar puncture should be done straight away, without the unnecessary delay of a CT.24
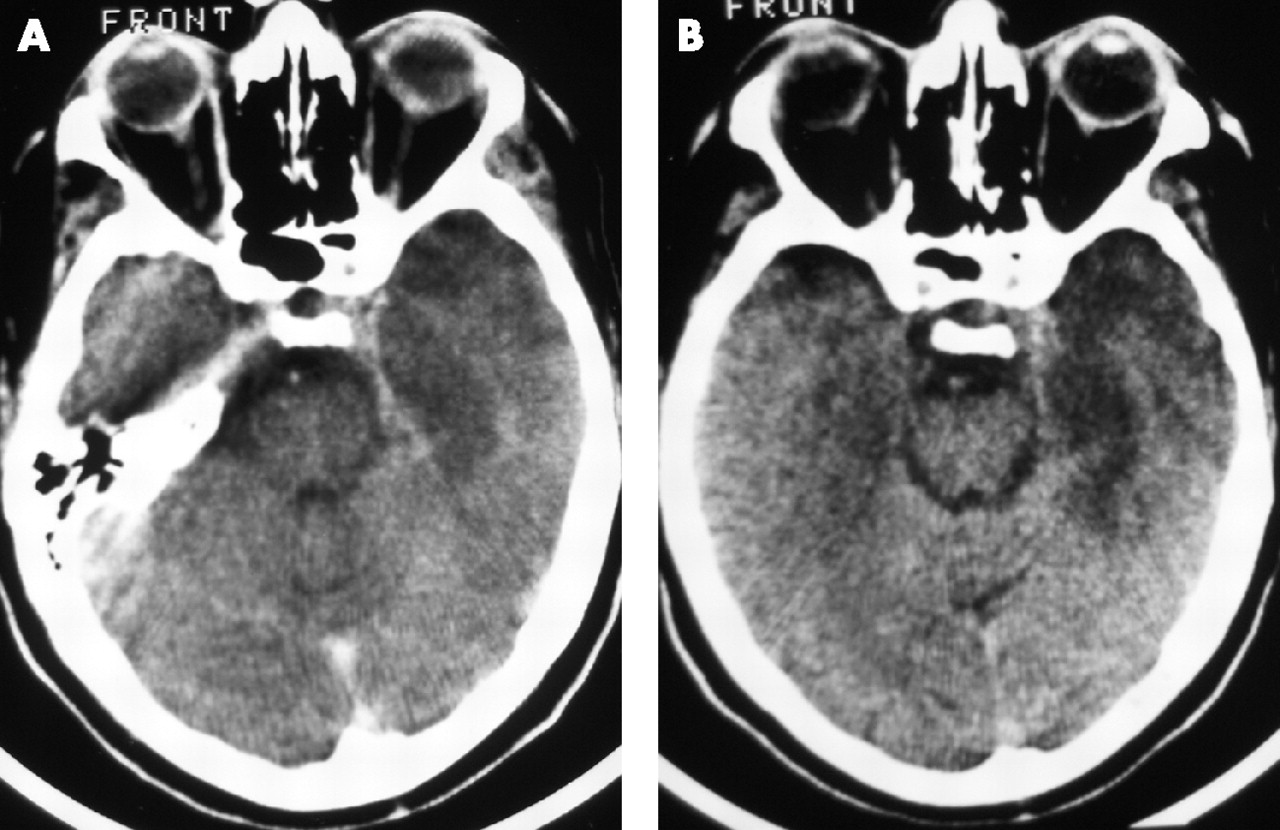
CT scan with contrast of a middle-aged man with a one-week history of a flu-like illness, severe headache and increasing confusion, who had HSV encephalitis confirmed by CSF PCR. (A) A low density area in the left temporal lobe, with swelling and some contrast enhancement. (B) The same patient four days later with more marked changes (Photos: T Solomon).
