Article Text

Abstract
Amyloid positron emission tomography (PET) imaging enables in vivo detection of brain Aβ deposition, one of the neuropathological hallmarks of Alzheimer’s disease. There is increasing evidence to support its clinical utility, with major studies showing that amyloid PET imaging improves diagnostic accuracy, increases diagnostic certainty and results in therapeutic changes. The Amyloid Imaging Taskforce has developed appropriate use criteria to guide clinicians by predefining certain scenarios where amyloid PET would be justified. This review provides a practical guide on how and when to use amyloid PET, based on the available research and our own experience. We discuss its three main appropriate indications and illustrate these with clinical cases. We stress the importance of a multidisciplinary approach when deciding who might benefit from amyloid PET imaging. Finally, we highlight some practical points and common pitfalls in its interpretation.
- ALZHEIMER’S DISEASE
- AMYLOID
- BEHAVIOURAL DISORDER
- VISUAL ATTENTION
- ATTENTION
- COGNITIVE NEUROPSYCHOLOGY
- COGNITION
Statistics from Altmetric.com
- ALZHEIMER’S DISEASE
- AMYLOID
- BEHAVIOURAL DISORDER
- VISUAL ATTENTION
- ATTENTION
- COGNITIVE NEUROPSYCHOLOGY
- COGNITION
INTRODUCTION
Amyloid positron emission tomography (PET) imaging is a relatively new diagnostic investigation enabling in vivo detection of fibrillar Aβ plaques, a pathological hallmark of Alzheimer’s disease (AD), with very high sensitivity and specificity.1–3 It has revolutionised Alzheimer’s research and has increased the understanding of how Aβ deposition relates to cognitive and functional decline, brain atrophy and hypometabolism, both cross-sectionally and longitudinally.4 Furthermore, clinical trials of AD therapeutics have widely adopted amyloid PET in order to enrich the sample for amyloid beta (Aβ)-positive participants and to evaluate treatment effects on amyloid deposition. The European Medicines Agency and the US Food and Drug Administration have approved three fluorinated amyloid PET tracers (18F-florbetapir, 18F-florbetaben and 18F-flutemetamol) for clinical use. Currently, one tracer (18F-florbetaben) is commercially available in the UK. Although its cost effectiveness is still being evaluated and its availability is limited to the specialist centres, a growing body of evidence supports its clinical utility. It appears most helpful for people with atypical and young-onset cognitive impairment, or in those with a confounding neurological or psychiatric condition (see 'Dementia with atypical clinical course or aetiologically mixed presentation'), and thus is often relevant to cases that present to neurologists.
We have used amyloid PET imaging as part of our clinical service since 2013 and have scanned over 400 patients. Here we provide a practical guide on how and when to use amyloid PET based on the available research and our own experience.
WHAT IS THE WIDER CONTEXT? ADVENT OF AD BIOMARKERS AND DIAGNOSTIC PARADIGM SHIFT
The advent of neuroimaging and molecular biomarkers of AD, including amyloid PET as well as cerebrospinal fluid (CSF) analysis for Aβ 1–42 and tau, has changed the dementia field of over the past 20 years. There has been a conceptual shift in the diagnostic framework from defining AD as a clinical syndrome towards a biological definition.5 This change was reflected in the revised diagnostic criteria for AD proposed by the International Working Group and the National Institute of Aging–Alzheimer’s Association (NIA-AA), which now incorporate the use of biomarkers in the diagnosis of AD.6 7 In addition, atypical presentations of AD have been recognised, such that memory impairment is no longer required for diagnosis, as long as biomarker evidence is available. Furthermore, for research purposes, the new criteria for AD acknowledge that biomarker abnormalities may precede clinical symptoms. Thus, preclinical AD is defined by the presence of biomarker evidence of Alzheimer’s pathological changes in cognitively healthy people.8 9 The recently updated NIA-AA research framework further defines AD as a pathological process that is identified primarily by biomarkers and treats cognitive impairment as a symptom or sign of the disease rather than the definition of the disease.5
WHY USE AMYLOID PET? AN IN VIVO SURROGATE OF Aβ DEPOSITION
Pittsburgh compound B was the first amyloid PET tracer to be described and is the most extensively researched. It has a nanomolar affinity for fibrillar amyloid, but its short 20-min half-life limits any routine clinical application.10 Newer amyloid PET tracers have been developed, which use fluorine-18 radioisotope with a longer half-life (110 min); three of them—florbetapir, florbetaben and flutemetamol—are licenced for clinical use, with florbetaben being available in the UK. The postmortem studies correlating tracer uptake to pathologically detected amyloid demonstrated sensitivities of 91–98% and specificities of 89–100% across amyloid PET ligands,1 2 11 12 making amyloid PET a valid in vivo surrogate of amyloid deposition.
