Article Text

Abstract
People with Parkinson's disease have limited brain reserves of endogenous dopamine; thus, their medications must not be omitted or delayed as this may lead to a significant drop in brain dopamine levels. This has two main clinical consequences: first, a deterioration in disease control, with distressing symptoms such as tremor, pain, rigidity, dysphagia and immobility, and second, an increased risk of developing the life-threatening complication of neuroleptic malignant-like syndrome. Common reasons for people with Parkinson's disease being unable to take their oral medications are neurogenic dysphagia from progressive disease or concurrent illness, gastroenteritis, iatrogenic ‘nil by mouth’ status especially perioperatively, and impaired consciousness level. Here we outline alternative methods to give dopaminergic drugs in the acute setting to people with Parkinson's disease who cannot take their usual oral treatment, namely using dispersible preparations in thickened fluids, an enteral tube, a transdermal patch or subcutaneous injections.
- PARKINSON-S DISEASE
- DYSPHAGIA
- NEUROPHARMACOLOGY
- MOVEMENT DISORDERS
- PHARMACOLOGY
Statistics from Altmetric.com
Introduction
Parkinson's disease brain pathology is characterised by neuronal degeneration and Lewy body deposition. This pathological process begins about 7 years before the classical motor signs of Parkinson's disease—bradykinesia, tremor and rigidity—manifest. Approximately 30% of dopaminergic neurones are still functional by the time Parkinson's disease is clinically diagnosed and neuronal cell loss continues inexorably throughout the course of the disease. Consequently people with Parkinson's disease have very limited reserves of endogenous dopamine.
The mechanism of action of nearly all the drugs used to treat Parkinson's disease is via stimulation of the remaining dopaminergic neurones in the brain. This may be through delivering the dopamine precursor (levodopa), by directly activating the dopamine receptors with dopamine agonists, or by using enzyme inhibitors to slow the metabolism of dopamine or levodopa. We use generic drug names throughout this article and outline their brand names in the appendix.
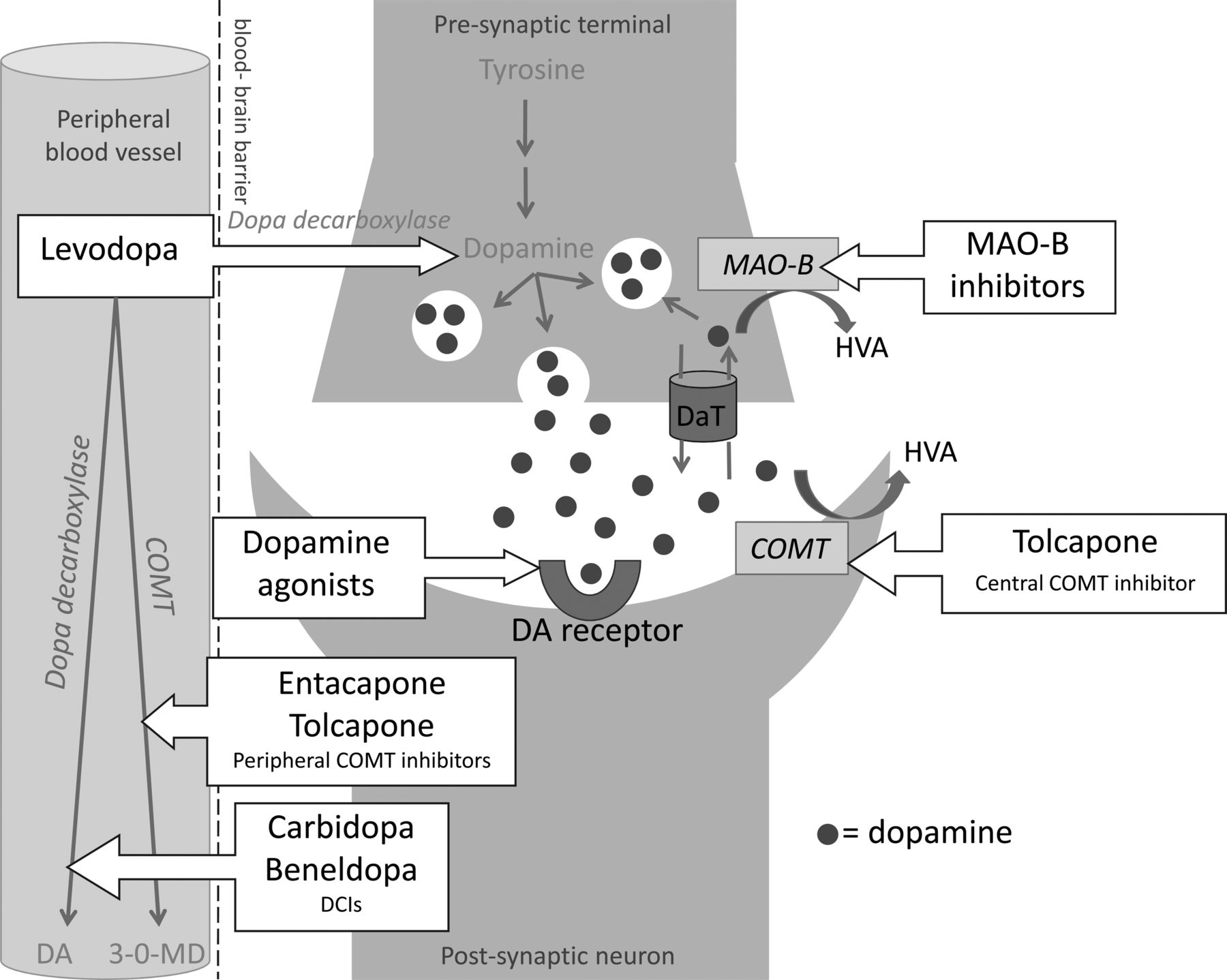
Levodopa is the main component in co-careldopa, co-beneldopa and carbidopa/levodopa/entacapone. Commonly used dopamine agonists include ropinirole, pramipexole and rotigotine. The enzyme inhibitor drugs have several actions but all impede the breakdown of levodopa or dopamine and comprise dopa decarboxylase inhibitors for example, carbidopa and benserazide, catechol-O-methyltransferase inhibitors, for example, entacapone and tolcapone, and monoamine-oxidase-B inhibitors, for example, selegiline and rasagiline (figure 1).