If a CT is going to cause a delay of several hours, then presumptive treatment for both bacterial and/or viral pathogens should be started. There are no hard and fast rules about how long a delay is acceptable before treatment is initiated. For bacterial meningitis a delay of more than six hours between arrival in hospital and initiation of antibiotic treatment is associated with a worse outcome.25 If patients have a purpuric rash suggestive of meningococcal septicaemia, or are deteriorating rapidly, antibiotics should be started immediately.26 In HSV-1 encephalitis, a bad outcome is associated with a delay of two days or more between hospitalisation and starting treatment.14 In practice, HSV encephalitis is rare, and most suspected cases turn out to have something different.27 While one would not advocate unnecessary delays, together these data suggest that for patients with suspected encephalitis the emphasis should be on investigating promptly where possible before starting treatment. For most patients with no contraindication, it should be possible to perform a lumbar puncture, and get the result back within a few hours to then guide the management. If there are delays or a patient appears to be deteriorating, then presumptive treatment with aciclovir is appropriate, at least while investigations proceed.
For patients with suspected bacterial meningitis or viral encephalitis, even if antimicrobial treatment has been started, it is still essential to perform a lumbar puncture, because this informs the diagnosis and guides subsequent management.28 Giving blind antibacterial and antiviral treatment to all patients with suspected CNS infection, and then not investigating with lumbar puncture because it “makes no difference to the management” is unacceptable practice and should be discouraged.21 This approach risks missing other diagnoses that may require alternative treatments,29 and increases the risk of adverse effects of the unwarranted and unnecessary drugs. For HSV-1 encephalitis, PCR of the CSF remains positive in about 80% of patients even a week after starting antiviral therapy.13
CEREBROSPINAL FLUID FINDINGS
In encephalitis, the CSF opening pressure is often slightly raised, and there is usually a mild to moderate CSF pleocytosis of 5–1000 cells/mm3, with predominant lymphocytes (table 6). However, early in the infection the CSF white cell count may be normal, or neutrophils may predominate, as they do in viral meningitis.30 The CSF red cell count is usually normal, or slightly raised, but it may be markedly raised in HSV-1 encephalitis, which can be haemorrhagic, or in acute necrotising haemorrhagic leukoencephalitis. The glucose ratio is usually normal in viral CNS infections, though it may be a little reduced—for example, in mumps or enterovirus infection.31 The CSF protein is often slightly raised, between 0.5 and 1.0 g/l.
Typical cerebrospinal fluid findings in central nervous system infections
DIAGNOSTIC VIROLOGY
The definitive diagnosis of a viral CNS infection is based on demonstrating the virus in the CNS, either from culture or PCR of brain tissue or CSF, or by demonstrating a specific antibody response in the CSF. Less strong evidence comes from detecting virus elsewhere in the body of a patient with a CNS syndrome (for example, from throat, rectal or vesicle swabs), or showing an antibody response to the virus in the serum (the organism is then presumed to be responsible for the clinical presentation, although there is always the possibility that it is a coincidental infection).
PCR of CSF
The diagnosis of viral encephalitis used to rely on brain biopsy,27 but many important viruses can now be detected with PCR.32,33 PCR tests for HSV have overall sensitivity and specificity >95%, but may be negative in the first few days of the illness, or after about 10 days.34,35 Initial investigation of immunocompetent patients with encephalitis should include PCR for both HSV and VZV because these are potentially treatable with aciclovir (see below) (table 7). Enterovirus PCR is often included at this stage, because it is a relatively common cause of viral meningitis, especially in the summer/autumn. In immunocompromised patients, EBV and CMV PCR should also be performed, and HHV-6 and HHV-7 considered. Measles and mumps should be looked for if there is a suggestive clinical indication, although they can occasionally cause encephalitis in patients with no other features. Other viruses to consider, especially in children, include adenoviruses, HHV-6, respiratory syncitial virus (RSV), and influenza virus A and B; rotaviruses and parvovirus B19 are also occasionally associated with CNS disease, especially in children.36,37 PCR can also be used to detect Chlamydia pneumoniae in the CSF.