The most prevalent theory of AD pathogenesis suggests that it begins with abnormal processing of amyloid precursor protein, which then leads to the accumulation of abnormally folded Aβ in the cortex.13 This is followed by the formation of neurofibrillary tangles (comprising phosphorylated tau) and subsequent neuronal dysfunction and neurodegeneration (which can be measured by 18F-FDG PET hypometabolism, CSF total tau and atrophy on MR), perhaps mediated via inflammation.14 Studies using amyloid PET imaging in healthy elderly people and patients with both sporadic15 and familial AD16 show that amyloid pathology develops approximately 10–20 years before the onset of clinical symptoms and precedes tau pathology, which in turn predates MR atrophy and the onset of clinical symptoms. Biomarkers of Aβ therefore indicate initiating upstream events, while neurodegenerative biomarkers such as fluorodeoxyglucose (FDG)-PET reflect the downstream pathophysiological processes that follow (see box 1 for further discussion on the role of FDG-PET in the evaluation of patients with cognitive impairment and its comparison with amyloid PET). Consequently, studies have confirmed that AD clinical symptoms are coupled to neurodegeneration rather than amyloid deposition, with the neurodegenerative biomarkers (not the amyloid deposition) predicting the rate of cognitive decline17–19
Box 1 Amyloid PET versus 18F-FDG-PET
FDG-PET imaging is a reflection of glucose metabolism within a tissue with decreased activity in regions of neuronal dysfunction and degeneration. It therefore acts as a marker for neuronal loss but is not disease specific, and in contrast to amyloid PET, it does not indicate the underlying pathology.
Amyloid plaque accumulation usually occurs several years before structural and metabolic (FDG) changes are seen, and even before symptoms of cognitive impairment.
The typical spatial pattern of FDG-PET hypometabolism in AD involves the posterior cingulate gyrus, limbic system, temporal lobes, precuneus, parietal cortex and, in advanced cases, the prefrontal cortex. In turn, amyloid PET interpretation is binary (either positive or negative) and the regional amyloid distribution does not correlate directly with the severity or type of AD presentation.
While the patterns of hypometabolism on FDG-PET can be used to subtype dementia syndromes at a group level, it lacks specificity on an individual patient basis. The FDG-PET findings can often be atypical or non-specific; even the ‘typical’ hypometabolism patterns can overlap between dementia subtypes (eg AD and frontotemporal dementia).
FDG-PET can help when looking for an underlying neurodegenerative brain disease in cases where the differential still includes the absence of brain disease (eg, psychological, psychiatric or metabolic presentations) and the MR brain appears within normal limits. If, however, MR scan shows focal lobar atrophy, then FDG-PET seldom adds to the picture as it typically shows hypometabolism in the atrophic regions.
Although FDG-PET is the nuclear imaging modality recommended by NICE (2018) for diagnosing dementia subtypes in a specialist clinical setting, these guidelines were produced before several recent studies demonstrated the clinical utility of amyloid PET imaging. While FDG-PET still has a role to play, we find amyloid PET is more helpful in a large proportion of cases. We suggest that where amyloid or FDGPET are both indicated (and available), amyloid PET would be preferable if AD is part of the differential diagnosis.
AD, Alzheimer’s disease; FDG-PET, fluorodeoxyglucose-positron emission tomography; NICE, National Institute for Health and Care Excellence.
While brain amyloidosis is a necessary condition for diagnosing AD, significant plaque deposition alone is not sufficient to produce cognitive decline. This is illustrated by the fact that 20–40% of cognitively healthy people older than 60 years have elevated levels of cerebral Aβ.20–22 Therefore, the negative predictive value of amyloid PET is very high—a negative amyloid PET essentially eliminates the diagnosis of AD. Conversely, a positive amyloid PET scan on its own is not sufficient to diagnose AD, but rather is a sensitive and specific marker of the presence of amyloid deposition. Therefore, the implications of a positive scan depend on whether a person is asymptomatic, or whether they have symptoms and signs of cognitive impairment.23 As amyloid deposition occurs pre-symptomatically in disease progression, it does not help as a clinical staging marker or index of pathological progression. Moreover, deciding which patients to scan in real-life clinical settings requires careful consideration and a multidisciplinary team approach.
