Article Text

Abstract
Paraneoplastic neurological syndromes can be associated with the presence of onconeural antibodies. These antibodies are the result of an immune response against a tumour that is ectopically expressing a neuronal antigen. The ‘classical’ onconeural antibodies (anti-Hu, Yo, Ma2, CRMP-5, amphiphysin and Ri) are directed against intracellular antigens and are strongly associated with underlying malignancy. By contrast, onconeural antibodies directed against cell surface antigens (eg, anti-NMDA, VGKC, AChR) have a weaker tumour association. This article gives a practical overview of the tumour associations, and the neurological associations, of the onconeural antibodies. There is also guidance on how to investigate occult malignancy in antibody positive cases.
Statistics from Altmetric.com
Introduction
A paraneoplastic syndrome consists of symptoms attributable to a neoplasm that are not the direct result of any local or metastatic presence of the neoplastic cells. Paraneoplastic neurological syndromes are sometimes associated with the presence of autoreactive antibodies; serum assays for these paraneoplastic autoantibodies (also known as onconeural antibodies) are, therefore, commonly requested in neurological practice.
Classical versus non-classical paraneoplastic neurological syndromes
Paraneoplastic neurological disorders are generally subdivided according to Posner's classification (table 1).1 Certain syndromes are defined as ‘classical’ because their presence strongly suggests an underlying cancer. Other syndromes are defined as ‘non-classical’ because, although they are sometimes associated with cancer, more often they are not—for example, myasthenia gravis where most cases are autoimmune and not thymoma related.
Clinical features of the antibody associated paraneoplastic syndromes in adults
