Article Text

Abstract
Traumatic brain injury (TBI) remains a major public health problem. This review aims to present the principles upon which modern TBI management should be based. The early management phase aims to achieve haemodynamic stability, limit secondary insults (eg hypotension, hypoxia), obtain accurate neurological assessment and appropriately select patients for further investigation. Since 2003, the mainstay of risk stratification in the UK emergency departments has been a system of triage based on clinical assessment, which then dictates the need for a CT scan of the head. For patients with acute subdural or extradural haematomas, time from clinical deterioration to operation should be kept to a minimum, as it can affect their outcome. In addition, it is increasingly recognised that patients with severe and moderate TBI should be managed in neuroscience centres, regardless of the need for neurosurgical intervention. The monitoring and treatment of raised intracranial pressure is paramount for maintaining cerebral blood supply and oxygen delivery in patients with severe TBI. Decompressive craniectomy and therapeutic hypothermia are the subject of ongoing international multi-centre randomised trials. TBI is associated with a number of complications, some of which require specialist referral. Patients with post-concussion syndrome can be helped by supportive management in the context of a multi-disciplinary neurotrauma clinic and by patient support groups. Specialist neurorehabilitation after TBI is important for improving outcome.
- Neurosurgery
- Traumatic Brain Injury
Statistics from Altmetric.com
Sources and selection criteria
-
This review aims to outline the current management of adult patients with traumatic brain injury (TBI). The sources of information we used were primarily evidence-based guidelines (international and UK), Cochrane and systematic reviews, expert panel recommendations, as well as a number of highly cited seminal papers published in the field of TBI. The method we employed to classify the class of evidence and the level of recommendations is the same used by the Brain Trauma Foundation in its 2007 guidelines (table 1). We decided to use the same method in order to maintain consistency. Emphasis has been placed in presenting the National Institute of Health and Clinical Excellence guidelines, which were originally designed for the UK. However, we believe that the principles presented in this review would be equally safe in other countries with similarly structured healthcare systems.
Introduction
Traumatic brain injury (TBI) is an insult or trauma to the brain caused by external mechanical forces, whereas head injury is a generic term referring to injuries affecting not only the brain but also other structures of the head. In the UK, every year 1500 per 100 000 of the population (total 900 000) attend emergency departments with a head injury, 225–300 per 100 000 are admitted to hospital, 10–15 per 100 000 are admitted to neurosurgical units (NSUs) and 6–10 per 100 000 die from TBI.1 ,2 An estimated 1.2 million people live with some level of TBI-related disability in the UK, which has profound socioeconomic consequences, as the prevalence is particularly high among children and young to middle-aged adults.3 Clinicians from many hospital specialties, general practitioners and allied healthcare professionals are regularly involved in providing direct care during the various phases of the treatment pathway for head-injured patients. This review aims to present the principles upon which modern TBI management should be based, using 12 practical questions.
What are the pathophysiological consequences of TBI?
Primary tissue disruption occurring at the time of injury is, in general, irreversible. Over the subsequent hours and days, a host of secondary insults that exacerbate the degree of injury ensue; however, these are potentially treatable. Cellular ischaemia, activation of inflammatory cascades, neuronal and astrocytic swelling, and vasogenic oedema are important mechanisms contributing to brain swelling.4 Within the rigid confines of the skull, brain swelling results in raised intracranial pressure (ICP) and reduced cerebral perfusion pressure (defined as mean arterial blood pressure minus ICP). Worsening cerebral ischaemia leads to a vicious circle, exacerbating swelling and ICP. The goal of treatment is to control ICP and maintain an adequate cerebral perfusion pressure in order to meet the demands of the injured brain.2
How is the severity of TBI initially determined?