WHEN TO USE AMYLOID PET? APPROPRIATE USE CRITERIA
The Amyloid Imaging Taskforce, convened by the Society of Nuclear Medicine and Molecular Imaging and the Alzheimer’s Association, produced a set of appropriate use criteria in 2013.24 These defined the types of patients and clinical circumstances (summarised in table 1) in which amyloid PET ought to be used, and have been used to inform guidelines published by other organisations.25 26
Appropriate use criteria for amyloid PET (adapted from Johnson et al)
The Amyloid Imaging Taskforce recommendations emphasise that clinical assessment and examination remain the key clinical tools in the diagnosis of AD, with amyloid PET reserved for cases of diagnostic uncertainty. According to the taskforce criteria, amyloid PET should be restricted to patients with a cognitive impairment of uncertain cause in whom AD is as a possible diagnosis. In this group, determining the presence or absence of Aβ pathology increases diagnostic certainty and affects management approaches. The taskforce further specified three general clinical scenarios in which amyloid PET imaging is appropriate: (i) persistent mild cognitive impairment (MCI), (ii) dementia with either atypical clinical course or aetiologically mixed presentation, and (iii) dementia with atypically early age of onset (usually defined as ≤65 years of age). Inappropriate clinical uses include further testing of patients with a highly certain diagnosis of AD, screening of asymptomatic people, evaluation of patients with no objective cognitive abnormality, even with a family history or known APOE4 allele or as an attempt to determine the severity of dementia.
Although some authors suggest that the current appropriate use criteria do not discriminate between patients who will benefit from amyloid PET and those who will not,27 the Amyloid Imaging Taskforce criteria provide an operational framework that most centres, including ours, have adopted, including ours. We will briefly discuss three main appropriate indications for amyloid PET, each illustrated with a clinical case, although it should be noted that some of the cases manifest more than one criterion.
(i) Persistent or progressive unexplained MCI
People with MCI comprise a heterogeneous group with a wide spectrum of underlying pathologies.28 Amyloid PET is useful for discriminating between patients with MCI who do and do not have AD pathology. Approximately 50–70% of people with MCI have high levels of cortical amyloid deposition.18 22 29 30 The presence of amyloid accumulation correlates highly with progression from MCI to Alzheimer’s dementia.29 31–34 The analysis of 684 subjects from the AD Neuroimaging Initiative cohort showed that 5-year conversion rates to AD in cognitively impaired subjects were 78% in amyloid+/FDG+ subjects and 42% in amyloid+/FDG− patients, while amyloid−/FDG− and amyloid−/FDG+ conversion rates were 5% and 22%, respectively. Amyloid PET predicted conversion to AD with 72% accuracy.34
Note, however, that asymptomatic brain amyloidosis is strongly associated with age—a large metanalysis showed that at the age of 90, about 40% of the apolipoprotein E4 (APOE4) noncarriers and more than 80% of APOE4 carriers with normal cognition are amyloid positive.22 Therefore, amyloid positivity in elderly patients may not relate to their cognitive symptoms or might be a secondary cause of cognitive impairment.
Given its moderate positive predictive value and the potential confound of age-associated increase in prevalence of cortical amyloid, the diagnostic value of amyloid PET in patients with MCI is more exclusionary, allowing Aβ pathology to be ruled out as a basis for the clinical syndrome. Such scenarios are frequent in patients with MCI who have multiple comorbidities where the clinical picture is complicated with potential vascular, traumatic, surgical or medical causes of cognitive impairment. Case 1 illustrates how amyloid PET was used to effectively exclude AD pathology in a patient with MCI, who was subsequently diagnosed with frontotemporal dementia, confirmed on genetic testing.
(ii) Dementia with atypical clinical course or aetiologically mixed presentation
This indication aims to include patients with established dementia in whom there is substantial uncertainty as to whether the dementia is secondary to AD pathology. This uncertainty can arise from (a) the presence of an atypical (ie, non-amnestic) presentation or unusual clinical course (eg, sudden onset, episodic, rapidly progressive) or (b) the presence of comorbid conditions that can also cause cognitive impairment.