Dopaminergic neurones are activated through a mechanism of dopamine (DA) being released from vesicles at the presynaptic terminal, crossing the synaptic cleft and then binding to postsynaptic dopamine receptors. Excess dopamine is metabolised by monoamine-oxidase-B (MAO-B) at the presynaptic terminal, after first being taken up by the dopamine active transporter (DaT), and also via catechol-O-methyltransferase (COMT) at the postsynaptic terminal. Levodopa, a dopamine precursor that can cross the blood–brain barrier, thus increases the amount of dopamine released at the presynaptic terminal, whereas dopamine agonists directly stimulate the postsynaptic dopamine receptors. MAO-B inhibitors and the COMT inhibitor tolcapone increase dopamine availability in the synaptic cleft by slowing down dopamine metabolism in the central nervous system. Dopa decarboxylase inhibitors (DCIs) and both COMT inhibitors (entacapone and tolcapone) reduce peripheral metabolism of levodopa, thus increasing the amount available to cross the blood–brain barrier, and reducing peripheral side effects. Note: This diagram outlines the main actions of Parkinson's disease drugs on dopaminergic neurones but is not exhaustive; most of these drugs have additional roles, especially the enzyme inhibitors on other neurotransmitters’ metabolism. HVA, homovanillic acid.
It is crucial that people with Parkinson's disease receive their medications regularly as omissions or significant delays will lead to a rapid reduction in dopaminergic stimulation. This has two main clinical consequences: first, control of their Parkinson's disease will deteriorate with the development of distressing symptoms such as tremor, pain, muscle stiffness and difficulties with walking, speech and swallowing. These in turn increase the risk of complications such as pressure sores, aspiration pneumonia and falls. Second, a significant drop in brain dopamine levels increases the risk of developing neuroleptic malignant-like syndrome (also known as Parkinsonism–hyperpyrexia syndrome). This life-threatening complication manifests as high fever and extreme muscle rigidity. Ultimately the muscles begin to break down, resulting in elevated serum creatine kinase and urinary myoglobin concentrations. Neuroleptic malignant-like syndrome is a medical emergency and may rapidly lead to renal failure, cardiac arrest and death. It requires prompt treatment with intravenous fluids, dopaminergic drugs and body cooling. Patients need careful monitoring in a high dependency unit and may need muscle relaxants such as dantrolene sodium, although their role remains uncertain. Both these outcomes—Parkinson's disease complications and neuroleptic malignant-like syndrome—are entirely preventable if clinicians recognise the importance of, and actively pursue, regular dopaminergic stimulation in patients with Parkinson's disease. In other words, people with Parkinson's disease need their usual oral treatment regularly and on time, and if this is not possible, they must have an alternative method to receive an equivalent therapeutic dose (box 1).