Well characterised onconeural antibodies
In 2002, an international panel reviewed all the reported onconeural antibodies and defined six (anti-Hu, Yo, Ma2, CRMP-5, amphiphysin and Ri) as being ‘well characterised’.2 Their recommendation was that a patient with a neurological presentation whose serum is positive for a well characterised onconeural antibody should be defined as having a definite paraneoplastic syndrome (and hence underlying neoplasia), regardless of whether or not the underlying neoplasm had been found. A patient with no ‘well characterised’ antibodies must have proven cancer to be diagnosed with a definite paraneoplastic neurological syndrome. Rigorous criteria had to be met before an antibody could be described as ‘well characterised’, including its unambiguous identification across different studies, a high number of reported antibody positive cases, low frequency in patients without cancer and good reliability of the laboratory assay.
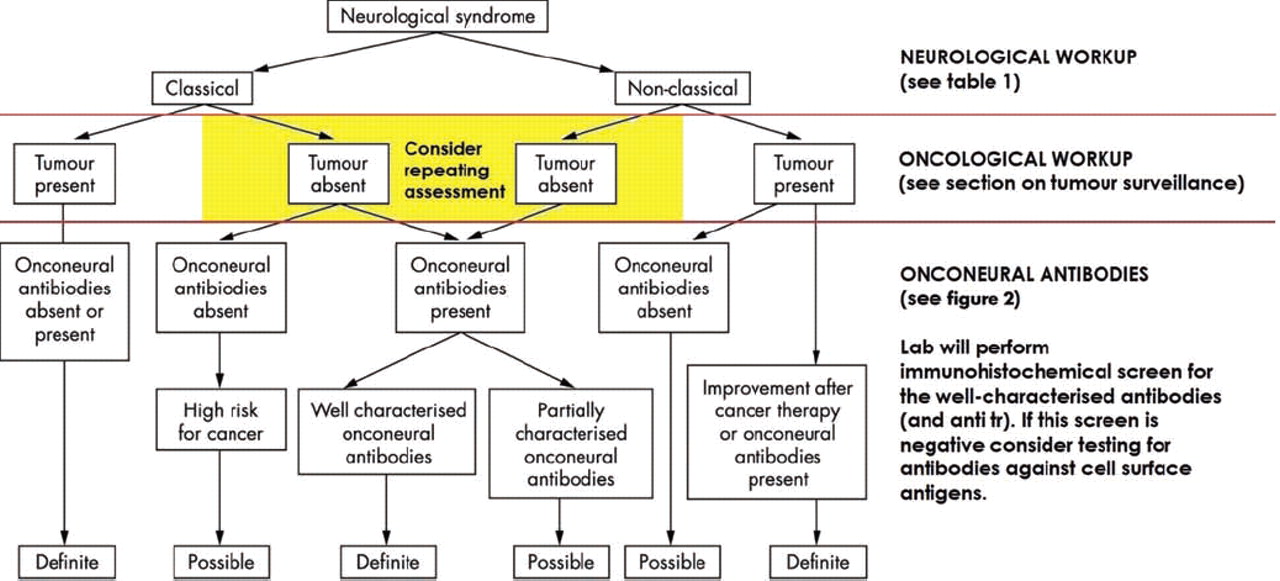
The panel also drew up diagnostic criteria for paraneoplastic neurological syndromes based on whether the syndrome was classical and whether the antibody was well characterised (table 2). The decision flow for the diagnosis of a paraneoplastic syndrome based on these criteria is shown in figure 1.

Decision pathway for the diagnosis of a paraneoplastic syndrome.2
Recommended diagnostic criteria for paraneoplastic neurological syndromes
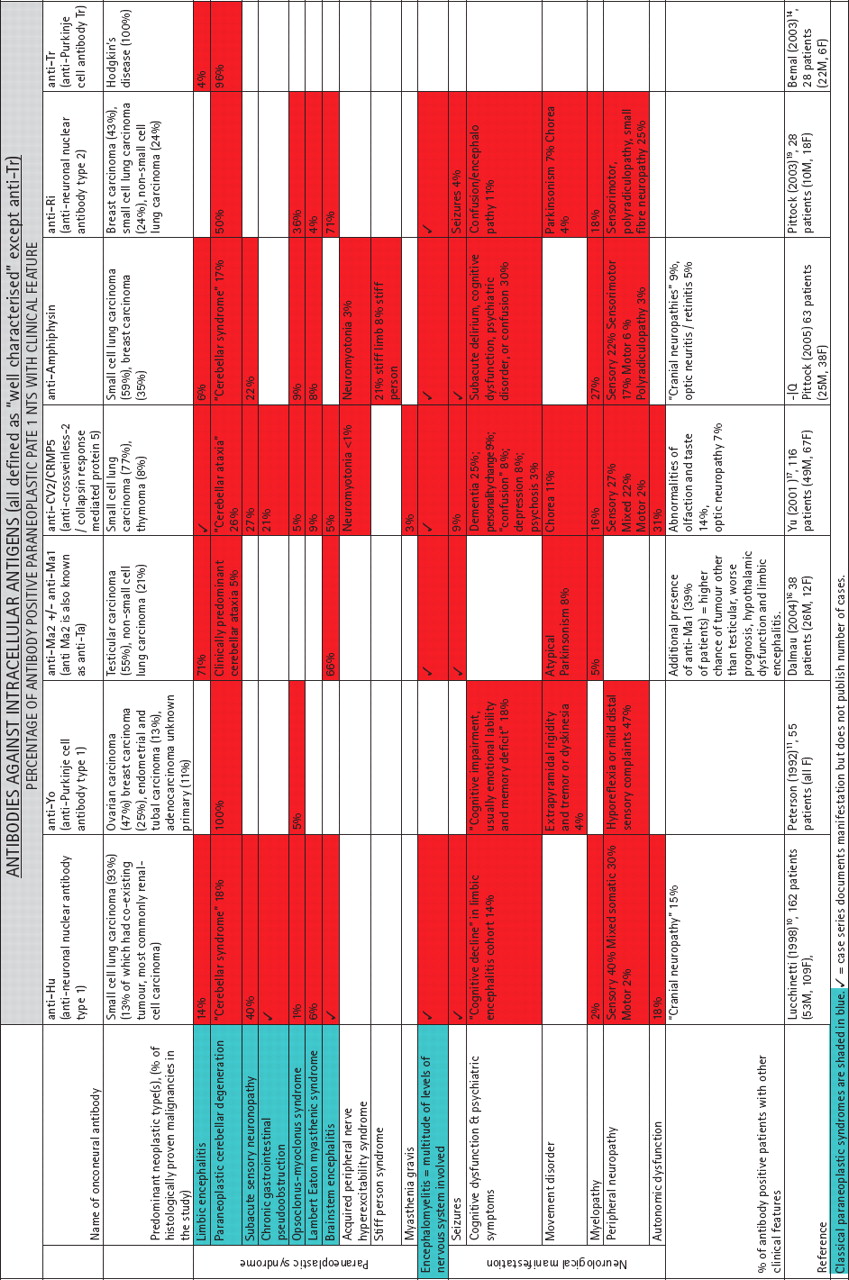
Figure 2 shows the well characterised onconeural and other onconeural antibodies for which large case series have been published. The overall frequency of the paraneoplastic neurological syndromes and other neurological manifestations are shown against each antibody, based on the data from the largest case series available for that antibody.


