Article Text

Abstract
Levodopa-induced motor complications of Parkinson's disease, including motor fluctuations and dyskinesias, become increasingly frequent as the disease progresses, and are often disabling. Oral and transdermal therapies have limited efficacy in controlling these problems. Advanced device-aided therapies, including continuous infusion of apomorphine, deep brain stimulation and levodopa-carbidopa intestinal gel can all ameliorate these complications. This review summarises the principles of each of these therapies, their modes of action, efficacy and adverse effects, and gives advice on timely identification of suitable patients and how to decide on the most appropriate therapy for a given patient.
- PARKINSON-S DISEASE
Statistics from Altmetric.com
Introduction
When appointed as a consultant neurologist in 2004, I set up a movement disorder clinic. Things seemed easy at first—I confidently diagnosed new patients with Parkinson's disease and started them on what I thought was the right treatment. Most responded and both they and I were pleased.
Eight years on, things are a bit different. I have learnt great respect for the principle that no two patients with Parkinson's disease are the same. Indeed, a few patients I diagnosed with Parkinson's turned out not to have it, a few others who did have Parkinson's have died, a few more have become demented and are in care homes, and still more have developed motor complications of levodopa therapy. Some of the motor complications are severe and have become resistant to medication tinkering. Some have gone on to receive one of the three main so-called ‘advanced therapies’:
-
apomorphine continuous subcutaneous infusion
-
functional neurosurgery/deep brain stimulation
-
continuous intrajejunal infusion of levodopa/carbidopa intestinal gel.
Some patients have done well, others less so. Did I make the right choices? I am interested in how to select patients for these. All are expensive, and not all are suitable for all advanced patients, and each can have serious complications. However, when you get it right, they can be life changing.
Geriatricians manage more patients with Parkinson's disease than neurologists in the UK, and there are wide variations in access to and experience of each treatment. Identifying patients who may benefit may be more difficult for a general neurologist in a busy general clinic than for a movement disorder neurologist in a tertiary specialist clinic. Some patients are referred much too late and others never get the opportunity.1 Therefore, my main aim is to help the generalist identify suitable patients for timely referral.
I will discuss the mechanisms underlying the development of motor complications, explain the technology and basic principles behind each of the three advanced treatments, present some evidence for and against each therapy, discuss how we should identify patients who might benefit from them, and conclude with advice on the selection of the right therapy for the right patient at the right time.
What are motor complications, and why do they occur?
A basic knowledge of the type and pathophysiology of motor complications in Parkinson's disease helps to understand the principles behind each of the three advanced therapies (boxes 1 and 2). Motor complications result from a complex interplay between the natural history and pathophysiology of the disease itself and the drugs we use to treat it. Normal humans and non-human primates do not develop these complications when receiving levodopa.
Motor complications
Motor fluctuations
-
Wearing-‘OFF’
-
Delayed ‘ON’ or no ‘ON’
-
‘ON’/'OFF’ fluctuations
Dyskinesias
-
Peak dose
-
‘Diphasic’
-
‘OFF’ period dystonia
Factors underlying the appearance of motor complications
Pharmacokinetic
-
Delayed gastric emptying
-
Amino acids competing for absorption
-
Short half-life of levodopa (c. 90 min)
Pharmacodynamic
-
Loss of presynaptic ‘buffering’ as nigrostriatal pathway degenerates
-
Plastic changes in postsynaptic receptor population
-
Changes in striatal gene transcription
In the ‘maintenance’ phase of Parkinson's disease, after diagnosis and starting treatment, most patients respond consistently to their medication, without gross fluctuations in motor symptom control at different times of the day or in relation to drug doses. Ironically, this is often called the ‘honeymoon’ period. As the condition advances, patients commonly develop one or both of:
-
Motor response fluctuations, including end-of-dose wearing-off, delayed ON and dose failures;
-
‘Dyskinesias’, most commonly generalised choreic or dance-like movements, usually related to peak plasma levodopa/extracellular central nervous system dopamine concentrations.
These complications define the onset of the ‘complex’ phase of the disease. They develop in about 10% of patients per year, the main risk factors being younger age at onset and higher dose of levodopa.2
Most people accept that levodopa therapy is more associated with motor complications than are dopamine agonists. However, as recently discussed in this journal, there is increasing dissent from this prejudice.3 In retrospect, in studies where patients with early Parkinson's disease were randomised to levodopa or a dopamine agonist, patients on dopamine agonists were found to be on overall lower equivalent doses of dopa agonists, and reported less motor benefit than those in the levodopa arms. Had patients on dopamine agonists taken equivalent doses, they may have had more motor benefit but also more dyskinesias. In open-label extensions of these studies, when patients taking dopamine agonists start levodopa, their rate of developing dyskinesia increases, and the overall proportion of patients with dyskinesia is ultimately very similar, regardless of the initial treatment.3 Although expert opinion remains ‘keep the dose of levodopa as low as possible for as long as possible’, levodopa should not be avoided; this advice may apply equally to dopamine agonists.
Whatever the true cause of motor complications, clinicians often fail to identify wearing-off, and their patients may equally be unprepared for it. One way to improve early detection of motor fluctuations is the wearing-off questionnaire.4 This can save time in a busy outpatient clinic, and I would recommend giving this and other questionnaires to patients beforehand.
The mechanisms contributing to the development and persistence of motor complications include delayed gastric emptying, variable levodopa absorption and the short half-life of levodopa.5 As the disease progresses, postsynaptic striatal dopamine receptors are subjected to increasingly erratic and pulsatile non-physiological stimulation,5 leading to changes in postsynaptic striatal neurones. If patients continue short-acting dopaminomimetic drugs, this further exacerbates the problem. OFF periods are probably related to low plasma and striatal levels of dopaminergic drugs, whereas peak dose dyskinesia occurs when levels are high. Figure 1 illustrates the progressively narrow therapeutic window as the disease advances.