Staged approach to microbiological investigation of viral encephalitis
CSF viral culture is now rarely performed, although it has the potential advantage over PCR of being able to detect any virus, whereas PCR only detects the viruses being targeted by the panel of PCR assays used. Newer more sensitive PCR methods, such as “real-time” and quantitative PCR have improved the clinical utility of this test, and are becoming available for herpes viruses and enteroviruses.38
One problem is that the high sensitivity of some of the recent PCR assays for herpes viruses, such as EBV and CMV, can make positive results difficult to interpret. Most of the adult population have been infected with these viruses and carry them in their lymphocytes. Therefore, there is debate about whether detection of the viruses by PCR of the CSF represents true pathogenic infection, rather than just the presence of infected lymphocytes.39 Where there is uncertainty about the significance of a result, the amount of virus in the CSF compared with the blood (determined by quantitative PCR) usually helps resolve it. For example, in a patient with HIV, a CSF CMV PCR titre that is higher than that in the serum is usually significant.
Antibody testing
Antibody testing continues to play an important role in the diagnosis of many viral CNS infections. Traditional techniques required the demonstration of a fourfold rise in antibody between acute and convalescent serum samples collected 2–4 weeks apart, and thus are not helpful in making an early diagnosis. And in practice convalescent samples are often forgotten.
Newer enzyme immunoassays can detect immunoglobulin (Ig)-M and IgG antibodies in the serum and CSF against most of the important viruses, as well as Mycoplasma pneumoniae. Specific anti-viral IgM is often produced within a few days of a primary infection and can be measured by IgM enzyme immunoassays. The detection of virus specific IgM antibodies in the CSF in higher titres than in serum indicates local production of antibody in the CNS in response to infection. IgM does not normally cross the blood-brain barrier because of its size. However, if there is inflammation the barrier is leaky to IgM, and other immunoglobulins. In this circumstance, the ratio of CSF to serum for the specific IgM antibody can be compared to the ratio for immunoglobulin as a whole, to decide if this is local production rather than leak across an inflamed blood-brain barrier. IgM detection is especially useful for flavivirus infections, but less so for herpes virus infections, which are often reactivations. In contrast to IgM, IgG is normally found in the CSF at a ratio of 1/200th of the serum concentration; hence in a primary acute CNS infection, IgG rises later than IgM both in CSF and serum. In reactivations and secondary infections, IgG tends to rise earlier and to a greater extent than IgM.
The detection of oligoclonal bands is sometimes a useful non-specific indicator that a patient has an inflammatory process in the CNS, rather than a non-inflammatory cause of encephalopathy. Immunoblotting of the bands against viral proteins has been used, but mostly as a research tool to help determine the cause of the inflammation—for example, HSV-1 or HSV-2.29,34 However, the detection of intrathecal anti-HSV antibody has a sensitivity of 50% by 10 days after clinical presentation, and is thus only considered useful for retrospective diagnosis.
Our practice, at least for diagnosing HSV infections, is to ask for PCR on CSF acutely. If this is negative, but suspicion remains high, PCR of the CSF is repeated after a few days (as indicated above PCR can sometimes be negative if the sample is taken early in the illness). If two CSFs are negative for HSV by PCR then it is unlikely that the patient has HSV infection. If for logistic reasons CSFs were not taken at this time, or were not sent for HSV PCR, then testing a late CSF (for example, later than 10 days of hospitalisation) for the production of intrathecal antibodies against HSV, by IgM, IgG or antibody-mediated immunoblotting of oligoclonal bands, can be useful.
INVESTIGATION OF OTHER SAMPLES
Other investigations include:
-
PCR and/or culture of throat and rectal swabs for enteroviruses, mumps virus or measles virus.
-
PCR or antigen detection and culture of nasopharyngeal aspirates for respiratory viruses such as adenoviruses, RSV, parainfluenza viruses or influenza viruses.
-
Urine culture for mumps virus.
-
Chlamydia pneumoniae and Mycoplasma pneumonia can also be detected in throat swabs using PCR.