Alternative methods of giving dopaminergic medications
There are four common alternative methods to consider if a person with Parkinson's disease cannot take their usual oral medications:
dispersible preparations±thickened fluids
enteral tube
transdermal patch
subcutaneous injection.
We discuss each in turn below. The dose conversion rates used are based on an excellent review paper by Tomlinson et al1 and allow for a similar degree of dopaminergic stimulation across a range of different drugs. Deep brain stimulation surgery and carbidopa/levodopa enteral gel are alternative long-term methods for maintaining dopaminergic stimulation but we do not discuss these further here as we aim to focus on acute management options.
Dispersible preparations
Levodopa
Levodopa is the most potent oral medication used in Parkinson's disease; significant delays or dose reductions are particularly likely to bring about symptoms of reduced dopaminergic stimulation. If the patient cannot swallow tablets but can manage fluids (including thickened fluids), convert their usual levodopa-containing medications to an equivalent dose of ‘co-beneldopa dispersible’ using the conversion rates outlined below:
Immediate release ‘levodopa and dopa-decarboxylase inhibitor’
=1: 1 conversion (of levodopa dose) to co-beneldopa dispersible.
For example,
co-careldopa  =50 mg levodopa;
=50 mg levodopa;
so, co-careldopa 12.5 mg/50 mg→co-beneldopa dispersible 12.5 mg/50 mg
The bioavailability of levodopa from controlled-release preparations is slightly lower than from immediate release levodopa but we recommend giving a 1:1 conversion rate in the acute setting to avoid a sudden drop in dopaminergic stimulation and then seek advice from pharmacy as slight reductions may be needed beyond the first 24 h of therapy.
Carbidopa/levodopa/entacapone contains the same active constituents as co-careldopa, plus a catechol-O-methyltransferase inhibitor called entacapone, which further increases the bioavailability of levodopa (figure 1). Although carbidopa/levodopa/entacapone is only licensed as whole tablets given orally, we have often recommended crushing and dispersing the tablets in 15 mL of water to minimise the number of drug substitutions; see ‘Prescribing drugs off-licence’ section. Alternatively, an equivalent co-beneldopa dispersible dose may be calculated as follows:
Carbidopa/levodopa/entacapone
=1:1.3 conversion (of levodopa dose) to co-beneldopa dispersible
For example:
carbidopa/levodopa/entacapone  =150 mg levodopa;
=150 mg levodopa;
so, 1.3×150=195 mg→*200 mg co-beneldopa dispersible
*Since co-beneldopa dispersible only comes as 12.5 mg/50 mg and 25 mg/100 mg doses, 195 mg levodopa will need to be given as two of the 50 mg/100 mg tablets or four of the 12.5 mg/50 mg tablets, that is, round up the levodopa dose to the nearest 50 mg.
Dopamine agonists
Pramipexole and ropinirole are the most commonly used oral dopamine agonists and there are immediate release (given three times per day) and modified release (given once daily) versions of each. Immediate release pramipexole may be crushed and dispersed in 15 mL of water and immediate release ropinirole will disperse in 15 mL of water without being crushed. These dispersions may then be added to thickened fluids if necessary.
The once daily, modified release versions of pramipexole and ropinirole must not be crushed or added to water. If patients are taking these drugs, the modified release dose will first need to be split into three immediate release pramipexole or ropinirole doses per day. Each dose of immediate release pramipexole or immediate release ropinirole can then be dispersed in 15 mL of water as outlined above.
Enteral tube
If a patient cannot safely swallow thickened fluids, they may need a nasogastric tube to receive their usual oral medications, using the conversion rates outlined above. If the patient's swallowing remains significantly impaired in the long-term, it is worth considering a percutaneous endoscopic gastrostomy tube.2 ,3
Although carbidopa/levodopa/entacapone and immediate release pramipexole and ropinirole are not licensed for use with enteral systems, we have often done so (after first crushing and dispersing the tablets in 15 mL water)—see box 1—and found this helps to keep the patient's regimen as stable as possible, especially when patients need a short period of drug administration via nasogastric tube; see ‘Prescribing drugs off-licence’ and ‘Choosing an alternative method of drug administration’ sections for further discussion.