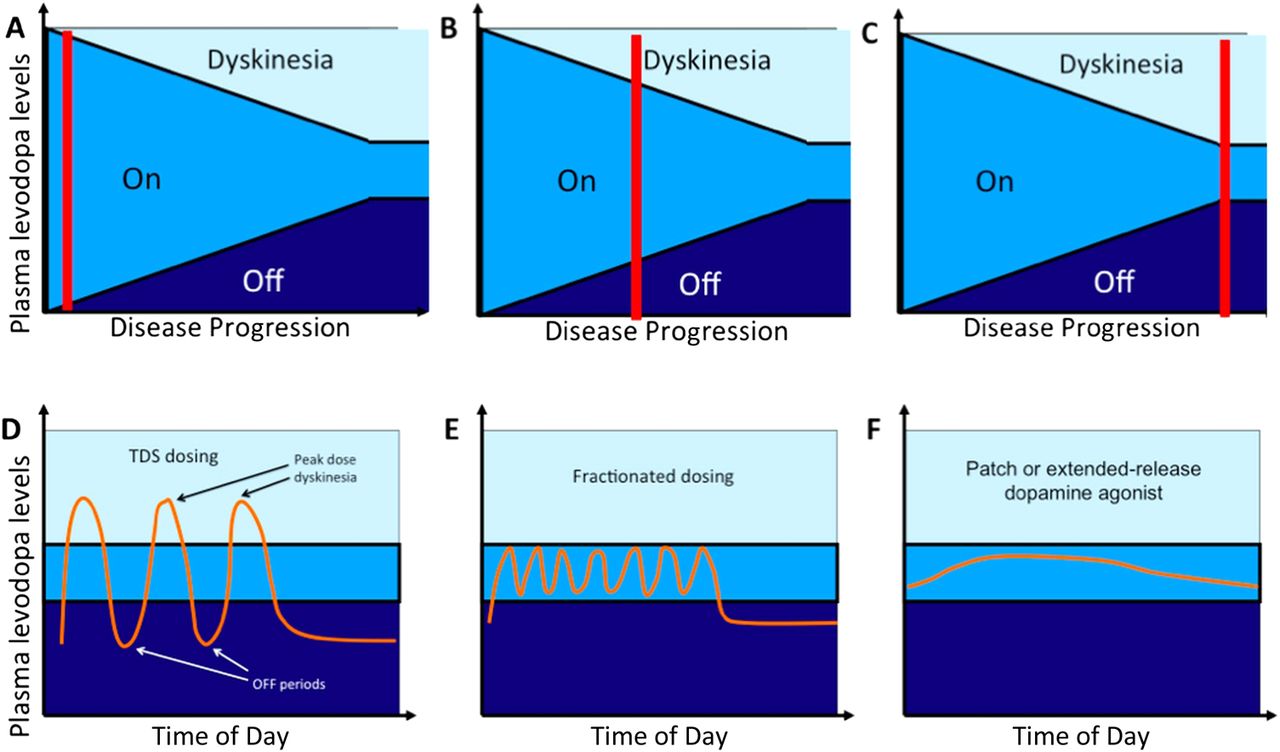
Simplified and schematic representation of motor complications in Parkinson's disease in relation to disease progression. Upper panels (A,B,C) the red bar indicates stage of disease. For a given extracellular or plasma level of dopaminergic therapy, the chances of the patient being in a satisfactory ON state decrease as the condition advances. (A) In early Parkinson's disease treated with levodopa, the optimal therapeutic window (mid-blue shading) is wide with no wearing-OFF (dark blue) or dyskinesia (light blue). (B) As the disease progresses, owing, in large part, to ongoing loss of nigrostriatal neurones and postsynaptic receptor and neuronal changes, the therapeutic window narrows and wearing-off and dyskinesias emerge. (C) In advanced disease, with further narrowing of the therapeutic window, it becomes increasingly difficult to maintain the patient in the satisfactory ON state, with OFF periods and dyskinesias often predominating. Lower panels (D,E,F). Early management strategies to treat motor complications. Note x-axis is now time of day. (D) The patient treated with standard three times daily levodopa experiences sequential OFF periods, ON without dyskinesia, and peak dose dyskinesia. (E) Fractionating levodopa into larger numbers of smaller doses may result in some improvements but is increasingly inconvenient for patients. (F) Use of a longer-acting dopamine agonist may allow more consistent control of motor symptoms, reducing OFF time and time with dyskinesia Courtesy R Genever.
There are several ways to manage early motor fluctuations and dyskinesias (figures 1 and 2), each approved by the UK Parkinson's Disease National Clinical Guideline.6 These include: levodopa fractionation (smaller doses more often), adding a dopamine agonist, adding a catechol-O-methyl transferase inhibitor (eg, entacapone), or adding a monoamine oxidase-B inhibitor (eg, rasagiline). A detailed discussion of these therapies is beyond the scope of this article, but there is no clear evidence to support one approach over another. Amantadine may help if dyskinesia does not respond to these simple measures, but insomnia and confusion may preclude its continued use. Often, patients with Parkinson's disease for several years end up on the same combination of all the above.
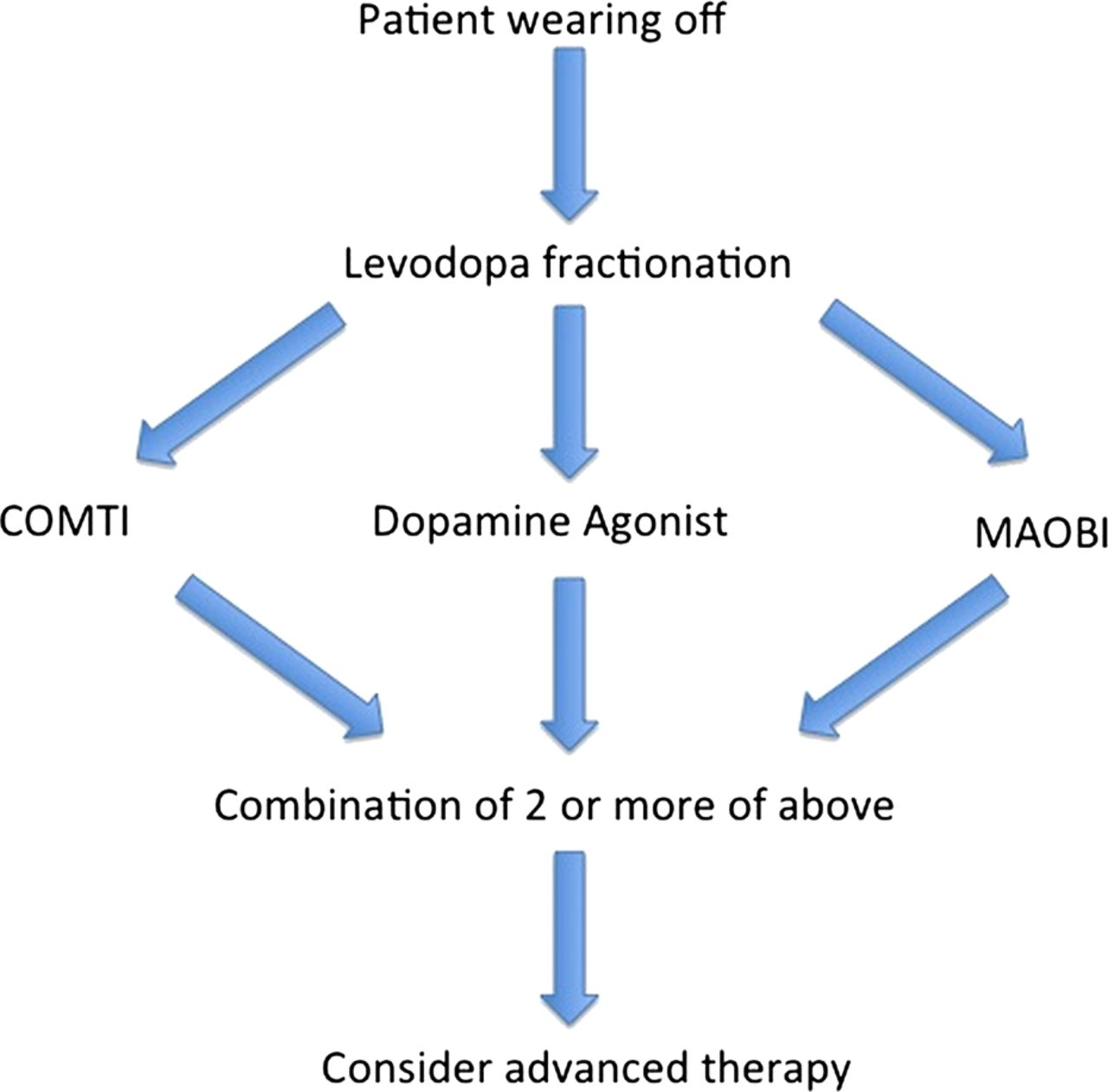
Managing early motor fluctuations in Parkinson's disease. An algorithm for managing the patient on levodopa who has started to experience motor fluctuations. COMTI, catechol-O-methyl transferase inhibitor, for instance, entacapone; MAOBI, monoamine oxidase B inhibitor, for instance, selegiline.
How to recognise the patient who may benefit from ADVANCED therapies
At varying times after starting a treatment to manage early motor complications, the problems worsen to the point where more advanced therapies need to be considered. Two illustrative case histories (box 3) may help the reader to understand the place of advanced therapies in the wider context of the progression of Parkinson's disease.