Atypical AD syndromes include progressive aphasia, posterior cortical atrophy, corticobasal syndrome and frontal variant of AD (behavioural/dysexecutive syndrome).35 These may mimic the clinical phenotypes of other proteinopathies including primary tauopathies, TDP-43 (TAR DNA-binding protein 43) proteinopathies or synucleinopathies.28 As these atypical AD syndromes often have less clear-cut CSF profiles than are normally seen in typical AD, amyloid PET is a particularly useful biomarker in such cases.36
Studies have shown the benefit of amyloid PET imaging in differentiating between atypical AD and frontotemporal dementia, especially in the initial stages of the disease.37–39 Both conditions can present as progressive aphasia, and the frontal variant of AD may closely resemble behavioural frontotemporal dementia. Amyloid imaging has also been particularly useful to ascertain the absence of AD pathology in patients with primary progressive aphasia (PPA),40–42 a heterogeneous syndrome with different subtypes and neuropathological causes that can be difficult to discriminate clinically. Consensus clinical diagnostic criteria describe three major forms of primary progressive aphasia: non-fluent (nfvPPA), semantic (svPPA) and logopenic variant (lvPPA), with clinicopathologic studies most often linking nfvPPA to tau pathology,43 44 svPPA to TDP43-positive pathology45 and lvPPA to AD pathology.46 In practice, many patients do not easily fit into one clinical category, and amyloid PET can improve diagnostic accuracy.
Similarly, amyloid PET can provide invaluable evidence for underlying AD in patients with posterior cortical atrophy47 48 or corticobasal syndrome,49 both of which can have different underlying pathologies. It is important to note that despite striking focality of the symptoms and structural imaging changes in posterior cortical atrophy, amyloid deposition usually occurs across the cortex, with amyloid PET scans from such patients often being indistinguishable from those with typical AD.47 Therefore, while amyloid PET has a role in defining underlying pathology, it is not useful in defining AD syndromes. Case 2 illustrates the use of amyloid PET in a patient with atypical visuospatial presentation of AD and inconclusive CSF results.
Finally, various coexistent comorbidities may affect cognition, sometimes making the diagnosis of AD particularly difficult. These include psychiatric disease, cerebrovascular disease, traumatic brain injury, alcohol dependence, neuroinflammatory disease and vitamin B12 deficiency.50 51 In such cases, amyloid PET can provide crucial diagnostic clarity. Psychiatric disease in particular, such as treatment-resistant depression, may be a presenting feature of AD.52–56 In these cases, investigations such as MR and neuropsychology cannot always reliably differentiate between psychiatric disease without underlying neurodegeneration, and AD presenting with depression and/or anxiety, and amyloid PET can help in making this distinction.57
(iii) Dementia with early age of onset (<65 years)
The Amyloid Imaging Taskforce appropriate use criteria also include the use of amyloid PET in patients with early-onset progressive cognitive decline (≤65 years). It may be used in patients who manifest common clinical features of AD as well as those who do not, noting that people with younger-onset AD more likely have atypical features.58 Enabling diagnosis in this group is particularly important. The Royal College of Psychiatrists (UK) report into young-onset dementia noted that young-onset patients and their families often experience a considerable delay in getting a diagnosis and then accessing appropriate support, seeing an average of two to five consultants before a diagnosis is made. The negative impact of a delayed or erroneous diagnosis is considerable, through family stress and loss of earnings, as well as delays in starting treatment and potentially missing opportunities to participate in clinical trials.59
HOW TO USE AMYLOID PET? CRUCIAL ROLE OF THE MULTIDISCIPLINARY TEAM APPROACH AND INTERPRETATION PITFALLS
The Amyloid Imaging Taskforce criteria highlight the need to integrate imaging with comprehensive clinical and cognitive evaluation performed by a dementia expert in order to maximise the likelihood that amyloid-PET imaging will contribute to the patient’s management. In our centre, patients are first assessed by an experienced cognitive neurologist and subsequently undergo a set of investigations (eg, dementia bloods, MR scan of brain). Clinical details and test results are discussed with a detailed review of structural imaging at a cognitive neuroradiology multidisciplinary team meeting, where a decision to perform amyloid-PET is made by consensus between neuroradiologists, nuclear medicine specialists, old age psychiatrists, care of the elderly physicians and cognitive neurologists, as per the Amyloid Imaging Taskforce.24 On the day that suitable patients attend for scanning, they receive an injection of the PET tracer, and then after a 30–90-min delay, they are scanned for approximately 10–20 min, depending on the type of tracer used. During this time, they need to lie still in the scanner, strapped into a headrest. Radiation exposure is around 4–7 mSv, which is approximately 2.5 times the amount of background radiation to which a UK citizen is exposed over a year.
