Article Text

Abstract
Most patients with Guillain-Barré syndrome (GBS) respond to treatment with intravenous immunoglobulin, but it is not uncommon for some to continue to deteriorate for a period after treatment has been started. This may reflect the natural history of the disease, or an error in diagnosis. This article reflects my own view of what to do in this situation, with a review of what few data there are to guide decision making.
Statistics from Altmetric.com
A patient with clinically typical Guillain-Barré syndrome (GBS) is admitted and given five days of intravenous immunoglobulin (IVIg) at a conventional dose of 0.4 gm/kg per day. His cerebrospinal fluid (CSF) is normal on day 4 of the illness and the nerve conduction studies—limited to conduction velocities in an upper and lower limb—come back as normal. He continues to deteriorate, requiring ventilation. After a further two weeks there is no sign of improvement. What should I do now?
THE CORRECT DIAGNOSIS?
This scenario is not unusual and in a busy regional centre we see such patients several times a year. My first reaction is to make sure the diagnosis is correct. The diagnosis of GBS is usually straightforward and conditions that can cause diagnostic difficulties in the first 48 hours, such as hypokalaemia or acute polymyositis, are usually recognised fairly quickly (box). I have seen neuromyelitis optica cause more prolonged diagnostic difficulty, especially in a ventilated patient who cannot complain of visual difficulties. Nerve conduction studies are usually abnormal in GBS, even early in the course of the disease, provided detailed studies are performed (in a recent study 85% of patients had abnormal values1). These abnormalities may be limited to prolonged distal motor latencies or small and dispersed muscle action potentials, or sometimes just prolonged F wave latencies. If the nerve conduction studies remain normal on repeat testing then I wonder about lymphoma or malignant meningitis with root infiltration. These two disorders are usually associated with a CSF pleocytosis but a modest increase in cell count (up to 50/μl) is not incompatible with the diagnosis of GBS. A high CSF cell count always makes me think of Lyme disease and HIV. Although a raised CSF protein is helpful in making the diagnosis, it is frequently normal in the first week when the examination is usually performed. Repeat studies are seldom done but usually show a later rise in protein. I have seen an ependymoma present with a rapidly progressive lower motor neuron problem in the legs, with only equivocal nerve conduction studies consistent with proximal root damage. The CSF usually helps here but breast carcinoma can present with a normal CSF and a subacute neuropathy that causes confusion. Porphyria or acute toxin exposure are always difficult to diagnose, although a detailed history can help.
Diagnoses to consider in the differential of Guillain-Barré syndrome
Central nervous system disorders
Transverse myelitis
Neuromyelitis optica
Brainstem stroke
Cord tumour
Peripheral disorders
Systemic or peripheral nerve vasculitis
Hypokalaemia
Polymyositis/dermatomysositis
Porphyria
Toxins (eg lead, hydrocarbons)
Botulism
Myasthenia
IS THERE ANY VALUE IN RE-TREATMENT?
Let us assume that we are certain of the diagnosis and the patient has not responded to IVIg, the value of which in GBS has been established by a number of clinical trials;2 so we should feel reasonably secure that we have given the correct first line treatment. Many neurologists would give a second course of IVIg in this situation and this is certainly reasonable. However, although both IVIg and plasma exchange produce significant shortening of the time taken to recover, no randomised clinical trial has so far addressed the value of re-treatment. A Dutch trial of a second course of IVIg in patients not responding to the first course has been proposed (Hughes R, personal communication). Trials in GBS have become very much more difficult to do because of the widespread use of IVIg in small local hospitals so that single units cannot mount a trial alone, and large multicentre trials are very expensive.
Lack of response to IVIg will of course occur in a significant number of patients and is entirely consistent with the randomised trials which simply confirm the statistical “on average” benefit of treatment of the population. Furthermore, an apparent lack of response to IVIg is to be expected in some patients who may still go on to benefit from treatment. Consider the figure to illustrate this.