Illustrative case histories
Case 1. A 62-year-old woman, a nurse with a 5-year history of Parkinson's disease, presented with increasing symptoms of wearing-OFF and immobility towards the end of the dose. At diagnosis, she was treated with selegiline (which she did not tolerate), but then started co-careldopa 125 mg three times a day with good effect. She developed end-of-dose deterioration after 3 years of co-careldopa therapy. Controlled release co-careldopa made her dyskinetic. She was switched to levodopa 100/carbidopa 25/entacapone 200 one tablet four times a day. Continuing wearing-off symptoms were characterised by painful dystonia in her left arm, and prompted the trial of a dopamine agonist (rotigotine transdermal patch) with initial benefit, but after 2 years this was switched to ropinirole. After a further year, because of worsening pain during OFF periods she was started on apomorphine intermittent injection, which worked well for a year, but she was then switched to apomorphine continuous subcutaneous infusion.
At the age of 69 years, knowing that age may soon preclude deep brain stimulation, she was keen to be evaluated for surgery. She had no cognitive problems, had normal speech, no falls or postural instability, and was deemed fit for surgery. After 2 years on apomorphine, she underwent bilateral deep brain stimulation of subthalamic nucleus (STN), with good effect. Her OFF periods vanished and her walking became consistently good. She stopped her apomorphine and levodopa completely, remaining only on ropinirole 4 mg every morning and 8 mg every night. She still has the occasional subcutaneous injection of apomorphine 4 mg if her left arm becomes painful.
Case 2. A 70-year-old man had a 12-year history of Parkinson's disease, but no other medical problems. He presented with increasing walking difficulties and occasional falls, occurring mostly, but not exclusively when his tablets wear off. He was originally treated with ropinirole, and levodopa was added after 3 years as his symptoms worsened. He began to notice wearing-off 4 years ago, and despite levodopa fractionation, addition of entacapone and rasagiline, he was spending 5 h a day OFF, and developed moderately severe peak dose dyskinesias. Tolcapone resulted in severe diarrhoea.
He was started on apomorphine continuous subcutaneous infusion with which he developed nodules and severe somnolence. This was therefore stopped. He was referred for an opinion about deep brain simulation. He was cognitively intact, but it was felt that owing to moderate dysarthria, which could get worse with deep brain stimulation of STN, and because some of his falls were occurring in the ON state, that he was not a good candidate for deep brain stimulation. He was started on levodopa/carbidopa intestinal gel therapy. In spite of some early mild complications with low-grade infection around the gastrostomy site, he responded well, with virtually no daily OFF time, minimal dyskinesia and no more falls. He has gained confidence, and can now go out unaccompanied by his wife.
Clinicians should be alert to the signals that conventional therapies are no longer controlling symptoms, and that more advanced therapies are needed. These should be sought early and the patient referred to a specialist movement disorder service for an opinion. The general neurologist does not need a detailed understanding of the pros and cons of each therapy to recognise these signals.
It is hard to know how many patients suitable for advanced therapies have either never been considered for them or been considered too late, once the ‘ship has sailed’. Colleagues in centres offering deep brain stimulation frequently complain that patients are often referred to them only when already demented, hallucinating or having a host of other non-motor symptoms that will not respond to advanced therapies. A recent Swedish survey of over 3000 patients with Parkinson's disease, one-third of whom had advanced disease, showed that three-quarters had heard of advanced therapies but felt they were ‘denied’ treatment.1 Fewer than 30% of respondents with advanced disease had heard about these therapies directly from their doctor. Although some may ultimately not have been suitable, the general lack of familiarity with these therapies, and lack of time for careful assessment and discussion in busy general clinics probably underlies this failure. A detailed discussion with a specialist about the possible benefits of treatment, even if ultimately deemed unsuitable, often helps to realign patient and clinician expectations. Deep brain stimulation is rarely considered for Parkinson's disease after the age of 70 years (see below), and so it is imperative to avoid ‘missing the boat’.
Patients with young-onset Parkinson's disease (<50 years) have a greater risk of levodopa-induced motor complications, and so should be particularly closely monitored. With their young age and likely longer disease duration, they very likely will ultimately require and benefit from an advanced therapy. However, clinicians should take care in talking about brain surgery to young patients too early in their disease.
Recognising red flags and warning signs for considering advanced therapy
Care planning is key, and the Parkinson's nurse specialist is central to this process. Tinkering neurologists can get caught up in frequent adjustments of oral or transdermal drugs—it is easy to feel you are doing something useful, when, in reality, any benefit from tinkering has long passed. When patients first develop motor fluctuations, sometimes many years before they need complex therapies, the clinician should have an outline plan. We should set goals and be clear that if a specific treatment does not improve the patient's activities of daily living or capabilities, they should progress their therapy. Obviously, the goals must be realistic and there must be consensus on what constitutes an ‘adequate’ trial of a therapy. As a rule of thumb, after 2 months of a stable dose of a given drug, further benefit is unlikely with that drug.
Patients whose uncontrolled motor complications permanently or periodically prevent them from performing specific activities of daily living, despite adequate trials of oral or transdermal medications, should be considered for referral. I would discourage putting strict limits on the amount of daily OFF time or on the severity of a patient's dyskinesia; their distress and inconvenience should be assessed case-by-case. The main hurdle to timely referral is recognising their burden of disability. Asking simple questions, such as, ‘Can you do what you want to do, when you want to do it?’ ‘Do you have any times of day when you feel really good?’ or ‘What can't you do when you are bad that you CAN when you are good?’ are helpful triggers that may reveal a plethora of thereto unrecognised problems.
What are the prerequisites for considering advanced therapies?
These prerequisites reflect the need for realistic expectations, aligned between clinician and patient.
-
There must be no doubt about the diagnosis of idiopathic Parkinson's disease. Patients with secondary parkinsonism and atypical parkinsonian disorders are not suitable for advanced therapies
-
Patients with frank dementia, chronic hallucinosis or psychosis, unresponsive to medication adjustment, are unsuitable for advanced therapies
-
Patients must be clearly levodopa-responsive; those without a clear current or historical response to levodopa usually respond no better to advanced therapies
-
Apart from dyskinesia reduction, these three therapies will not make the patient any better than they already are AT THEIR BEST; the aim is to maintain them at their best for more of the time
-
Levodopa-unresponsive axial symptoms usually respond no better to advanced therapies than to conventional medication. These symptoms are common in advanced Parkinson's disease and often overlooked or misunderstood. In practice, they include dysarthria, dysphagia, falls through loss of postural reflexes and/or freezing of gait when in the ON state (for more information see box 4).
Box 4Levodopa-unresponsive axial symptoms
Probably mediated by non-dopaminergic systems, and do not respond well to dopaminergic therapy33 or advanced therapies including:
-
Postural instability
-
Dysarthria
-
ON freezing of gait
What is postural instability?
-
Use the ‘Pull’ test in the ON state with the patient at her best
-
The examiner stands behind the patient, who is in turn in front of a solid wall
-
Pull the patient back by the shoulder a total of three times with increasing force
-
Patient is instructed to put a foot back for stability while being pulled
-
Patients unable to put a foot back sufficiently quickly to prevent a potential fall, or who simply fall backwards into the examiner have significantly impaired postural reflexes
What is ON freezing?
-
Distinguishing ON freezing from freezing in the OFF state (when freezing can be expected as part of general hypokinesia) is difficult
-
Patients describe feet as ‘glued’ or ‘velcroed’ to the floor,
-
Usually happens suddenly and without warning, in doorways or in unfamiliar environments especially outdoors, and may fall
-
Ask ‘Do your feet freeze suddenly and unpredictably when your general movements are otherwise good, and is it usually for seconds only?’ If yes, this is ON freezing
-
Ask also ‘When you freeze, are you generally stiff slow, shaky, and this lasts at least minutes or even hours?’ By contrast with ON freezing, this is probably freezing related to OFF periods and may respond to increased/retimed medication and advanced therapies.