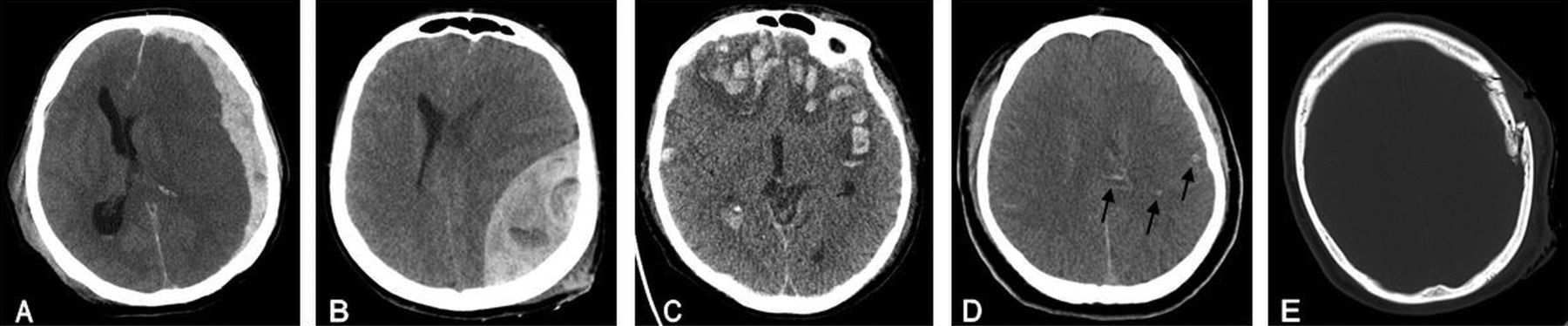
The Glasgow Coma Scale score (GCS) is used in the triage of patients early after TBI to indicate its severity. Approximately 90% of head-injured patients presenting to emergency departments have TBI that is mild (GCS 13–14) or minor (GCS 15); in 5%, the TBI is moderate (GCS 9–12) and in 5% it is severe (GCS 8 or less).5 TBI is usually divided into focal, diffuse and penetrating (figure 1).6 Blunt trauma usually results in focal injuries, whereas angular or rotational acceleration–deceleration forces (such as those experienced in high-speed road traffic collisions) cause diffuse injury by shearing of the brain tissue; both types of injury may coexist.7
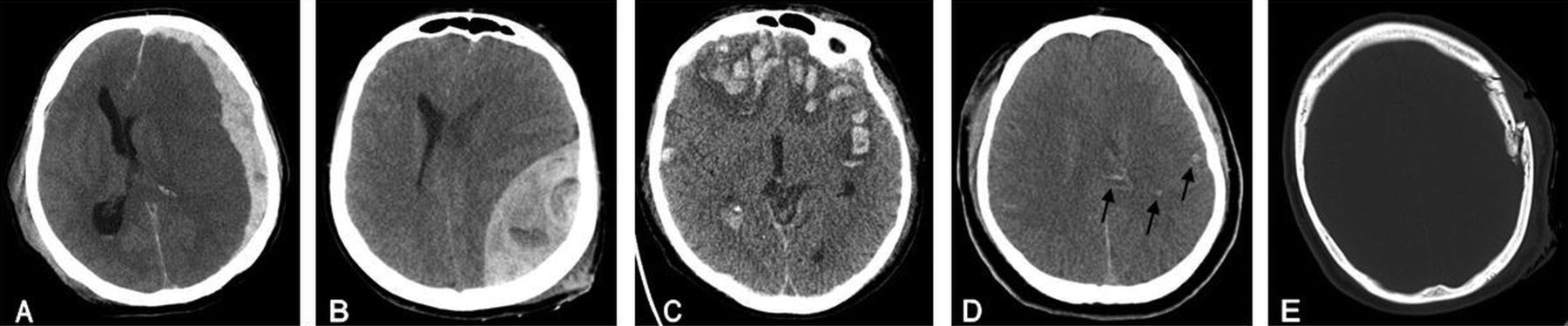
(A) Acute subdural haematoma with midline shift (note the crescent shape which is typical of these haematomas). (B) Acute extradural haematoma with midline shift (note the biconvex shape which is typical of these haematomas). (C) Contusions in both frontal and temporal lobes. (D) Diffuse brain injury (arrows indicate petechial haemorrhages in the splenium of the corpus callosum and grey–white matter junction). (E) Depressed skull fracture.