Clinical features and tumour associations of the paraneoplastic autoantibodies in adults.
Pathogenesis
The paraneoplastic antibodies have the same origin: an immune response directed against a tumour which is ectopically expressing a neuronal antigen. The resultant antibodies are then directed against antigens in the central and/or peripheral nervous systems. The classical paraneoplastic autoantibodies predict type of cancer much more accurately than the type of neurological syndrome.3 These antibodies, albeit at lower titres (eg, 1:1000), are also detectable in cancer without paraneoplastic neurological symptoms; for example. in small cell lung carcinoma (SCLC), the neoplasm most frequently responsible for paraneoplastic syndromes, there is a background 1:1000 titre anti-Hu positivity of 15% in patients without any paraneoplastic syndrome.4
The well characterised onconeural antibodies consistently demonstrate a characteristic immunofluorescence staining pattern when serum is applied to primate or rodent brain (figure 3). Laboratories will therefore screen using an immunohistochemical approach before confirming the individual antibodies using an immunoblot.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Two sections of rat cerebellum (×20 magnification), each immunoreacted with serum from a different patient (×200 dilution). Positive staining is brown. The serum used in (A) is Hu positive and in (B), Yo positive. Hu serum binds neuronal nuclei in the granular and molecular layer. Yo serum avidly binds Purkinje cell cytoplasm. GL, granular layer; ML, molecular layer.
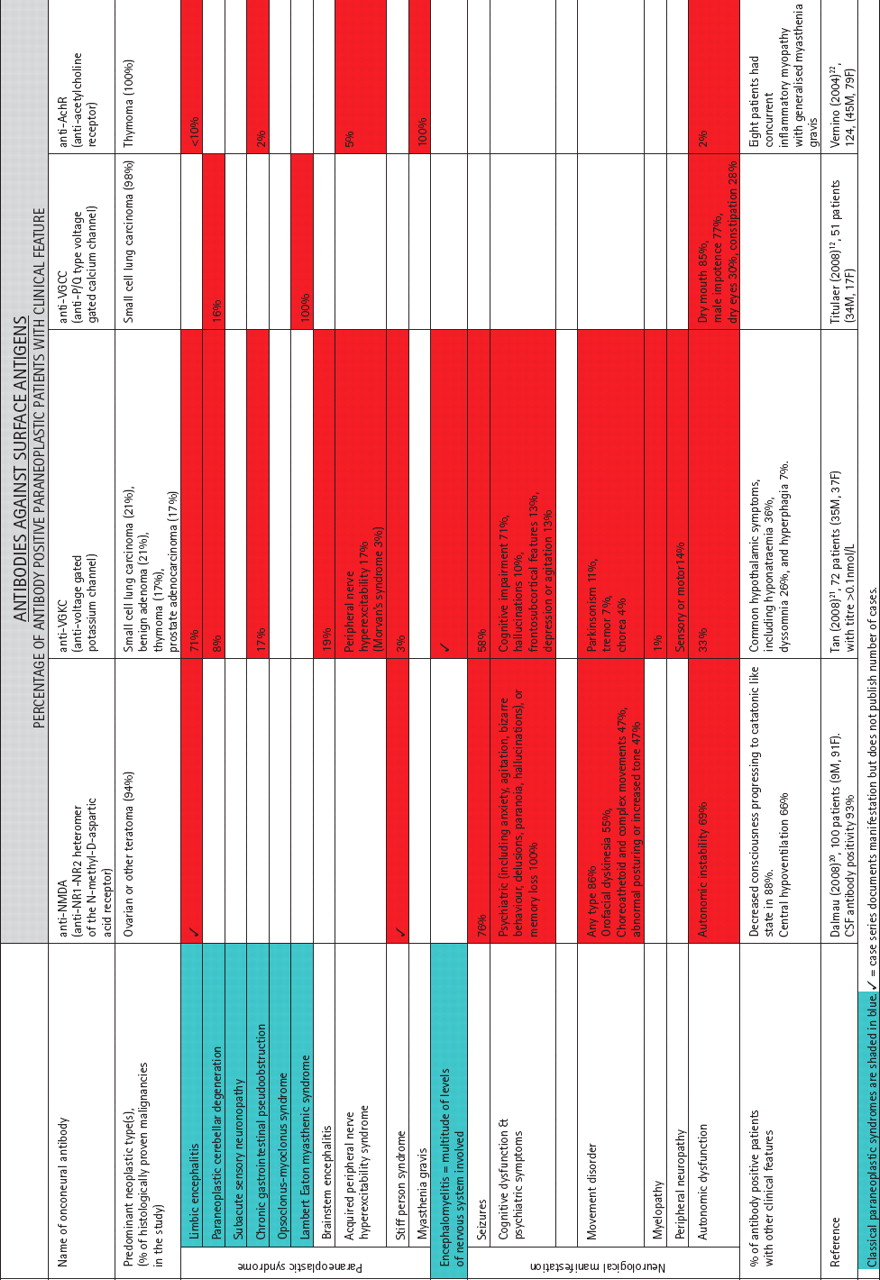