-
Vesicles, for example in hand foot and mouth disease, should be aspirated for culture or PCR, for enteroviruses.
-
VZV or HSV can be detected in herpetic rashes by cell culture, antigen detection by immunofluorescence or PCR. Electron microscopy of vesicle fluids may also demonstrate herpes viruses.
In general, a virus detected in sterile sites, such as vesicles, is more likely to be causal than a virus from non-sterile sites. For example, enteroviruses detected in vesicle swabs indicate that they are temporally associated with the acute infection, whereas shedding from the rectum occurs for several weeks after an acute infection.40
The list of all possible investigations for causes of viral CNS disease is clearly very long. Our practice is to do the initial CSF PCR for HSV and VZV as soon as the samples are received, because of their importance for early management. PCR for enteroviruses and parechoviruses is also usually done at this stage. In addition, patients that are immunocompromised are investigated with CMV and EBV PCR. Further investigations are guided by the clinical picture, especially the patient’s immune competence and the initial CSF findings. The opinion of a clinical virologist in assessing such patients is invaluable.
With the advent of PCR, brain biopsy of patients with suspected encephalitis has become less common. Previously it was considered the gold standard for diagnosis of HSV-1 encephalitis. It may still have a role in undiagnosed patients that are deteriorating. In one study approximately half of patients with suspected HSV-1 encephalitis who had a brain biopsy had an alternative diagnosis, of which 40% were treatable.27
IMAGING AND EEG
As described above, in patients with encephalopathy and fever, a CT scan is generally done before the lumbar puncture if there are clinical features of brain shift or a space-occupying lesion. In HSV the scan may be normal initially, or there may be subtle swelling of the frontotemporal region with loss of the normal gyral pattern (fig 1). Subsequently there is hypodensity, or there may be high signal change if haemorrhagic transformation occurs. MRI is generally more sensitive, showing high signal intensities in the brain areas affected (fig 4), but even MRI scans can look normal if performed very early.41 Diffusion-weighted MRI may be especially useful for demonstrating early changes.42
{kind=link}
{kind=link}
{kind=link}
{kind=link}
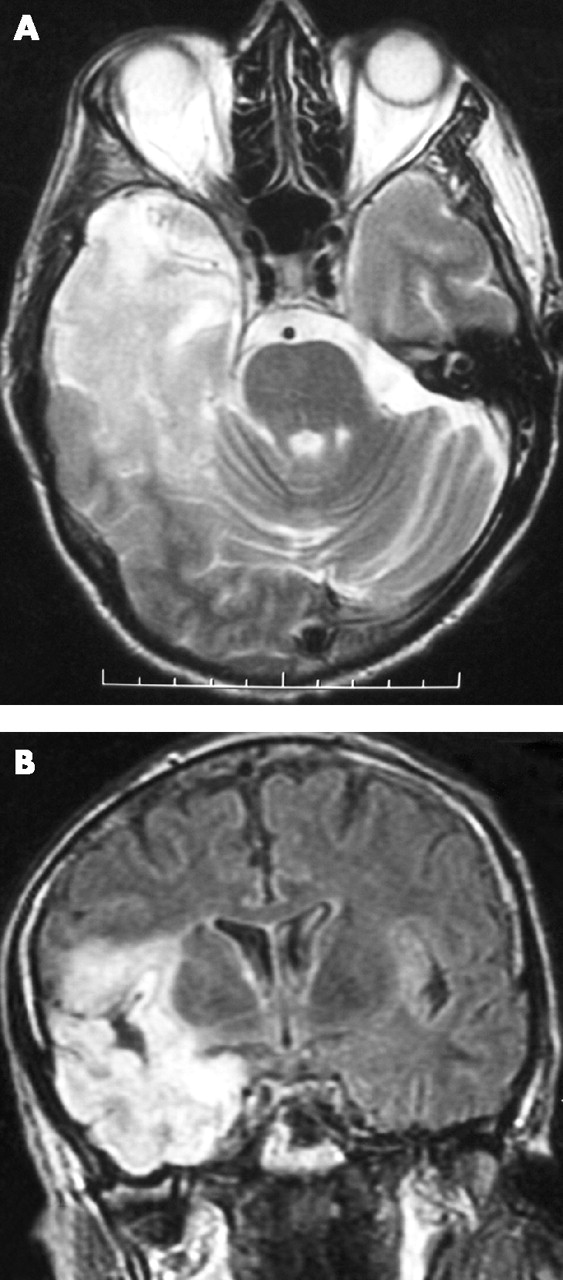
T2-weighted MRI brain scan showing right temporal lobe hyperintensity in a patient with herpes encephalitis (Photos: T Solomon).