-
-
Many non-motor symptoms, such as apathy, drooling of saliva, constipation, nocturia and sleep disturbances may not respond to any advanced therapy, though there are no good data on their effects on non-motor symptoms.
-
Patients must understand that none of these therapies is a cure, and none slows the progression of the disease, or prevents dementia
How does each therapy work?
All three advanced therapies aim to circumvent the problem of variable absorption of dopaminomimetic drugs and, therefore, reduce or avoid pulsatile stimulation of striatal dopamine receptors. They allow for this in different ways, either by:
-
Restoring more ‘physiological’ conditions in the striatum by continuous drug delivery and, therefore, continuous pharmacological stimulation (apomorphine continuous subcutaneous infusion and continuous intrajejunal infusion of levodopa/carbidopa intestinal gel), or by
-
High-frequency continuous electrical stimulation through functional neurosurgery to help to ‘normalise’ excessive neuronal activity in the output nuclei of the basal ganglia.
Apomorphine
Apomorphine, the oldest dopaminergic medication, has been used for analgesia, insomnia, alcohol dependence and schizophrenia. It was originally used for Parkinson's disease over 60 years ago but abandoned with the advent of levodopa. It is a potent D1 and D2 receptor agonist, rapidly absorbed after subcutaneous injection (C max=20 min), and has a short half-life of 40 min. It works rapidly: when injected, the onset of effect is usually heralded by yawning after about 5 min, followed by rapid improvement of all parkinsonian features.
Traditionally, patients have been brought into hospital to start apomorphine, often for several days. With increasing cost pressures, it is now often done as a day case ‘challenge’, sometimes in primary care or a community hospital, and usually carried out and overseen by the Parkinson's disease nurse specialist (see box 5 for details).
Initiation of treatment with apomorphine
-
The main aim of the apomorpine challenge is to determine the dose at which a good motor response is achieved.
-
Patients are pretreated with a 3-day course of oral domperidone, 10–20 mg three times a day, before the challenge. Domperidone may need to be continued after successfully starting therapy. Domperidone can prolong the QT interval. If patients need chronic treatment, the dose should be limited to 30 mg/day in elderly patients, or those with cardiac disease, or who are taking other QT-prolonging drugs, and the ECG should be monitored
-
Prominent orthostatic hypotension may occur, so blood pressure should be closely monitored
-
A dosage of 1 mg is administered by subcutaneous injection, with increments of 1 mg every 15 min until the patient responds. This is the dose on which the patient is discharged, for instance, a patient who responds at 4 mg will be started and discharged on 4 mg/h.
-
Apomorphine is delivered using a compact syringe driver connected via a flexible infusion line to a subcutaneous needle. The needle is usually inserted into the skin of the anterior abdominal wall or the anterior thigh
-
Apomorphine is most conveniently supplied in prefilled syringes which are much easier to set up than the traditional ampoules
-
Once on a stable dose, oral medication can then start to be withdrawn, starting with the dopamine agonist if the patient is receiving one
-
Some patients may safely be started on therapy at home by starting them on a low dose of 1 mg/h and titrating slowly until there is a good response
Apomorphine comes either as an intermittent subcutaneous injection (Pen-ject), or as prefilled syringes for continuous subcutaneous infusion. The Pen-ject resembles an Epi-Pen and can be carried discreetly in a handbag or pocket. It is very useful for patients with infrequent disabling OFF periods, for instance, those requiring perhaps no more than 2–3 injections per day. This may have a liberating effect, for instance, in patients unwilling to leave the house. However, in my and others’ experience, intermittent injection can lead to overuse and abuse, especially in those patients who tend to overuse oral dispersible preparations of levodopa. These patients often pre-empt OFF periods and sometimes this leads to rapid escalation in usage and development of the ‘dopamine dysregulation syndrome’.7
My personal preference for willing, motivated and socially supported patients who are experiencing disabling motor complications is to treat with apomorphine continuous subcutaneous infusion rather than the Pen-ject. However, the assistance needed to set up the pump and insert a new needle every day may exclude patients who live alone, or whose carers are needle phobic or unwilling to assist with needle insertion. Typically, apomorphine is infused throughout the waking day, and the pump taken down at night. For those with disabling nocturnal motor symptoms, 24-h infusion is possible, though unlicensed.
Deep brain stimulation
Electrical stimulation of various anatomical targets in the basal ganglia, usually the subthalamic nucleus (STN), globus pallidus internus segment (GPi) and ventral intermediate nucleus (Vim) of the thalamus, owes its development to the observation in the first half of the last century, that vascular lesions in some patients with Parkinson's disease substantially ameliorated motor symptoms.8 This led to great enthusiasm for neurosurgical intervention with various lesioning or ablative techniques, though with variable results, some catastrophic. These techniques were largely abandoned with the advent of levodopa. However, they re-emerged as possible treatment for the motor complications of levodopa therapy, when again it was observed that dyskinesias could be improved by lesioning the GPi, and intractable tremor could be improved with lesions of the Vim. Thus, irreversible lesioning techniques enjoyed a renaissance in the late 1970s and 1980s.
Pioneering studies involving electrical stimulation of these same targets in MPTP (1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine)-treated primates showed similar benefit without the need for destructive lesions.9 Since the early 1990s, the functional neurosurgical procedure of choice has usually been bilateral high-frequency stimulation of the STN. This involves two permanently implanted multicontact electrodes connected via two subcutaneous wires to a single dual-channel pulse generator or ‘pacemaker’, itself surgically implanted subcutaneously below the clavicle. The GPi is also used and may be associated with fewer cognitive and axial adverse effects, and is useful for patients with prominent dyskinesia (box 6 gives details of surgical and implantation procedures). Vim stimulation is reserved for patients with intractable tremor at any stage of the disease, and will not be discussed further.
Initiation of deep brain stimulation therapy
-
Deep brain stimulation is carried out in only a few centres that are remote from the patient's home
-
Patients need to make several pre- as well as postoperative visits
-
Detailed preoperative assessments include cognitive testing, structural brain imaging and usually a levodopa challenge to ensure that the patient is levodopa-responsive
-
A stereotactic frame is anchored to the skull, and CT and MRI is performed to localise precisely and calculate the coordinates of the target structures
-
Electrode implantation is carried out by drilling of two burr holes and careful insertion of the two electrodes to their targets
-
In many centres, the procedure is carried out under local anaesthesia
-
Intraoperative MRI techniques can also be used to ensure accurate electrode placement
-
Usually, patients’ symptoms improve intra- or immediately postoperatively, because of temporary lesioning from electrode placement
-
The wires are tunnelled under the skin but are usually not connected to the pulse generator until some days after implantation of the electrodes
-
Repeated adjustment of stimulation parameters may be required for several months after surgery, presumably reflecting plastic changes in basal ganglia circuitry.