What is the initial management of TBI?
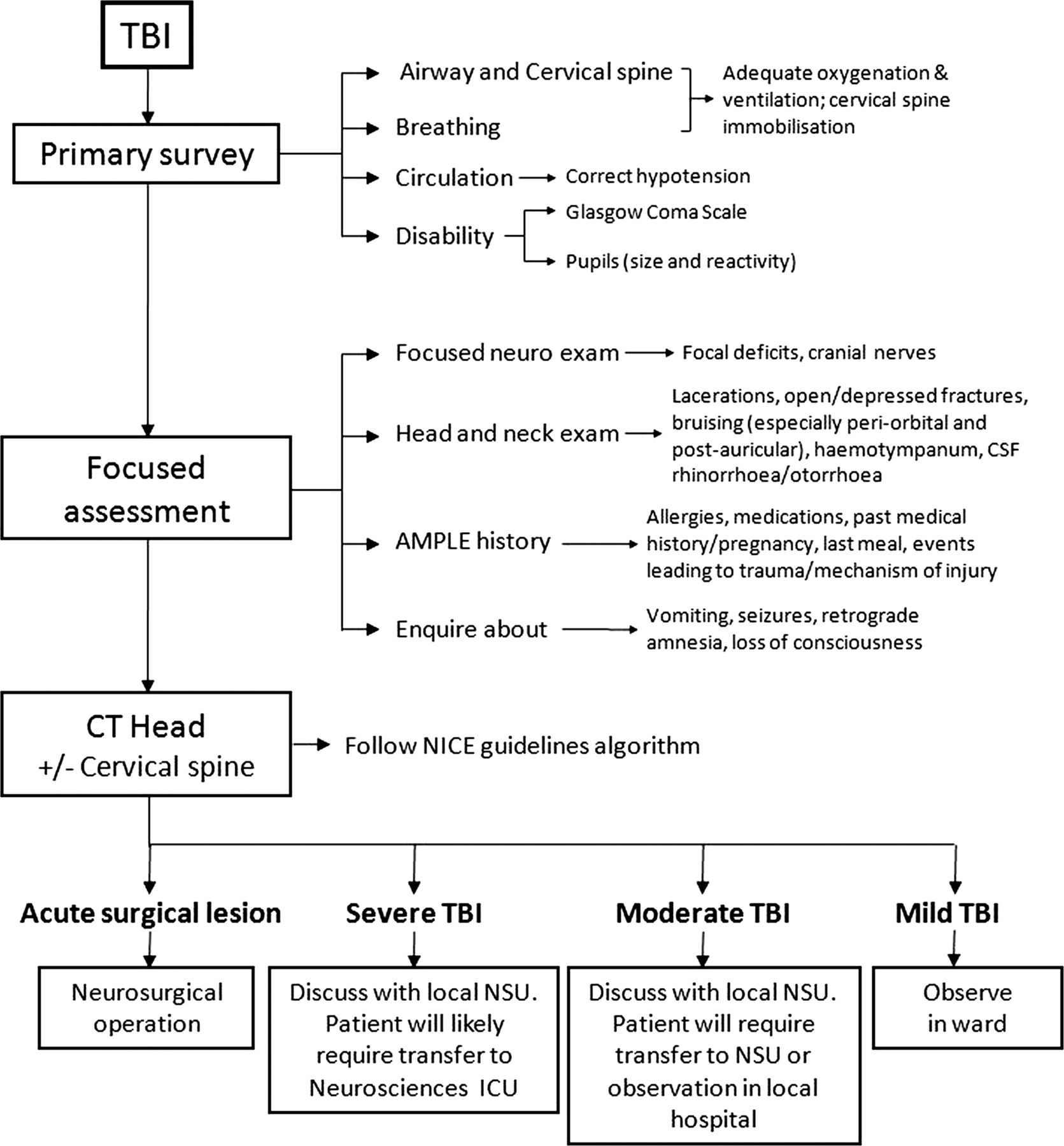
Management at the scene and in the emergency department should follow the principles of prehospital and advanced trauma life support courses (ie, assessment and treatment of the most urgent problems first in a systematic order; figure 2). Patients who are comatose or who have deteriorating consciousness should have their airway secured (if necessary with intubation), adequate oxygenation and ventilation, and fluid replacement to avoid hypotension.8 Spinal immobilisation should be maintained until clinical assessment and/or imaging studies indicate that it can be removed. In the emergency department, a primary survey and simultaneous resuscitation need to be undertaken for all head-injured patients, including those with mild TBI. Clinicians should also focus on TBI signs and symptoms (figure 2).