Transdermal patch
If a patient with Parkinson's disease is nil by mouth, nil by enteral tube (eg, perioperatively) or likely to have problems absorbing drugs via the gastrointestinal tract, a useful way of continuing dopaminergic stimulation is by a transdermal patch that administers the dopamine agonist, rotigotine; see box 1. The patch may also help patients with impaired swallowing, as an alternative to using dispersible preparations of levodopa or dopamine agonists in thickened fluids or via an enteral tube.
Case study
A 64-year-old woman, who had been diagnosed with Parkinson's disease five years previously, underwent a subtotal gastrectomy for adenocarcinoma of the stomach. Six weeks prior to the surgery a nasojejunal tube had been placed because she was not meeting her nutritional needs and was losing weight. Her Parkinson's was well controlled on dispersible co-careldopa 25mg/100mg four times per day and pramipexole salt 0.875mg three times per day; both drugs were given via the nasojejunal tube, the latter crushed and dispersed in water before delivery. Immediately before surgery the medication was replaced with rotigotine 22mg/24 hours, applied as two 8mg patches, and one 6mg patch every 24 hours. She made an uneventful recovery from the surgery and her Parkinson's disease remained relatively well controlled throughout the post-operative phase. Six days after the operation and having been established on oral feeding she was able to return to taking the oral medication. She was discharged home and was very well, three days later.
Rotigotine patches are available in 2 mg/24 h, 4 mg/24 h, 6 mg/24 h and 8 mg/24 h doses. The maximum licensed dose of rotigotine is 16 mg/24 h. The patches must not be cut to achieve the correct dose but rather the nearest patch dose that provides an equivalent level of dopaminergic stimulation should be chosen. Figure 2 outlines the method of calculating an equivalent rotigotine patch for levodopa-containing drugs and oral dopamine agonists. Table 1 summarises the conversion rates for commonly used doses of dopamine agonists.4
Conversion of pramipexole and ropinirole doses to rotigotine patches

{kind=link}
{kind=link}
Flow chart demonstrating how to convert multiple different drug class doses into an equivalent daily rotigotine patch dose.
Due to the confines of the rotigotine patch dosages, it is not always possible to give the exact equivalent dose and a decision needs to be made as to whether to round the dose up or down. We discuss below some of the clinical issues to consider when making this decision. Whichever patch dose is ultimately chosen, it is important to monitor how the patient responds and to tailor further doses accordingly—so if there are side effects of too much dopaminergic stimulation such as confusion and hallucinations, the dose may need to be reduced, and if there is an increase in Parkinson's disease signs such as rigidity and tremor, the dose may need to be increased. This principle extends to all the drug classes when calculating equivalent doses and ongoing monitoring is fundamental to achieving the best clinical outcome.
As a rule of thumb, if the daily levodopa dose is over 500 mg, the patient is likely to need a higher dose of rotigotine patch than the maximum licensed dose of 16 mg/24 h. In this circumstance additional drugs may be given via an enteral tube or if this is not feasible, then consider subcutaneous apomorphine. Alternatively, a clinician may decide to prescribe doses of rotigotine higher than 16 mg/24 h to give an equivalent dose for the usual oral medications (see box 2). We discuss this option further in the ‘Prescribing drugs off-licence’ section.
Subcutaneous injection
Apomorphine, a potent dopamine agonist, may be given via subcutaneous injection under specialist supervision if the methods described above are not suitable, or when a rapid response is required. If a patient with Parkinson's disease is admitted with an apomorphine pump already in situ it is very important not to stop or alter pump settings without seeking advice from the on-call neurologist or pharmacist. There is also a 24-h telephone helplinei provided by the manufacturer of apomorphine that will assist patients and clinicians on how to deal with the practicalities of the pump.
Prescribing drugs off-licence
Not infrequently we, as clinicians managing Parkinson's disease, face a dilemma regarding whether to prescribe drugs off-licence. This may be necessary to maintain a level of dopaminergic stimulation equivalent to the usual oral regimen and hence reduce the risk of Parkinson's disease complications and neuroleptic malignant-like syndrome. For example, clinicians may need to consider using rotigotine patch doses higher than 16 mg/24 h (see box 2) or giving crushed immediate release pramipexole via an enteral tube, both of which are not licensed. In these scenarios, the prescriber needs to recognise that this would be unlicensed and hence to take full responsibility for the prescription. However, nurses and pharmacists involved in the care of the patient may share some of the responsibility. Our advice is intended as a guide only and not as an authority for the unlicensed use or administration of medicines discussed. Therefore, individual practitioners need to be familiar with or to seek advice from a specialist pharmacist with respect to the legal and ethical aspects of the use and administration of unlicensed medicines. Ultimately the clinical management decision aims to minimise the risk of adverse effects, from undertreatment of Parkinson's disease and also the potential adverse effects of using drugs off-licence, while recognising that further clinical experience is still required on the use of Parkinson's disease drugs off-licence.