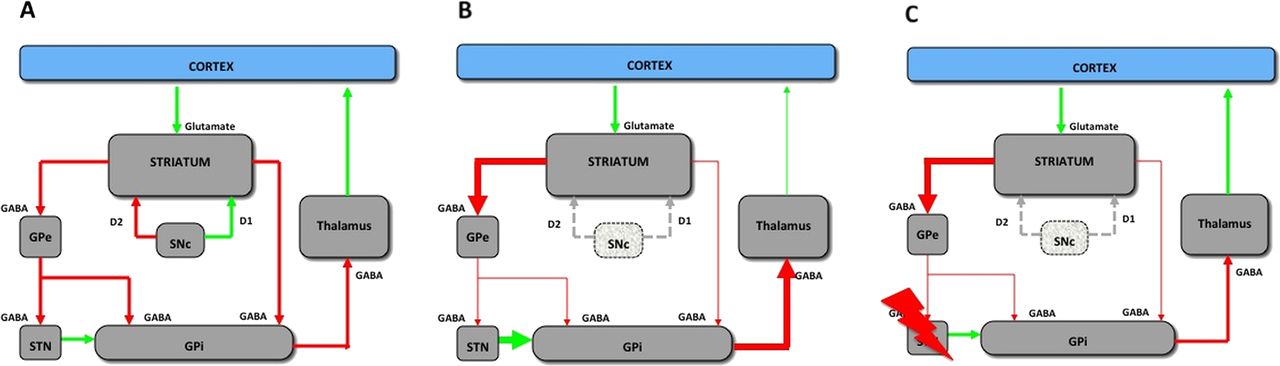
We do not fully understand how deep brain stimulation improves parkinsonian symptoms. Figure 3 shows the proposed mechanism. In untreated Parkinson's disease, the loss of dopaminergic input to the striatum from the substantia nigra results in excessive movement-inhibiting neuronal activity in the GPi, the main output nucleus of the basal ganglia. This inhibits activity in the thalamus and indirectly in the motor cortex. High-frequency electrical stimulation of either STN or GPi suppresses the overactivity, in turn ‘normalising’ thalamic and motor cortical activity and restoring movement.
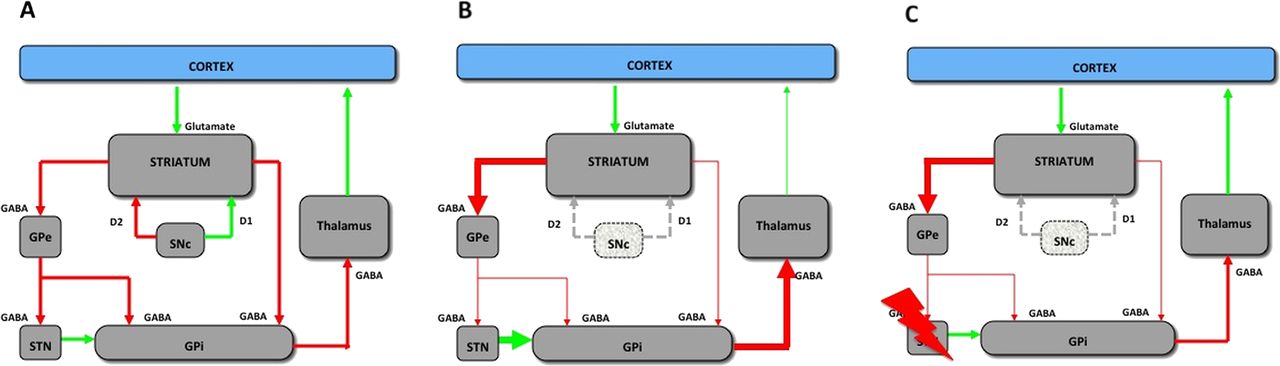
Schematic showing the proposed mechanism whereby DBS of the STN/globus pallidus internal segment (GPi) restores ‘normal’ basal ganglia output. DBS, deep brain stimulation; GABA, gamma-amino butyric acid; GPe, globus pallidus external segment; GPi, globus pallidus internal segment; SNc, substantia nigra pars compacta; STN, subthalamic nucleus. In all panels, red arrows are inhibitory, and green arrows excitatory. (A) The normal basal ganglia. The direct pathway is the direct link between striatum and GPi. Activity in this pathway increases cortical activity (‘the go pathway’). The indirect pathway is the link between striatum and GPi via GPe and STN. Activity in this pathway decreases cortical activity (‘the stop pathway’). Dopaminergic input to the striatum facilitates the direct pathway via D1 receptors, and simultaneously inhibits the indirect pathway via D2 receptors. (B) In the untreated parkinsonian state, loss of dopaminergic input to the striatum through degeneration of the SNc results in reduced activity in the direct pathway and increased activity in the indirect pathway, leading to an overactive STN and GPi, and an inhibited thalamus. (C) High-frequency stimulation of the STN (lightning arrow) or GPi in DBS is thought to reduce the excessive neuronal activity in the surgical target, which in either case may restore the inhibitory output of the GPi towards ‘normal’ and so facilitates movement. There is no simple explanation of the mechanism of dyskinesia reduction. Courtesy P Connick.
Levodopa/carbidopa intestinal gel
Infusing levodopa directly into the small intestine is not a new idea. Levodopa is absorbed exclusively in the jejunum, and so it is logical to deliver it directly to this part of the gut. Various attempts to do this have been more as proof of principle than serious long-term option.10 There is good evidence that delayed gastric emptying and consequent delayed absorption of levodopa make major contributions to response fluctuations. However, levodopa is relatively insoluble, and requires large volumes of fluid to be administered, limiting practical development of this idea. The development of a gel as a stable carrier for levodopa, combined with carbidopa in the same 4:1 ratio as in the oral preparations of co-careldopa, is proving a practical solution.11
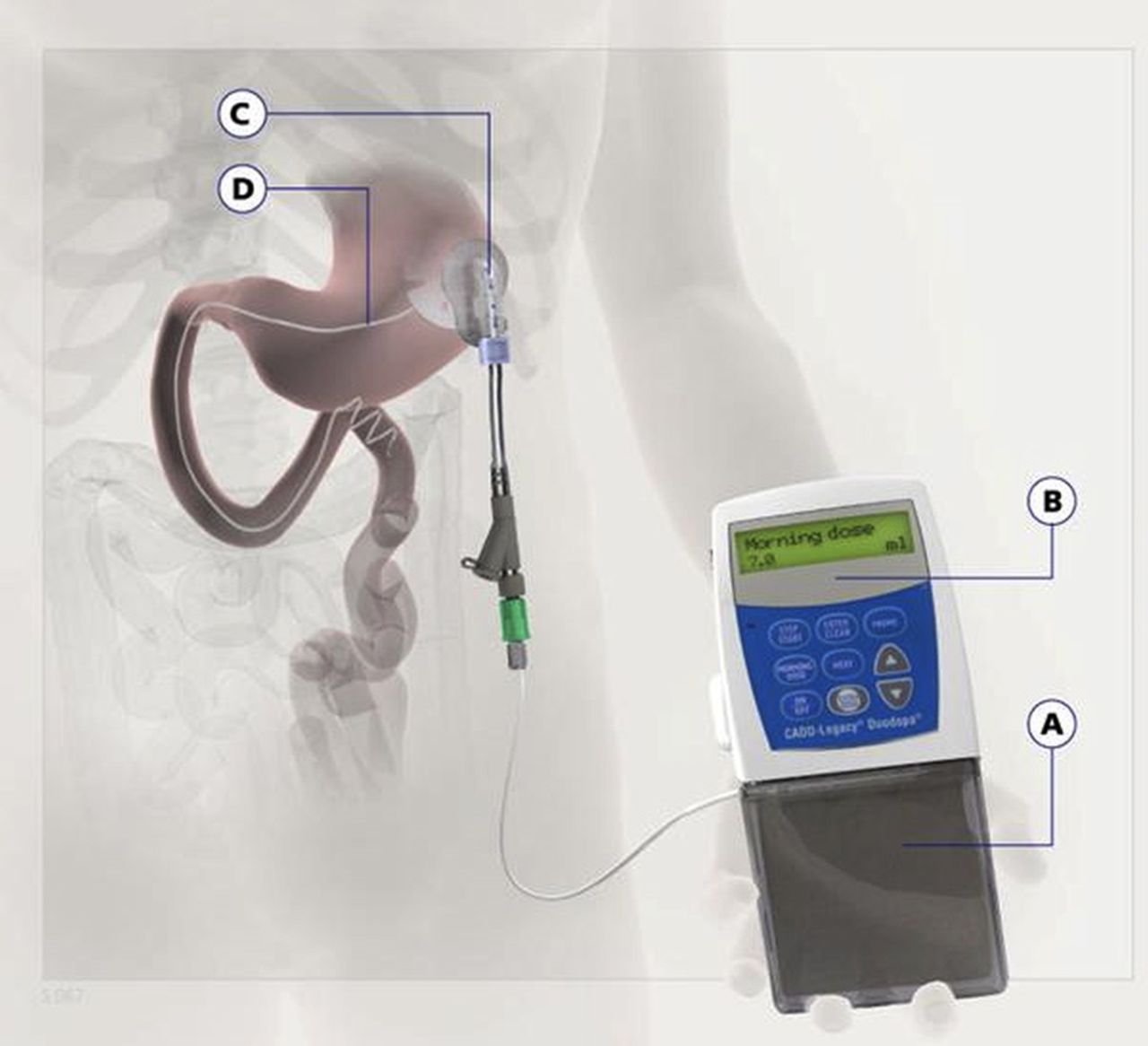
Levodopa/carbidopa intestinal gel is delivered by a purpose-built pump, and the cartridge containing the gel is changed daily (figure 4). Each cartridge contains 2 g of levodopa and 500 mg carbidopa, sufficient for most patients’ daily requirements. A modified percutaneous gastrostomy tube is inserted endoscopically. An inner jejunostomy tube is then inserted through the percutaneous gastrostomy into the jejunum (figure 5). The pump is attached to the inner tube and the gel is infused directly into the jejunum (box 7).