{kind=link}
{kind=link}
Initial management of traumatic brain injury (TBI). In addition to the above, patients with a deteriorating Glasgow Coma Scale score (GCS) (particularly deteriorating motor component), progressive neurological signs, penetrating injuries and cerebrospinal fluid (CSF) leak should also be discussed with the local neurosurgical unit (NSU). National Institute for Health and Clinical Excellence (NICE) guidance regarding the selection of adults for CT scanning of the head can be accessed online at http://www.nice.org.uk/nicemedia/live/11836/36257/36257.pdf. ICU, intensive care unit.
What are the indications for imaging?
Since 2003, the mainstay of risk stratification in the UK emergency departments has been a system of triage based on clinical assessment, which then dictates the need for a CT scan of the head. Such a system is important in order to identify early patients who have significant intracranial injury and are at risk of deteriorating; it also serves to identify injuries, such as cerebral contusions, which are relevant to prognosis and rehabilitation but do not necessarily require neurosurgical intervention. After a systematic review of published evidence, the National Institute for Health and Clinical Excellence (NICE) has adapted the Canadian CT Head Rule and provided recommendations for both CT head scanning and imaging of the cervical spine, with clear management algorithms.1 Essentially, head-injured patients who present with a GCS less than 13, or those failing to reach GCS 15 within 2 h of injury, need an urgent CT scan of the head. In addition, patients who are intubated or have a GCS less than 13 require a CT scan of the cervical spine.9
When to discuss with neurosurgery?
According to the NICE guidelines, patients with an abnormal CT head scan (haematomas, fractures), GCS of eight or less post-resuscitation, deteriorating GCS (particularly deteriorating motor component), progressive neurological signs, penetrating injuries and cerebrospinal fluid (CSF) leak should be discussed with the local NSU.9
Which patients should be transferred to neuroscience centres?
A large retrospective cohort study using prospectively recorded data from the Trauma and Audit Research Network database showed that since 2003 there has been an average 12% reduction in the adjusted log odds of death per annum in patients with TBI (n=15 173), following the introduction of the NICE guidelines and increased treatment of severe TBI in neuroscience centres.10 There is now increasing recognition that patients with severe and moderate TBI should be managed in neuroscience centres, regardless of the need for neurosurgical intervention (class II evidence).11 However, due to current resource constraints, in terms of neuroscience beds and staff, this may not always be possible. In such cases, ongoing liaison with a neurosurgeon over clinical management is essential. The Association of Anaesthetists of Great Britain and Ireland published a set of recommendations for the safe transfer of patients with brain injury in 2006. In general, patients with a GCS of eight or less requiring transfer should be intubated and ventilated.12 Although such transfers are often urgent, life-threatening extracranial injuries must be attended to at the referring hospital according to the advanced trauma life support guidelines, as haemodynamic and respiratory stability are a pre-requisite for a safe transfer.13 In the context of TBI with deteriorating consciousness, a new-onset unilateral pupillary dilatation indicates transtentorial herniation usually due to an expanding mass lesion. Administration of mannitol can buy time in such a situation; however, it should not be given to hypotensive patients.8
When to admit and discharge patients after TBI?