The binding of an antibody to a particular neural antigen on the exposed cellular structure of a fixed brain section does not indicate the mode of pathogenicity of the neurological syndrome; this varies. For example, anti-Hu is directed against nuclear antigens (a family of RNA binding proteins normally expressed in the nervous system); presumably these ectopically expressed nuclear antigens become externalised during the antitumour immune response. Antinuclear antibodies in general are not thought to be pathogenic5; for example, passive transfer of anti-Hu containing immunoglobulin G into animals does not induce disease.6 In anti-Hu syndromes the neuropathology is thought to be cell mediated7 and the antibody is merely an immunological accompaniment. In contrast, the onconeural antibodies directed against cell surface antigens such as anti-NMDA and anti-VGKC are themselves disease mediating. This type of onconeural antibody is associated with an autoimmune, non-paraneoplastic neurological syndrome in a significant proportion of cases (table 3).
Percentage of antibody positive patients without cancer
Often more than one onconeural antibody is found in association with a tumour; there is positivity of one or more additional paraneoplastic antibodies in 35–57% of cancer cases where an onconeural antibody is found. However, anti-Yo positivity is usually found on its own (91% of cases).3
New onconeural antibodies are discovered regularly. A recent example is antiglial nuclear antibody, in SCLC associated Lambert–Eaton myasthenic syndrome (LEMS). It was initially defined by immunoreaction to Bergmann glia of rat cerebellum. In 2007 the neuronal antigen was shown to be SOX (Sry-type high mobility group box), a neurodevelopmental transcription factor. SOX antibodies are found in 67% of patients with SCLC associated LEMS and are highly specific to the paraneoplastic form of LEMS, unlike the antivoltage gated calcium channel antibody. Currently SOX assays are available in the UK on a research basis only.