Starting levodopa/carbidopa intestinal gel therapy
-
Patients require a 1-week admission to hospital
-
A temporary nasojejunal tube is passed into the stomach by standard techniques, usually on a Friday
-
The patient can go home for the weekend, returning on Monday for a plain abdominal x-ray to check the tube's position. Most tubes will spontaneously pass through the pyloric sphincter: those that do not have to be placed endoscopically
-
Patient is started on levodopa/carbidopa intestinal gel pump connected to nasojejunal tube
-
Over several days, the dose of levodopa/carbidopa intestinal gel is optimised, and the patient's normal Parkinson's drugs are gradually reduced with a view to stopping all other therapies
-
The nasojejunal tube is removed, the percutaneous gastrostomy and inner tube are inserted endoscopically, and the patient begins to receive levodopa/carbidopa intestinal gel through the inner tube
-
The manufacturer of levodopa/carbidopa intestinal gel currently provides a specially trained nurse to supervise the titration of the drug
-
Significant levels of support and frequent dose adjustments are usually required after discharge, with good stoma care being a priority. The Parkinson's disease nurse specialist is in a good position to coordinate the various agencies involved
-
Levodopa/carbidopa intestinal gel is usually infused during waking hours only, with oral doses of controlled release levodopa often sufficient to control noctural motor symptoms
-
Some patients, like some of those receiving apomorphine, benefit from 24-h therapy, though this is also unlicensed.

A patient treated with levodopa/carbidopa intestinal gel therapy. Note the sizeable and heavy pump and cartridge attached to the inner tube which is fed through the percutaneous gastrostomy tube into the jejunum endoscopically.

A schematic representation of the levodopa/carbidopa intestinal gel therapy system. (A) The cartridge containing levodopa/carbidopa gel in a 4 : 1 ratio. (B) The purpose-built pump. (C) Percutaneous access port. (D) The inner tube is passed endoscopically into the jejunum. This tube has a pigtail end which is said to reduce the chances of dislocation. Source: Abbott 2012.
What benefits can patients expect from each therapy?
As mentioned previously, patients must understand that, apart from severe dyskinesia, none of these therapies is likely to improve them beyond their current best, or to eliminate all their motor complications. The main aim is to increase the time spent at their best. All three therapies aim to reduce OFF time, increase ON time and/or reduce ON time with troublesome dyskinesia. Clearly, the key measure of benefit is improved ability consistently to carry out activities of daily living and improved quality of life: these have been incompletely studied across all three therapies.
There are no good studies directly comparing the three therapies, since very few patients are suitable for all three; such a study would not be relevant to the real world. In our recent systematic review of the three therapies,12 it proved difficult to compare trials as they often use different inclusion criteria, methods and end points. We concluded that no one modality was superior to another.
Apomorphine continuous subcutaneous infusion
There are no randomised controlled studies of apomorphine continuous subcutaneous infusion. A review of the various open-label studies showed improvements in mean daily OFF time of 38–80%.13 One small study of 12 patients showed a mean reduction of 2.4 h daily OFF time.14 In these studies, it is often possible to stop oral or transdermal dopamine agonists when starting apomorphine; levodopa dose may be reduced by up to 81%.13 In fact, dyskinesias are unlikely to reduce unless the dose of levodopa can be lowered. However, all these studies were uncontrolled and short term. In practice, it is almost impossible to get patients off ALL their oral drugs; attempts to do so often fail, even in experienced hands (N Fletcher, personal communication). The effects of apomorphine continuous infusion on quality of life and cost effectiveness have not been studied systematically. The basic cost of apomorphine infusion depends on dose, but may be as much as £11 000 per annum.
Deep brain stimulation
Among the three treatments, the best evidence is for STN deep brain stimulation. However, even here there are few good randomised studies comparing stimulation of STN versus GPi; the larger trials confirm that, for selected patients, quality of life improves by 12–23%, and daily ‘ON’ time increases by around 4.5 h.15–17 Patients achieve a mean levodopa dose reduction of around 400 mg/day. Patients with prominent dyskinesia may benefit more from stimulation of GPi than of STN,18 although this is controversial—patients randomised to either had similar improvements in time spent with troublesome dyskinesia at 24 months.19 Longer uncontrolled follow-up studies have shown sustained, albeit reduced, benefit when patients are off their medication.20 The basic cost of the deep brain stimulator and operation is around £30 000, but costs in subsequent years are an order of magnitude lower. In a questionnaire-based study comparing patients treated with subthalamic deep brain stimulation versus best medical treatment, cost per quality-adjusted life year of subthalamic deep brain stimulation was €34 389.21
Levodopa-carbidopa intestinal gel
The main aim of levodopa/carbidopa intestinal gel therapy is again to reduce daily OFF time and increase ON time without dyskinesia. A recent randomised international multicentre, double-blind, double-dummy 12-week study compared levodopa/carbidopa intestinal gel with oral immediate-release levodopa in 71 subjects. Daily OFF time fell by 4 h in the levodopa/carbidopa intestinal gel group and by 2 h in the oral levodopa group (p=0.0015), with similar improvements in ON time in the levodopa/carbidopa intestinal gel group (p=0.0059).22 An open label follow-up of the patients in this study is ongoing and the benefit seems to be sustained at 1 year. Quality of life (summary PDQ-39 index) improved in levodopa/carbidopa intestinal gel patients. The basic cost of levodopa/carbidopa intestinal gel is around £30 000 per year for the duration of therapy, based on Markov simulations, with estimates of incremental cost per quality-adjusted life year ranging from £36 02423 to £94 000.24 However, there are no long-term or rigorous cost-effectiveness data for this treatment modality.
Summary of efficacy and cost effectiveness
In summary, the efficacy of these therapies in terms of daily OFF and ON times may not be greatly different. Dyskinesia reduction is most convincing for deep brain stimulation, with GPi possibly superior to STN. Medium-term quality-of-life improvements, and short-term cost effectiveness are convincing only for deep brain stimulation. The main cost of deep brain stimulation is in the first year, whereas both apomorphine and levodopa/carbidopa intestinal gel incur recurrent annual costs. A recent questionnaire-based study of the costs of all three therapies in the Spanish healthcare system showed that the mean cumulative 5-year cost per patient was lower with deep brain stimulation (€88 014) versus either apomorphine infusion (€141 393) or levodopa/carbidopa intestinal gel (€233 986) (p < 0.0001). Deep brain stimulation had the lowest cumulative costs from year 2, with a yearly average cost of €17 603 versus €46 797 for levodopa/carbidopa intestinal gel and €28 279 for apomorphine.25
What are the main adverse events with each therapy?