The Society of British Neurological Surgeons TBI working party recommends that patients with isolated mild TBI are best managed on observation wards under the care of emergency department staff.11 The objective of hospital admission for patients who do not require transfer to a NSU is to continue neurological observations, allow time for improvement in patients’ symptoms and to identify the small subset of patients who deteriorate. Patients usually require admission if they have an abnormal CT head scan (but do not require transfer to a neuroscience centre), GCS less than 15 regardless of CT findings or persistent symptoms (eg, vomiting, severe headaches, CSF leak).9 In general, patients can be discharged when their GCS has returned to the pre-injury level and major symptoms have resolved. The NICE guidelines recommend that all patients should be referred to their general practitioner for follow-up within 1 week after discharge.9
How are intracranial haematomas best managed?
Acute extra-axial haematomas (subdural or extradural), causing compression of the underlying brain with significant midline shift, are usually managed surgically. The management of traumatic intracerebral haematomas is more controversial, reflecting the lack of high-quality evidence. The Brain Trauma Foundation (BTF) evidence-based guidelines have defined threshold values for volume and thickness of haematomas that require evacuation (class II and III evidence).14 However, in practice, these cases should be discussed with a neurosurgeon. Other factors that may have an impact on the decision to operate include the size and location of the haematoma, swelling of the underlying brain, other major injuries, the patient's neurological state (including pupillary size and reactivity), age and comorbidities. Patients without neurological compromise and a small intracranial haematoma can be managed with careful, regular observation.14 Following systematic review of the literature, the BTF guidelines have recommended that time from clinical deterioration to operation should be kept to a minimum, as it can affect the outcome of patients with acute subdural or extradural haematomas.14
Levels of evidence used in Brain Trauma Foundation guidelines
How is severe TBI managed in intensive care?
Intensive care management of TBI focuses on maintaining physiological stability and preventing secondary brain injury. The BTF systematic review of the literature demonstrated that hypotension and hypoxia should be avoided, as they are associated with worse outcomes (class II and III evidence).15 Following trauma, the brain is particularly susceptible to physiological derangements; raised ICP and decreased cerebral perfusion pressure each independently predict poor outcome following TBI.16–18 ICP monitoring requires insertion of an invasive probe into the brain parenchyma or insertion of an external ventricular drain. The monitoring and treatment of raised ICP is paramount for maintaining blood supply and oxygen delivery. Although there is no class I evidence for management of ICP and cerebral perfusion pressure, there is abundant level II and III evidence.15 Targets for cerebral perfusion pressure (60–70 mm Hg) and ICP (less than 20–25 mm Hg) have been defined.15 In a recently published randomised trial, which recruited 324 patients with severe TBI in Bolivia and Ecuador, care focused on maintaining ICP at or below 20 mm Hg was not superior to care based on imaging and clinical examination.19 However, the selected composite primary endpoint, mainly focused on neuropsychological measures, was problematic and resulted in an underpowered study. For these reasons, we believe that ICP monitoring will remain a standard of care following severe TBI. Table 2 lists the range of interventions available in intensive care to control ICP. Many of these carry a risk to the patient: good intensive care requires a careful balance of the risks and benefits as well as management of complications.20
Methods of controlling raised intracranial pressure (ICP)
What are the complications of TBI?
Even mild TBI can be associated with a range of complications2; table 3 lists the most common of these.
Common complications of traumatic brain injury
What is the post-concussion syndrome?