Investigation for occult malignancy
It should be emphasised that a definite or possible paraneoplastic syndrome can still be diagnosed even in a patient with negative assays for all the known onconeural antibodies (see diagnostic criteria, table 2). A patient with suspicious neurological symptoms who is antibody negative should still be investigated thoroughly for occult malignancy (the common malignancies to look for are shown in table 1).
In antibody positive cases, investigation should first focus on detecting the most likely tumour, always guided by careful history taking and examination. With the exception of pelvic examination, the neurologist should be able to competently perform all aspects of an initial physical examination.
Patients suspected of paraneoplastic disease should have their history, examination and investigations repeated at frequent intervals for at least 5 years
Depending on the positive antibody(s) in question, investigation will usually begin with blood tests such as full blood count, urea and electrolytes, liver function and bone function tests. Appropriate radiological examinations are CT chest–abdomen–pelvis followed by fluorodeoxyglucose–positron emission tomography.8
Tumour markers relevant to paraneoplastic neurological syndromes are:
α-fetoprotein and β human chorionic gonadotrophin in suspected germ cell/testicular tumours
CA125 in suspected ovarian cancer
prostate specific antigen in suspected prostatic cancer.
A negative result does not exclude malignancy. A positive result provides some indication of the likelihood of a particular malignancy but is not diagnostic; for example, CA125 is raised in other conditions such as heart failure and diabetes. The National Academy of Clinical Biochemistry does not recommend the use of CA15-3 for breast cancer diagnosis (it only has a role in monitoring treatment and detecting recurrence) or carcinoembryonic antigen for colorectal cancer because these are of low diagnostic sensitivity for early stage disease and low specificity for their respective tumours.9
It is essential to involve appropriate specialists at the diagnostic stage because investigations will usually then take a more specialist and invasive course. In the case of suspected breast cancer, the appropriate initial investigation is mammography; for suspected colorectal cancer it is colonoscopy. Often an area of suspicion will warrant biopsy and sometimes initial negative investigations will require invasive tests—for example, an anti-Hu positive patient requires bronchoscopy even if the CT chest is normal. There may be more than one tumour, particularly in anti-Hu positive patients, and discovery of an unexpected tumour warrants continued investigation for a more commonly expected underlying malignancy.2
In the large onconeural antibody studies, the neurological syndrome preceded the tumour diagnosis in most patients and the latency of diagnosis varied from 3 weeks to 8 years.10 11 The panel responsible for the diagnostic criteria (table 1) chose 5 years as the time span for continuing to pursue occult malignancy based on the vast majority of tumours declaring themselves within this interval.2 Therefore, patients suspected of paraneoplastic disease should have their history, examination and investigations repeated at frequent intervals for at least 5 years. There is no validated guidance on how frequently this assessment should take place. Ultimately the decision should be taken on a case by case basis and will depend on risk stratification for cancer (eg, age, lifestyle and family history).
With some paraneoplastic syndromes, knowing about the clinical features that associate with cancer can be helpful. For example, early onset thymomatous myasthenia gravis tends to be much more severe than autoimmune myasthenia in the same age group and usually presents with progressive generalised and oropharyngeal weakness rather than ocular weakness. In LEMS, a rapidly progressive disease, distal involvement, autonomic dysfunction and ataxia all point towards SCLC.12 In limbic encephalitis and opsoclonus–myoclonus syndrome, poor recovery with immunotherapy suggests underlying neoplasia.