Apomorphine continuous subcutaneous infusion
The disadvantages of apomorphine relate to its propensity (as a dopamine agonist) to produce hallucinations, psychosis, sedation and somnolence, orthostatic hypotension and a positive Coombs’ test. However, clinically significant haemolytic anaemia is rare. The commonest adverse effect leading to stopping treatment is subcutaneous nodule formation, which occurs in most patients.26 Scrupulous hygiene, proper needle insertion technique and site rotation may help. Unproven techniques, such as massage, ultrasound and silicone gel dressings may reduce nodule formation in individual patients.27
Deep brain stimulation
Adverse reactions to deep brain stimulation relate either to the surgical procedure and hardware or to the stimulation itself. In a meta-analysis of 22 studies, the most common serious adverse event was surgery-related intracranial haemorrhage, occurring in up to 4%;28 its severity and long-term consequences vary greatly among studies. In the PD-SURG study, only four out of 183 (2.2%) patients had postoperative intracranial haemorrhage, including one death; one haemorrhage occurred 5 months after treatment, probably unrelated to the surgery.17 The cumulative incidence of surgery-related adverse effects in the large meta-analysis was 11%,28 but varied between studies; 4.4% had to have parts of the device replaced due to infection, migration of the leads or malfunction. The most common stimulation-related adverse events were dysarthria (9.3%), weight gain (8.4%), depression (6.8%), eyelid opening apraxia (3.6%), dyskinesias (2.6%) and mania (1.9%).
Levodopa-carbidopa intestinal gel
Although levodopa/carbidopa intestinal gel therapy is perceived as less invasive than deep brain stimulation, there are still potentially serious adverse effects.26 Device and tube-related problems are common with levodopa/carbidopa intestinal gel therapy, including dislocation, occlusion, kinking, knotting or erosion of the tube. Other patients have problems with the stoma, including infection, excessive granulation tissue or with the pump itself. The most common reason for stopping therapy is repeated tube dislocation. Peripheral neuropathy is common in Parkinson's disease, and may occur with levodopa/carbidopa intestinal gel therapy;29 hyperhomocysteinaemia associated with levodopa therapy may be responsible. As patients are often on higher doses of levodopa after starting levodopa/carbidopa intestinal gel, having stopped other dopaminergic drugs, the risk may be higher with intestinal gel than with oral levodopa therapy. However, there are no good quality case-control data to allow accurate risk assessment. Practically, patients should be screened for neurophysiological evidence of peripheral neuropathy and by measuring serum homocysteine and vitamin B12 before levodopa/carbidopa intestinal gel therapy.
What factors determine selection of one device-aided treatment over another?
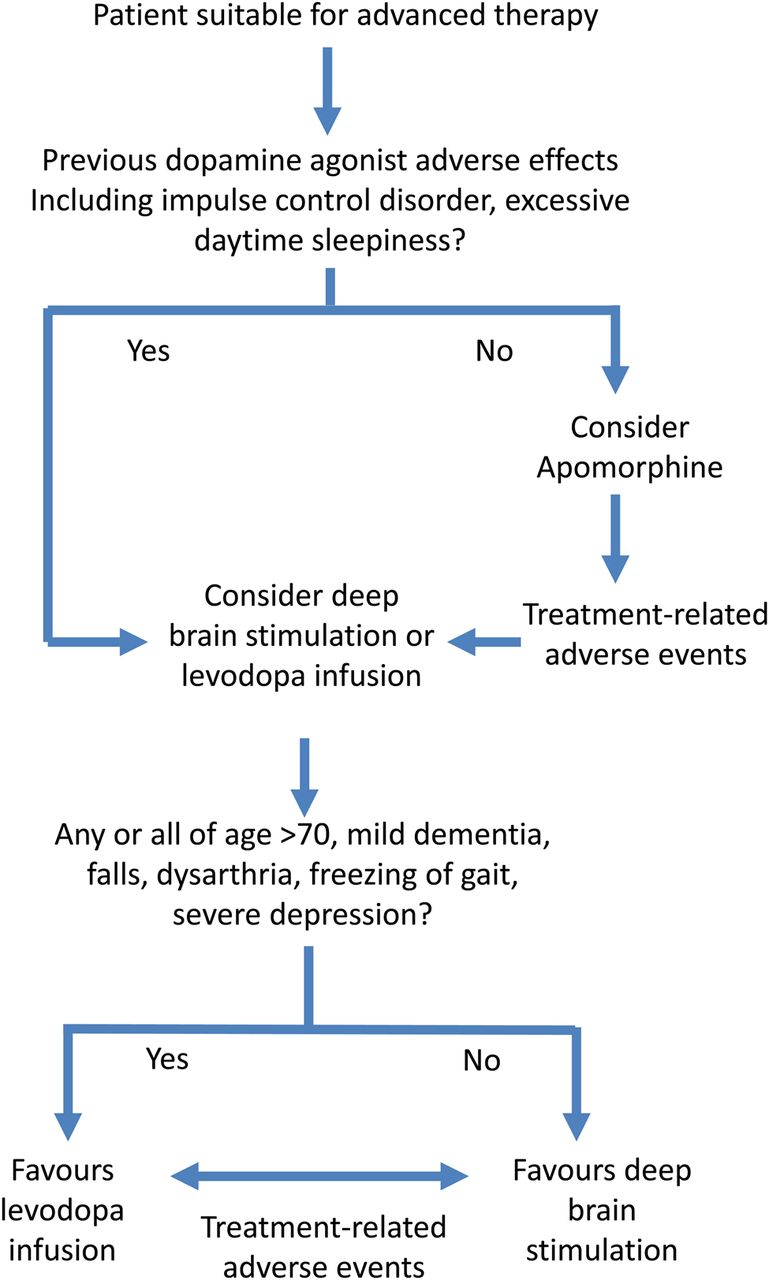
Without convincing data to show that one advanced treatment is better than another, the decision to use a specific therapy must be on a case-by-case basis. Thus, it depends more on patient and clinician preference and on matching the potential adverse event profile of each treatment to the patient's clinical profile. There are several factors that may guide the clinician to the most appropriate therapy (table 1). Figure 6 shows how these factors might affect the decision.
Illustrating how specific complications of the disease process and documented adverse effects of previous drug therapy may influence the decision to use device-aided therapy

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
A decision-making algorithm for advanced therapies in Parkinson's disease. Rigid adherence to this algorithm is not intended, but this is rather a simplified overview of the main factors influencing decision-making. Levodopa/carbidopa intestinal gel and deep brain stimulation should both be considered equally in all patients not suitable for or who have experienced adverse effects from apomorphine. Factors favouring levodopa/carbidopa intestinal gel are as shown. The cut-off age of 70 years for deep brain stimulation is not fixed but used as a rough rule of thumb.
The access to these therapies varies worldwide. In the UK and in most European countries, deep brain stimulation is offered only in tertiary neuroscience facilities. Apomorphine is available to specialists in most local hospitals in the UK and many in Europe, but to date neither apomorphine nor levodopa/carbidopa intestinal gel are available in the USA. In the UK, because of cost and lack of accepted cost-effectiveness data, levodopa/carbidopa intestinal gel therapy is generally reserved for those who have either failed or are deemed unsuitable for apomorphine and deep brain stimulation, regardless of patient preference. In England, individual funding requests from the primary care health boards, known as ‘Primary Care Trusts’, have to be made, and are often refused. By contrast, in some European countries such as Germany, clinicians may start whichever therapy that they and the patient agree is most suitable.