The post-concussion syndrome is a common consequence of mild TBI, and comprises a range of non-specific symptoms, including headache, dizziness, fatigue, irritability, sleep disturbance, memory/concentration problems and affective disorders. It is usually self-limiting and resolves over weeks and months. However, in a subset of patients, the symptoms can be long standing and debilitating.21 Patients who have persistent post-concussion syndrome symptoms 4–6 weeks post-injury, should see their general practitioner. Although there is no specific proven treatment, supportive management in the context of a multi-disciplinary neurotrauma clinic and patient support groups (eg, Headway in the UK) can ameliorate the effects on the patient and their family.22 ,23
What is post-traumatic epilepsy?
Post-traumatic seizures are classified into early (within 1 week post-injury) and late (more than 1 week post-injury). Post-traumatic epilepsy can first manifest several years after injury and often has profound implications for patients’ quality of life and socioeconomic status. Long-term, post-traumatic epilepsy affects 10%–15% of patients after severe TBI. Its prevalence following moderate TBI is less than 5%, and there is only marginal excess risk over the general population after mild TBI.24 A recently published population-based cohort study from Denmark demonstrated that even though the risk of epilepsy was higher in the few years after the head injury, the excess risk continued for more than 10 years.25 Some neurosurgeons use short-term anti-epileptic prophylaxis for high-risk cases (eg, cortical contusion) as it has been shown to reduce the incidence of early seizures; however, there is no evidence supporting the use of long-term prophylaxis.26 All patients in the UK with seizures must inform the Driver and Vehicle Licensing Agency as they will be required to stop driving, at least in the short term.
What is the outcome after TBI?
Functional recovery from TBI is classified on the Glasgow Outcome Scale and is commonly dichotomised into favourable versus unfavourable outcome (table 4).27 Prognostic models derived from large prospective datasets have shown that age, severity of primary injury (measured by GCS, pupillary reaction and CT scan appearances) and major secondary insults including hypotension and hypoxia are the principal risk factors for death and long-term neurological morbidity.28 ,29 Approximately 40% of patients presenting in coma with severe TBI die and a further 20% survive with major disability, whereas patients with moderate TBI have around 10%–20% risk of death or severe disability.30 ,31 The overwhelming majority of patients with mild TBI make a good recovery even though cognitive deficits and symptoms are common in the acute stage.32 Predicting outcome for an individual patient is, however, notoriously difficult and a clear prognosis often emerges only over the days and weeks following injury. MRI of the brain may assist with prognostication of outcome.7
Glasgow Outcome Scale for classifying outcome following traumatic brain injury (TBI)
Why is rehabilitation important after TBI?
After TBI of any severity, a substantial proportion of patients display cognitive and emotional difficulties that, even without gross motor or sensory deficits, may preclude returning to work and other social activities. Rehabilitation after TBI is a complex process because patients’ individual needs evolve with time and depend upon the severity and type of TBI, pre-morbid functional status and levels of social support. The authors of a recent Cochrane review concluded that intensive intervention appears to lead to earlier gains.33 Earlier transfer to rehabilitation can improve functional outcome and lower both rehabilitation and acute hospitalisation costs.34 However, access to neurorehabilitation services remains restricted.11
Future directions
The numerous trials of neuroprotective agents in recent decades have had largely negative results; hence, there is still an unmet need for effective therapies against TBI. A major challenge is to improve trial design and validate new outcome scales to detect smaller but clinically meaningful treatment effects. Decompressive craniectomy, therapeutic hypothermia, hyperoxia (hyperbaric and normobaric) and progesterone are the subject of ongoing phase III randomised trials. Also underway are systematic studies of genetic risk factors in TBI that should improve prognostic models and suggest new treatment targets. As multimodality neuromonitoring (ICP waveform analysis, brain tissue oxygenation, microdialysis, advanced neuroimaging) becomes more established in the clinical arena, our ability to detect secondary insults and deliver individualised targeted interventions will improve.35 Therapeutic approaches that promote repair of the primary injury to the central nervous system, including stem cell treatments, remain experimental and have not yet been tested clinically.
Summary points
-
The early management phase following traumatic brain injury (TBI) aims to achieve haemodynamic stability, limit secondary insults (eg hypotension, hypoxia), obtain accurate neurological assessment and appropriately select patients for further investigation.