An EEG usually shows non-specific diffuse high amplitude slow waves of encephalopathy, but can be useful to look for subtle epileptic seizures. Periodic lateralised epileptiform discharges were once thought to be diagnostic of HSV encephalitis, but have since been seen in other conditions.43
MANAGEMENT
There are three elements to the management of patients with encephalitis:
-
the first is to consider whether there is any antiviral or immunomodulatory treatment to halt or reverse the disease process;
-
the second is to control the immediate complications of the encephalitis;
-
the third is to prevent some of the secondary and late complications.
Standard intensive care for patients with encephalitis include oxygen via a mask, paying attention to fluid and hydration, nasogastric or parenteral feeding, and treating the complications of infection such as pneumonia. Patients with a reduced coma score or impaired gag reflex, should be assessed by an intensive care unit outreach team, with a view to early transfer.
When to start aciclovir
In most immunocompetent patients in developed countries aciclovir should be given as soon as there is a strong suspicion of viral encephalitis, based on the clinical presentation and initial CSF and/or imaging findings. If performing these investigations is likely to lead to long delays and the clinical suspicion is strong, then treatment should be started at once, for both viral encephalitis and possible bacterial meningitis. The situation may be different in developing countries, where the cost of aciclovir may be an issue, and other causes of CNS infection are more common. For example in much of Asia large outbreaks of Japanese encephalitis occur; in parts of Asia and sub-Saharan Africa, HIV-associated CNS infections and cerebral malaria are common.
Aciclovir is a nucleoside analogue that is highly effective against HSV and some of the other herpes viruses, such as VZV and herpes B virus. Intravenous administration of aciclovir at 10 mg/kg three times daily reduces the risk of a fatal outcome from approximately 70% to less than 20%.44,45 Renal function should be monitored closely and adequate hydration maintained, because of the rare risk of renal failure. Other rare adverse effects include local inflammation at the site of the intravenous canula, hepatitis, and bone marrow failure.
When to stop aciclovir
Although the original aciclovir trials were for 10 days’ treatment, most physicians continue for 14 or 21 days, especially in patients with proven herpes encephalitis, because of the risk of relapse after 10 days.46 Some advocate repeating the CSF examination at the end of treatment and continuing with aciclovir if HSV is still detected by PCR. This approach is being evaluated by the American Collaborative Antiviral Study Group, which is assessing the prognostic value of quantitative PCR detection of viral DNA in the CSF at the end of three weeks’ treatment and prolonged high dose oral valaciclovir for three months.
If the initial CSF PCR is negative for HSV but other features are consistent with HSV encephalitis, then the aciclovir should not be stopped, because false negative PCR results can occur, particularly early on.47,48 In such patients the lumbar puncture should be repeated because it may be positive 24–48 h later and, even if negative again, treatment continued for at least 10 days. However, if a definitive alternative diagnosis has become apparent, or it seems very unlikely that the patient has viral encephalitis, then it is reasonable to stop the acyclovir earlier.
A role for oral valaciclovir?
In circumstances where ongoing intravenous treatment is proving difficult (for example, in a child who is now fully conscious), oral valaciclovir may be reasonable,49 although we would only consider this after the first 10 days of intravenous treatment. Valaciclovir is the valene ester of aciclovir, which is converted to aciclovir after absorption, and has good oral bioavailability. Although oral valaciclovir may have a role, oral aciclovir should not be used in HSV encephalitis, because the levels achieved in the CSF are inadequate.