Choosing an alternative method of drug administration
The method chosen depends upon the individual patient and their circumstances. There is rarely just ‘one correct method’ and the clinician needs to weigh up the potential risks and benefits of each approach. There are a few overarching guiding principles such as: it is generally best to choose the least invasive method and if appropriate, to revert to the patient's usual oral regimen as soon as possible. It is also crucial to choose a method of drug administration fairly swiftly, to prevent significant (>4 h) dose delays; so, for example if there were difficulties passing a nasogastric tube it would be advisable to apply a rotigotine patch, at least as an interim measure rather than waiting for another clinician to attempt passing the nasogastric tube if this meant several doses would be missed. While we cannot discuss every indication in this article, we will now outline a few general factors to consider when choosing which method to use.
First, it is crucial to explore the reasons why the person with Parkinson's disease cannot take their usual oral medications. Common systemic causes for deteriorating swallowing function in persons with Parkinson's disease include constipation and infections; these should be actively sought and treated. It is important always to check the drug chart in any patient with Parkinson's disease who has recently developed dysphagia because missed doses may simply be the sole cause; thus a short course of their usual medications given via a nasogastric tube (or in thickened fluids if this is safe) may quickly restore swallowing function. Similarly, check that the patient has not taken dopamine antagonist medications recently (table 2) as stopping these may quickly return swallowing to normal. In the case of gastroenteritis, where vomiting precludes ingestion and diarrhoea disrupts absorption, it is probably easiest to substitute the oral medications with an equivalent rotigotine patch. However, if patients have had a known adverse reaction to dopamine agonists, it is reasonable to consider a short course of antiemetic and/or antidiarrhoeal (eg, loperamide) drugs in order to maximise the bioavailability of their usual oral medications. This should be used cautiously—carefully observing for signs of reduced dopaminergic stimulation—and not at all if there is bloody diarrhoea.
Drugs to avoid in patients with Parkinson's disease
Alternatively, if a patient's swallowing has gradually deteriorated over many months despite optimising the drug regimen, it is worth considering a long-term non-oral method such as a transdermal patch or percutaneous endoscopic gastrostomy. In any scenario where there is persistent dysphagia, referral to a speech and language therapist is recommended. Similarly it is useful to plan ahead when advising on preoperative patients undergoing abdominal surgery, as a ‘nil by mouth’ status may quickly become a ‘nil by bowel’ status postoperatively and hence the first two methods would be less appropriate.
Second, it is important to consider the adverse-effect profiles of different drug classes and how these may relate to the individual patient. For example, dopamine agonists have an increased risk of hallucinations compared with levodopa, especially in older patients and those with delirium or dementia. Conversely, some patients are very sensitive to the hypotensive effect of pulsatile levodopa-containing drugs and may be better suited to the continuous stimulation offered by a transdermal rotigotine patch. It is helpful to find out which drugs a patient has previously not tolerated and avoid drugs in the same class if possible. Similarly it is often sensible to make as few drug switches as possible, especially if the current oral regimen is well tolerated. For example, for a patient taking levodopa, we find that it is probably best in terms of limiting drug-related adverse effects to give dispersible levodopa in thickened fluids or via nasogastric tube, rather than introduce a new dopamine agonist.
Parkinson's disease drugs that can be omitted in the acute setting
Finally, while making every effort to avoid abruptly stopping any Parkinson's disease medications, it is usually safe to omit the following drugs in the acute setting: rasagiline, selegiline, amantadine, entacapone and tolcapone. It is important, though, to be alert to new symptoms that could be drug withdrawal effects (eg, rapid withdrawal of amantadine occasionally causes an acute dystonic reaction) and to seek pharmacy advice within 48 h.
Key points
People with Parkinson's disease need regular dopaminergic medication to prevent their symptoms deteriorating and to avoid neuroleptic malignant-like syndrome.