{kind=link}
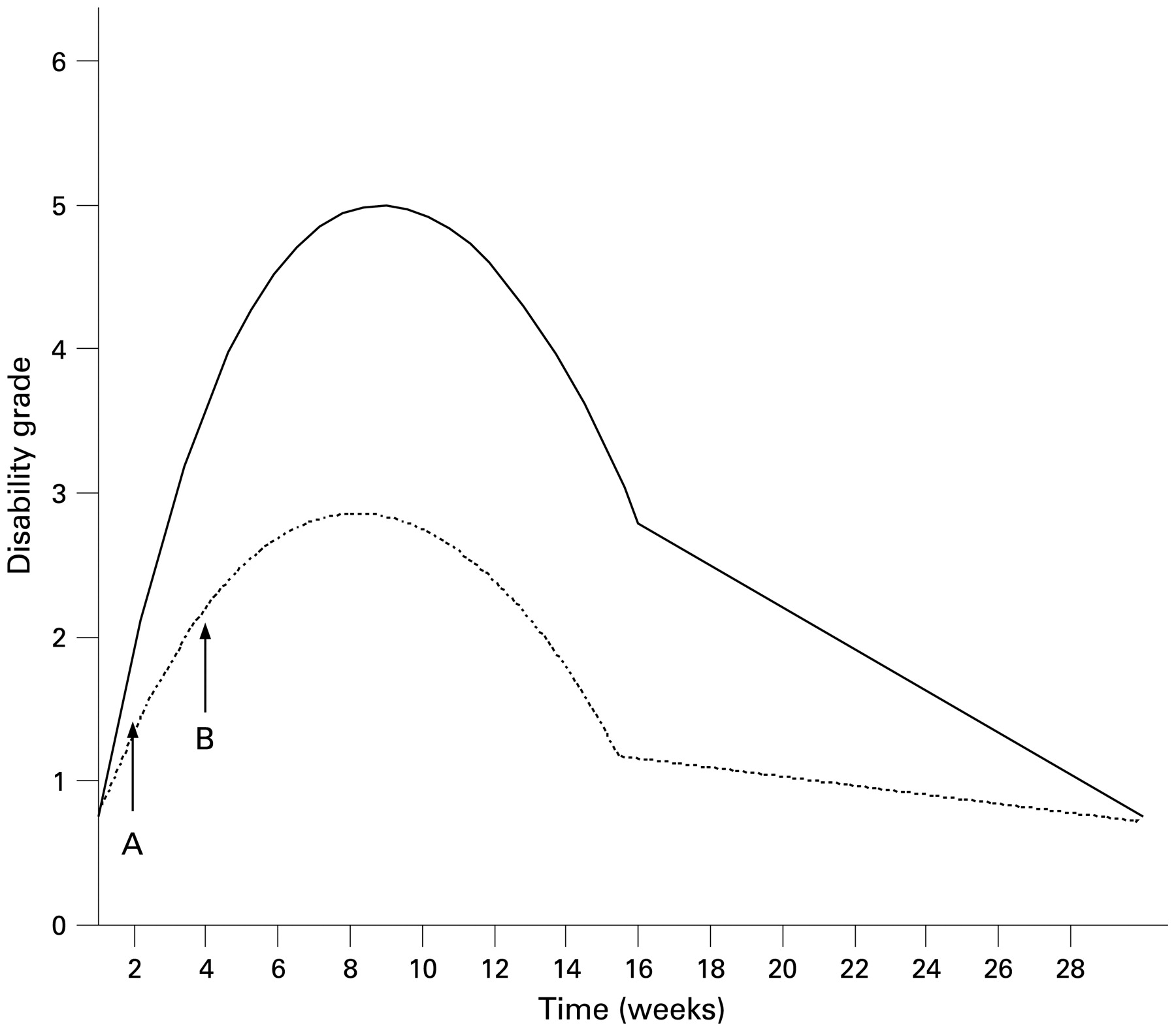
Hypothetical course of an attack of Guillain-Barré syndrome. Change in disability grade over weeks.
In the figure the response of a patient with severe GBS is charted. He receives IVIg within 24 hours of admission at point A and the dotted line depicts his progress compared to a supposed untreated patient (continuous line). Both patients eventually reach grade 1 of the most commonly used disability scale but the treated patient has a path with a lower trajectory and a more rapid recovery. At point B both patients will have shown some deterioration, even the treated patient, but he can clearly be seen to have responded to treatment—in the long run.
WHAT ABOUT THE PATIENT WHO RESPONDS AND THEN RELAPSES?