A negative panel of paraneoplastic antibodies does not exclude malignancy sufficiently. However, the antibody panel is expanding with new discoveries in the field, and in the future it may be common to use combined antibodies in cancer screening. Recently, a study explored the collective use of SOX and Hu as a tumour marker for SCLC in 136 non-paraneoplastic patients4; an overall sensitivity of 43% was achieved, with no healthy controls or patients with polyneuropathy exhibiting SOX/Hu antibodies.
Treatment
Definitive treatment is directed towards the underlying tumour; the neurological syndrome may then stabilise and even improve. There is evidence in anti-Hu associated encephalomyelitis that early cancer treatment improves neurological outcome.13 Other syndromes in which tumour treatment is known to positively affect neurological outcome are: LEMS, myasthenia gravis, opsoclonus–myoclonus and stiff person syndrome. The Hodgkin's associated anti-Tr paraneoplastic cerebellar degeneration tends to improve with tumour therapy14 whereas anti-Yo paraneoplastic cerebellar degeneration does not usually improve.11
Practice points
A patient with a neurological syndrome whose serum is positive for a well characterised onconeural antibody should be diagnosed with a definite paraneoplastic syndrome (and hence underlying neoplasia).
The well characterised antibodies predict type of cancer much more accurately than the type of neurological syndrome; a positive result should prompt urgent oncology workup.
The paraneoplastic neurological syndrome precedes the tumour diagnosis in most patients and the tumour may take up to 5 years to become evident; regular follow-up and tumour surveillance is essential in suspected paraneoplastic cases.
Definitive treatment for paraneoplastic syndromes is directed towards the tumour but some antibodies against cell surface antigens are associated with a paraneoplastic neurological syndrome that responds well to immune therapy.
Often more than one paraneoplastic antibody is found in association with a tumour but a negative panel of all the currently available antibodies does not exclude an underlying malignancy with adequate sensitivity.
In general, immune therapies such as corticosteroids, plasma exchange and intravenous immunoglobulin are more likely to affect neurological outcome when the syndrome is caused by an antibody directed against a cell surface antigen (N-methyl-D-aspartic acid (NMDA), voltage gated potassium channel (VGKC), voltage gated calcium channel (VGCC), acetylcholine receptor (AChR)). Fortunately, immune therapy does not appear to prejudice the oncological outcome.15
Conclusion
Although paraneoplastic neurological syndromes are rare, their antibody associations are important because of the antibody's aetiological connection with the underlying tumour. The paraneoplastic autoantibody may lead the pathway to early recognition of the tumour, prompt treatment of which can sometimes improve the neurological outcome.
Acknowledgments
We thank Angela Vincent and Bethan Lang for reading the manuscript and for their helpful suggestions. This article was reviewed by Robin Grant, Edinburgh.
References
Footnotes
-
Provenance and peer review Commissioned; externally peer reviewed.
-
Competing interests None.
Other content recommended for you
- Republished: Which antibody and which cancer in which paraneoplastic syndromes?
- Central nervous system neuronal surface antibody associated syndromes: review and guidelines for recognition
- Paraneoplastic neurological syndromes: a practical approach to diagnosis and management
- Rhombencephalomyelitis due to possible paraneoplastic syndrome associated with Hodgkin’s lymphoma
- Opsoclonus-myoclonus paraneoplastic syndrome in nasopharyngeal carcinoma
- A rare case of long-term paraesthesia diagnosed as a paraneoplastic syndrome by anti-SOX1 antibody determination
- Recommended diagnostic criteria for paraneoplastic neurological syndromes
- Protein kinase Cγ autoimmunity in paraneoplastic cerebellar degeneration and non-small-cell lung cancer
- Delayed onset of a second paraneoplastic neurological syndrome in eight patients
- Anti-Yo paraneoplastic cerebellar degeneration in a patient with stage IV ovarian adenocarcinoma during bevacizumab maintenance therapy