People with Parkinson's disease have limited endogenous reserves of dopamine: rapid withdrawal, significant delay or missed doses lead to a drop in dopaminergic stimulation.
Reduced dopaminergic stimulation in Parkinson's disease can lead to dysphagia—so act quickly to avoid the need for enteral administration.
Oral Parkinson's disease drugs may be converted to an equivalent dose of a dispersible preparation, transdermal patch or subcutaneous injection, or may be given via an enteral tube.
Consider the legal and ethical aspects of using unlicensed medicines in people with Parkinson's disease.
Case study: worked example to show the conversion rate calculation
Step 1: Total doses in a 24-h period: co-careldopa 25 mg/100 mg four times a day=400 mg levodopa, pramipexole salt 0.875 mg three times a day=2.625 mg pramipexole salt
Step 2: Equivalent rotigotine dose for levodopa=400 mg×0.033=13.2 mg Equivalent rotigotine dose for pramipexole=2.625 mg×3.3=8.75 mg
Step 3: Total rotigotine daily dose: 13.2 mg+8.75 mg=21.9 mg In this particular case, we made a clinical decision to prescribe an unlicensed dose of rotigotine—22 mg in 24 h, using two 8 mg patches plus one 6 mg patch. We discuss further the prescribing of drugs off-licence below.
Acknowledgments
The authors thank the patient described in the case study for consent to its publication.
Appendix: Generic and equivalent brand drug names
Co-careldopa (Sinemet); co-beneldopa (Madopar); controlled release cocareldopa (Sinemet CR, Half Sinemet CR); controlled release co-beneldopa (Madopar CR); carbidopa/levodopa/entacapone (Stalevo, Sastravi); carbidopa/levodopa enteral gel (Duodopa); ropinirole (Requip); pramipexole (Mirapexin); modified release ropinirole (Requip XL); modified release pramipexole (Mirapexin PR); rotigotine (Neupro); apomorphine (Apo-go); entacapone (Comtess); tolcapone (Tasmar); selegiline (Zelapar, Eldepryl); rasagaline (Azilect); amantadine (Symmetrel).
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
- Data supplement 1 - Online supplement
Footnotes
Twitter Follow Jane Alty @janealty1 and Jeremy Robson at @jezzarobson
Contributors JA wrote the first draft of the paper, coordinated incorporation of the other authors’ edits into second and third drafts, produced figures 1 and 2 and submitted the paper. JR reviewed all drafts of the paper and significantly edited table 1. PD-C reviewed all drafts of the paper, produced tables 1 and 2, and obtained patient consent for the case study. SJ reviewed all drafts of the paper and wrote the case study.
Competing interests JA is employed by Leeds Teaching Hospitals NHS Trust. She has previously been awarded grants by Ipsen, UCB Foundation and Parkinson's UK. She has stock ownership in Dr Carsten Grimm Medical Consultancy and Clear Sky Diagnostics. She receives royalties from Taylor & Francis Group for medical textbooks she has coauthored. JR is employed by Leeds Teaching Hospitals NHS Trust. PD-C is employed by Leeds Teaching Hospitals NHS Trust. She sits on advisory boards for Britannia, Apo-go pens and pumps. SJ is employed by Leeds Teaching Hospitals NHS Trust. He is a founder shareholder in Clear Sky Diagnostics, sits on advisory boards for Abbvie and GSK, has received honoraria from GE Healthcare, UCB, GSK, Orion and grants from Merz and Allergan.
Patient consent Obtained.
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Simon Lewis, Sydney, Australia.
↵i Apomorphine pump 24-hour helpline numbers: UK 0844 880 1327, Germany +49 172 670 0272, Holland +31 800 766 7463, Spain +34 91 657 2348.
Linked Articles
- Editors' commentary
Other content recommended for you
- Initial management of Parkinson’s disease
- Behavioural and trait changes in parkinsonian patients with impulse control disorder after switching from dopamine agonist to levodopa therapy: results of REIN-PD trial
- Emergency presentations of Parkinson's disease: early recognition and treatment are crucial for optimum outcome
- Emergencies and critical issues in Parkinson’s disease
- Impulse control disorder in patients with Parkinson's disease under dopamine agonist therapy: a multicentre study
- Dopamine agonists: their role in the treatment of Parkinson's disease
- Pharmacological treatment of Parkinson's disease
- Restless legs syndrome: pathophysiology and modern management
- Initial drug treatment in Parkinson’s disease
- Developments in the treatment of Parkinson's disease