The other common scenario is the patient who responds to IVIg but then appears to deteriorate at a later date. Should these patients be retreated? About 3% of patients with GBS will turn out to have a more chronic disease which in time will fulfil the diagnostic criteria for chronic inflammatory demyelinating polyradiculoneuropathy (CIDP). Such patients would be expected to relapse and may eventually need treatment with corticosteroids or recurrent doses of IVIg. Recognition of these patients is difficult and I usually allow at least one relapse in the first two months before labelling a patient as CIDP.
In a recent randomised trial a significant deterioration of more than one clinical grade was considered by consensus, a reasonable threshold for giving a second course of IVIg. But what is the evidence that more IVIg is any better than waiting for spontaneous improvement? There is some weak evidence that a higher dose of IVIg is a little better than a lower dose3 and therefore one could argue that some patients may require more IVIg to stop the immune process than others. Consistent with the hypothesis that more IVIg might help in these cases, is the observation that some patients who show a good response to IVIg can have a relapse at about six weeks after treatment, which is recognised in the literature as a “treatment related fluctuation”.4 This is assumed to reflect the therapeutic effect of the IVIg wearing off. Anecdotal data support the treatment of these patients with a further course of IVIg.5 This is costly and associated with a further risk of IVIg-related complications, which rarely includes both renal failure and stroke. We clearly need further randomised trials to guide practice.
WHAT ABOUT PLASMA EXCHANGE IF THE PATIENT FAILS TO RESPOND TO IVIG?
The multicentre trial comparing treatment of GBS with plasma exchange followed by IVIg failed to find a significant advantage over IVIg or plasma exchange alone.6 There was however a slight trend towards a better outcome from the combined treatment and therefore some have argued that it is more rational to treat with plasma exchange if the IVIg fails to produce a documented improvement rather than repeat the IVIg. But there is of course the inevitable consequence of washing out the IVIg still present in the blood which is at the very least undesirable and some would argue illogical. Furthermore, plasma exchange has more complications than IVIg even though it was well tolerated in clinical trials; it is also more complex and therefore difficult to deliver to sick patients, especially if they have prominent autonomic failure, which is not uncommon in severe GBS.
WHAT DO I DO?
In practice I usually try and wait for improvement unless there is clear evidence of either continuing deterioration of one disability grade two weeks after treatment, or a relapse of this severity. If this occurs I re-treat with a further course of 0.4 g/kg of IVIg per day for a further five days. (I accept that at present there is no formal evidence but this may come in time!) If the patient still does not improve then I reconsider the diagnosis. I have occasionally gone on to treat such patients with plasma exchange. There is no doubt that some patients with CIDP do respond to plasma exchange and not to IVIg and by analogy this might apply to GBS as well. Unfortunately the time window for effective treatment of GBS may be too short for several attempts at treatment.
Practice points
IVIg 0.4 gm/kg per day for 5 days is the standard treatment for GBS.
A small percentage of patients with GBS will develop CIDP with progressive deterioration or relapses.
Treatment-related fluctuation leading to a deterioration of one grade usually responds to re-treatment with the same regime of IVIg.
Patients who appear initially not to respond to IVIg may still benefit from that treatment as measured by the time taken to recover.
Some patients who fail to respond may benefit from a second course of IVIg, or plasma exchange.
Acknowledgments
This article was reviewed by Hugh Willison, Glasgow, UK.
Linked Articles
- Editor’s choice
Other content recommended for you
- Original research: Second IVIg course in Guillain-Barré syndrome with poor prognosis: the non-randomised ISID study
- Treatment dilemmas in Guillain-Barré syndrome
- What’s new in Guillain-Barré syndrome?
- Chronic inflammatory demyelinating polyradiculoneuropathy in solid organ transplant recipients: a prospective study
- Diagnosis and treatment in inflammatory neuropathies
- Oligoclonal IgG bands in chronic inflammatory polyradiculoneuropathies
- CIDP: mimics and chameleons
- Management of children with Guillain-Barré syndrome
- CSF sphingomyelin: a new biomarker of demyelination in the diagnosis and management of CIDP and GBS
- Chronic inflammatory demyelinating polyradiculoneuropathy: search for factors associated with treatment dependence or successful withdrawal