Patients starting either apomorphine or levodopa/carbidopa intestinal gel usually require a supportive and motivated carer to assist setting up and adjusting the pump/line. By contrast, although deep brain stimulation allows more patient independence and autonomy, without lines or needles, the stimulator usually requires indefinite follow-up at the implantation centre. Patients travelling long distances must be made aware of this, since some cannot cope with travel from places without the facilities to check batteries. The batteries need surgical replacement every few years, although there are now some rechargeable units.
As discussed earlier, the main indication for moving to an advanced therapy is uncontrolled motor fluctuations and/or dyskinesias. All three therapies should be considered where motor fluctuations are the main problem. Some patients, by contrast, are virtually never free of dyskinesia when in the ‘ON’ state and have relatively little wearing-off. In this situation, there is perhaps the best evidence for deep brain stimulation possibly of the GPi as above, although the extent to which apomorphine infusion can reduce dyskinesia is controversial, as there are no good controlled data.
Although apomorphine continuous subcutaneous infusion is the least invasive, cheapest (in the short term) and most readily available therapy in the UK, there are potential adverse effects, and no proof of cost effectiveness. It is reasonable for a general neurologist to start apomorphine infusion treatment, with ongoing supervision by a Parkinson's disease nurse specialist, but this should not preclude or delay consideration of one of the other two therapies. There are no data on how long patients can effectively remain on apomorphine, but expert experience is that this is not necessarily a long-term option, as adverse effects—especially nodules—limit its longer-term use. Clearly, if a patient is not suitable for apomorphine, or has failed a trial of it, deep brain stimulation and levodopa/carbidopa intestinal gel therapy should be considered. I would advocate referral to a specialist centre, ideally one with expertise in all three therapies BEFORE starting apomorphine, so that all options can be considered at the outset.
Age and comorbidity are important factors in choosing therapy, especially deep brain stimulation. Fitness for general anaesthesia, though not always required, is an obvious consideration. Patients with marked cerebral atrophy on imaging are more likely to develop intracranial haemorrhage after this surgery. Deep brain stimulation appears effective irrespective of age17 although benefits on quality of life may wane more rapidly in elderly patients.30 Age has not been systematically studied in respect of apomorphine or levodopa/carbidopa intestinal gel therapy, but both these should be used with caution in biologically aged patients with multiple comorbidities. In practice, a flexible upper limit of 70 years of age is used to select patients for STN deep brain stimulation, with perhaps slightly higher limits for deep brain stimulation of GPi. Patients would not normally be considered for deep brain stimulation if they have one or more of: cognitive impairment affecting multiple domains (especially language function), marked dysarthria, falls and postural instability, or a history of severe depression or attempted suicide. Patients with a history of adverse reactions to oral or transdermal dopamine agonists, in particular excessive daytime sleepiness, are more likely to experience these adverse effects with apomorphine.
Impulse control disorders may develop with dopaminergic therapy, particularly with dopamine agonists, and include hypersexuality, pathological gambling and compulsive shopping and eating. There are no data comparing the risk with respect to oral or transdermal dopa agonists in patients on apomorphine, but 4–8% of apomorphine-treated patients may develop hypersexuality.13 ,31 The risk of impulse control disorders with levodopa/carbidopa intestinal gel is uncertain. Deep brain stimulation of STN or of GPi may improve impulse control disorders, possibly through reducing the total dopaminergic therapy. However, some studies show no benefit, or even worsening, after surgery.32 In summary, in patients with a history of previous impulse control disorders, deep brain stimulation and levodopa/carbidopa intestinal gel therapy are probably preferable to apomorphine.
Summary
I have tried to present an evidence-based but essentially personal view of how to select therapies for advanced Parkinson's disease. The key message is not to deny or to delay consideration of advanced therapies that may help your patient. Procrastination and continued tinkering are unlikely to help and are simply a waste of time. Long follow-up intervals between appointments often add to this unnecessary delay. There is insufficient evidence to support selecting one device-aided modality over another based solely on efficacy, tolerability or safety. However, each treatment has a distinct adverse event profile that influences treatment choice.
Patients suitable for deep brain stimulation will have no medical conditions preventing surgery, no significant cognitive or psychiatric dysfunction, and probably be aged <70 years. Variables that negatively affect the appropriateness of referral for deep brain stimulation are: moderate intellectual impairment, levodopa-unresponsive axial symptoms, such as postural instability and freezing of gait in the ON state, dysphagia, dysarthria and older age. The restrictions on patients with predominant dyskinesias may be less stringent in respect of deep brain stimulation of GPi.
Most patients with advanced Parkinson's disease who fulfil the criteria for deep brain stimulation are also candidates for levodopa/carbidopa intestinal gel or apomorphine infusion. However, as the criteria for deep brain stimulation are by far the most restrictive, many more patients, including patients considered too old for surgery, are eligible for one of the pump treatments. In addition, patients with mild dementia and history of impulse control disorder may be candidates for levodopa/carbidopa intestinal gel therapy.
Unfortunately, there are no data on long-term outcomes for all three therapies. Patients with Parkinson's disease will, of course progress, and many will ultimately dement. Knowing when to stop infusion therapies in the palliative stage is just as important as knowing when to start them. For chronic treatment over years, deep brain stimulation is probably the least costly device-aided treatment. However, all therapies potentially place significant burdens on overstretched healthcare resources, and there may be more remote socioeconomic effects of treatment. Therefore, individual patient characteristics (including age, disease duration, comorbidities and relative contraindications), local availability, caregiver support and especially a patient's personal preference for a device, are likely to remain the main factors influencing treatment choice.
Summary Points
-
Clinicians treating Parkinson‘s disease should be alert to the potential for, and impending failure of conventional oral medication adequately to control motor complications
-
Patients suitable for advanced therapies should be referred early to a specialist with experience of all three advanced therapies, deep brain stimulation, apomorphine infusion and levodopa/carbidopa intestinal gel therapy
-
Patients with frank dementia, chronic hallucinosis / psychosis are not suitable for advanced therapies
-
All three therapies aim to ‘normalise’ basal ganglia output by providing more constant pharmacological or electrical stimulation
-
Appropriate candidates for all therapies should have a diagnosis of idiopathic Parkinson‘s disease, troublesome motor fluctuations and or dyskinesias despite optimal medical therapy or intolerance to anti-parkinsonian medication and definite motor levodopa-responsiveness
-
Levodopa-unresponsive symptoms including many non-motor symptoms will usually not respond to any of these therapies
-
There is no evidence to select any one therapy over another in a patient suitable for all three therapies
References
Footnotes
-
Competing interests PFW has received honoraria and consulting fees from Abbott, Genus Pharmaceuticals and has attended a DBS course sponsored by Medtronic.
-
Provenance and peer review Commissioned; externally peer reviewed. This paper was reviewed by Nick Fletcher, Liverpool, UK.
Other content recommended for you
- Parkinson’s disease: etiopathogenesis and treatment
- Subthalamic nucleus stimulation and compulsive use of dopaminergic medication in Parkinson's disease
- Deep brain stimulation for movement disorders
- Deep brain stimulation of the subthalamic nucleus: effectiveness in advanced Parkinson’s disease patients previously reliant on apomorphine
- Long-term outcome of subthalamic nucleus deep brain stimulation for Parkinson's disease using an MRI-guided and MRI-verified approach
- Efficacy of deep brain stimulation of the subthalamic nucleus in Parkinson’s disease 4 years after surgery: double blind and open label evaluation
- Emergencies and critical issues in Parkinson’s disease
- Effects of subthalamic deep brain stimulation on dysarthrophonia in Parkinson’s disease
- A prospective, controlled study of non-motor effects of subthalamic stimulation in Parkinson’s disease: results at the 36-month follow-up
- Different patterns of medication change after subthalamic or pallidal stimulation for Parkinson’s disease: target related effect or selection bias?