Ancillary treatments
In patients with brain swelling, corticosteroids and mannitol are often used to control raised intracranial pressure. A recent trial suggests steroids may be beneficial even in patients without marked swelling.50 Their role in HSV encephalitis merits further study.51 In patients with severe brain swelling, decompressive hemicraniectomy is sometimes performed. Antibiotic treatment with a cephalosporin is often also given, especially if the initial CSF findings could be consistent with bacterial disease (for algorithm see http://www.britishinfectionsociety.org). If listeria is suspected, ampicillin and gentamicin, or high dose cotrimoxazole, should be given.
Other antiviral and immunomodulatory treatments
There are few large, randomised controlled trials assessing the efficacy of antiviral treatments in viral CNS infections, other than for HSV encephalitis. Nonetheless treatments for other conditions are given based on an understanding of the pathogenesis, in vitro data, anecdotal reports, or small clinical series, although these sometimes provide conflicting data (table 8).
Treatment options to consider in encephalitis (modified from Boos and Esiri)52
If the clinical presentation and imaging findings suggest a post- or para-infectious encephalitis such as ADEM, acute haemorrhagic leukoencephalitis or diffuse encephalopathy associated with systemic viral infection, immunosuppressive drugs are given.52 High dose corticosteroid treatment is often the initial treatment, followed by intravenous immunoglobulin, plasma exchange, or further treatment with steroids, depending on the response to the initial treatment.
In some circumstances, both antiviral and immunosuppressive drugs are given. For example, in HSV encephalitis corticosteroids are sometimes used in addition to aciclovir as described above. In VZV encephalitis corticosteroids are used alongside aciclovir because of the strong vasculitic component of the disease.
Severe CMV and HHV-6 infections are treated with ganciclovir, foscarnet or cidofovir, severe adenovirus infections have been treated with cidofovir or ribavirin and Pleconaril has been used for severe enterovirus infections, particularly in the immunocompromised, although its overall role remains unclear.53,54 Interferon alpha has been used in West Nile virus and other flavivirus infections, but a randomised controlled trial in Japanese encephalitis showed it was not effective.55
Management of seizures, raised intracranial pressure and other complications
Seizures are common in encephalitis, particularly in children. In adults, seizures can be useful in distinguishing acute viral encephalitis from para-infectious inflammatory encephalopathies. There may be obvious generalised tonic clonic seizures or subtle motor seizures, which may manifest as twitching of a digit, or around the mouth or eyes, particularly in children. An EEG should be performed if there is any uncertainty.
Uncontrolled seizures lead to raised intracranial pressure, increased metabolic activity, acidosis and vasodilatation, which in turn leads to further raised pressure. The resulting positive feedback cycle can ultimately precipitate brain shift and herniation. If seizures are not easily controlled with phenytoin and low doses of benzodiazepines, patients should be intubated and ventilated mechanically, so that higher doses of sedating anticonvulsive drugs, including benzodiazepines and phenobarbital, can be used. Electroencephalographic monitoring, with or without continuous function and analysing monitoring (CFAM), should be used to detect ongoing epileptic activity.
Standard measures to control raised intracranial pressure include nursing the patient at 30° head up, keeping the head straight to ensure there is no obstruction to venous return, and ventilating to maintain a low arterial pCO2. Although there are no good data for viral encephalitis, data from other infectious encephalopathies suggest that osmotic diuretics produce a short-term reduction in pressure.56 The role of anti-inflammatory drugs in viral encephalitis is uncertain.51 To reduce the risk of deep venous thrombosis and pulmonary embolism, patients with reduced mobility should be fitted with compression stockings, and once it is clear that there is no major haemorrhagic component to the encephalitis, they should be given prophylactic heparin. Bed sores are a risk in immobile patients, and appropriate mattresses and regular turning are needed. Patients with encephalitis are also at risk of secondary pneumonia, due to aspiration, and urinary tract infections. Passive and active limb movements will reduce the risk of limb contractures, which can occur in patients with limb weakness, and splints and braces may be needed to facilitate mobilisation.