-
Since 2003, the mainstay of risk stratification in the UK emergency departments has been a system of triage based on clinical assessment, which then dictates the need for a CT scan of the head.
-
It is increasingly recognised that patients with severe and moderate TBI should be managed in neuroscience centres, regardless of their need for neurosurgical intervention.
-
For severe TBI, the monitoring and treatment of raised intracranial pressure is paramount for maintaining cerebral blood supply and oxygen delivery.
-
Specialist neurorehabilitation after TBI is important for improving outcome.
-
Continuing medical education resources box
-
Brain Trauma Foundation evidence-based guidelines: https://www.braintrauma.org/coma-guidelines/searchable-guidelines/.
-
Head injury review available online at Medscape reference: http://emedicine.medscape.com/article/1163653-overview.
-
Head injury module at http://www.ebrainjnc.com/register.html: ebrain supports training and continuous professional development for clinical neuroscience trainees and consultants, with much of the content also of relevance to non-specialists.
-
Traumatic brain injury: intensive care management. Br J Anaesth 2007;99:32–42. Review paper describing the management of severe TBI.
-
Information resources for patients
-
Headway is a UK charity set up to give help and support to people affected by brain injury http://www.headway.org.uk/About-Brain-Injury.aspx
-
Tips for non-specialists
-
Hypoxia and hypotension should be avoided.
-
Follow an evidence-based decision algorithm to decide the need for a CT head scan.
-
In a traumatic brain injury (TBI) patient with deteriorating consciousness and a new-onset unilateral pupillary dilatation, intravenous mannitol can buy time.
-
TBI is associated with a number of complications: some require specialist referral.
-
Patients with post-concussion syndrome can be helped by supportive management in the context of a multi-disciplinary neurotrauma clinic and by patient support groups.
Acknowledgments
AGK is supported by a Royal College of Surgeons of England Research Fellowship (funded by the Freemasons and Rosetrees Trust), a National Institute for Health Research Academic Clinical Fellowship, and a Raymond and Beverly Sackler Studentship. MRG is supported by a Royal College of Surgeons of England Research Fellowship and a Raymond and Beverly Sackler Studentship. AH is supported by a joint Royal College of Surgeons of England/Medical Research Council Clinical Research Training Fellowship and the Raymond and Beverley Sackler Fellowship. JA is supported by the Evelyn Trust. PJH is supported by an Academy of Medical Sciences/Health Foundation Senior Surgical Scientist Fellowship and the NIHR Cambridge Biomedical Research Centre.
References
Footnotes
-
Contributors AGK, MRG and AH drafted the article. JA and PJH revised the article critically. All authors have approved the final version to be published.
-
Competing interests None.
-
Provenance and peer review Commissioned. Externally peer reviewed. This paper was reviewed by Jakob Christiensen, Aarhus, Denmark.
Other content recommended for you
- Updates in traumatic brain injury management: brain oxygenation, middle meningeal artery embolization and new protocols
- Traumatic brain injury in England and Wales: prospective audit of epidemiology, complications and standardised mortality
- Concussion is confusing us all
- The Impact of Traumatic Brain Injury on Neurocognitive Outcomes in Children: a Systematic Review and Meta-Analysis
- Respect your elders: effects of ageing on intracranial pressure monitor use in traumatic brain injury
- Factors predicting mortality in victims of blunt trauma brain injury in emergency department settings
- Incorporating age improves the Glasgow Coma Scale score for predicting mortality from traumatic brain injury
- Comparative effectiveness of surgery in traumatic acute subdural and intracerebral haematoma: study protocol for a prospective observational study within CENTER-TBI and Net-QuRe
- Clinical characteristics and outcomes of traumatic brain injury in patients admitted to surgical ward of Jimma Medical Center, Southwest Ethiopia: a prospective observational follow-up study
- Discrepancy between disability and reported well-being after traumatic brain injury