Management in the recovery period
Ideally, a full neuropsychological assessment should be organised at hospital discharge, or soon after. This should include cognitive function, intelligence, memory and speech assessment, because these help determine the extent of any damage, and the help that might be needed. Regular out-patient assessment following encephalitis is especially important in children. Behavioural and psychiatric disturbances are common and may include depression or disinhibition. Antidepressants and mild night-time sedatives may be necessary. Other disabilities in the recovery period or afterwards include seizures, post-encephalitic parkinsonism seen after encephalitis lethargica, and encephalitis caused by flaviviruses. The risk of seizures is greatest in those who had seizures during the acute period; in one study the cumulative risk of seizures at 5 years was 10% for patients with no acute seizures, which increased to 20% for those with acute seizures.57
PRACTICE POINTS
-
All patients with a febrile illness and altered behaviour or consciousness should be investigated for a central nervous system (CNS) infection, unless there is very clear evidence of another diagnosis.
-
Patients with a suspected CNS infection need a lumbar puncture as soon as possible, unless there is an indication for a brain CT first.
-
Patients with a meningococcal rash and/or sepsis should receive immediate antibiotics, but for most other patients investigation with lumbar puncture should be possible before starting treatment.
Memory difficulties can be particularly prominent after HSV encephalitis. A range of practical approaches can help to overcome these difficulties such as the patient keeping a notebook and diary, labelling items around the house, and leaving messages as reminders. More sophisticated aids being developed include a neuropage system (http://www.neuropage.nhs.uk), which sends pager reminder messages throughout the day, and a camera, worn around the neck, which automatically takes pictures throughout the day as a reminder of what the patient has been doing (SenseCam). Excellent help and advice can be obtained from patient support groups, such as the encephalitis society (http://www.encephalitis.info)
PROGNOSTIC FACTORS AND OUTCOME
Although treatment with aciclovir has reduced the mortality of HSV, the morbidity remains high.13 Poor prognostic factors after HSV encephalitis include age above 60, reduced coma score on admission,44 especially if ⩽6,45 and delays between hospitalisation and starting aciclovir treatment (especially delays of more than two days).14,16 Two thirds of survivors have significant neuropsychiatric sequelae, including memory impairment (69%), personality and behavioural change (45%), dysphasia (41%) and epilepsy in up to 25%.16 This means that in addition to the high hospitalisation costs estimated in the USA at $500 million for 1983 alone, there are considerable additional costs of long-term care and support. If the personal tragedies themselves were not impetus enough, this major financial burden emphasises the need for a rational approach to investigation and treatment of this devastating condition.
Acknowledgments
We thank our clinical and laboratory colleagues at the Walton Centre for Neurology and Neurosurgery and the Royal Liverpool University Hospital for help in developing the Algorithm for the Early Management of Suspected Viral Encephalitis in Adults, which is available from http://www.liv.ac.uk/braininfections (under Education). We are also grateful to members of the Encephalitis Society for sharing with us their experiences.
This article was reviewed by Neil Scolding, Bristol, UK.
REFERENCES
Linked Articles
- Editor's choice
Other content recommended for you
- The management of infants and children treated with aciclovir for suspected viral encephalitis
- How and when to use CSF to investigate neonates and children with possible central nervous system infection
- Diagnosis and treatment of viral encephalitis
- Encephalitis in children
- Infectious encephalitis: mimics and chameleons
- Factors influencing PCR detection of viruses in cerebrospinal fluid of patients with suspected CNS infections
- Early autoimmunity and outcome in virus encephalitis: a retrospective study based on tissue-based assay
- Improving the diagnosis of central nervous system infections in adults through introduction of a simple lumbar puncture pack
- Herpes simplex virus (HSV) encephalitis in a young man: an unusual course
- Neonatal herpes simplex virus infections: HSV DNA in cerebrospinal fluid and serum