Interpretation of all amyloid PET scans is binary, that is, it is reported as either positive or negative. Two accredited readers report the scans—this is particularly important where there is any ambiguity. Note that the amount of amyloid burden in the brain does not correlate directly with the severity or type of AD presentation. Furthermore, amyloid deposition on PET does not seem to follow a sequential topographic progression through the isocortex.60 A positive result indicates moderate or high levels of cerebral amyloid plaque deposition, which is considered to support a clinical diagnosis of AD. A negative scan indicates absent or sparse levels of cerebral amyloid plaque deposition, which would not commonly support a clinical diagnosis of AD (figure 1A and B).
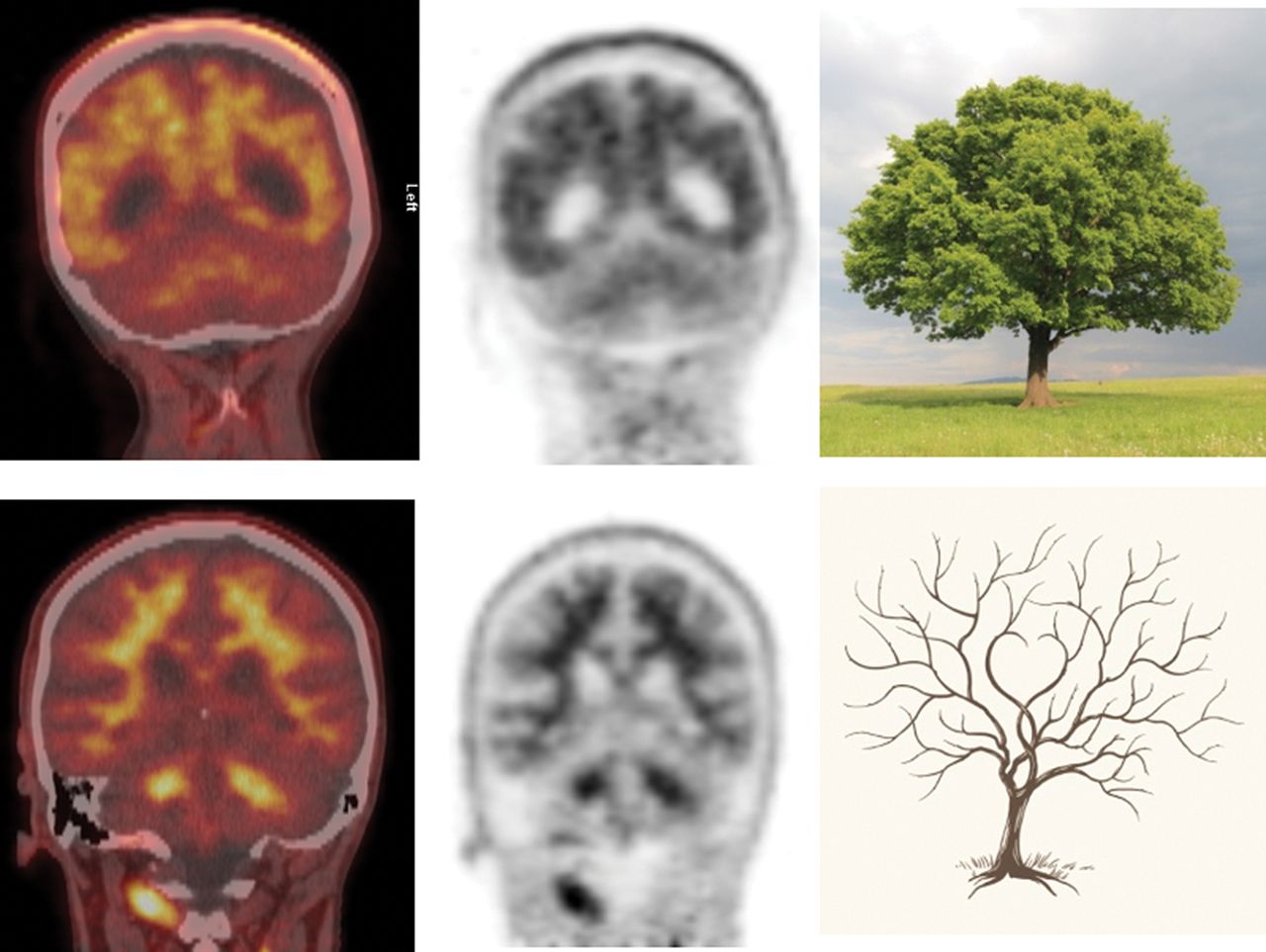
Amyloid PET interpretation (adapted from Dumba et al 24). (A) ‘Tree-in-bloom’ sign with loss of cerebral grey–white matter differentiation indicating a positive scan. (B) ‘Branching tree’ sign with good grey–white matter differentiation indicating a negative scan. PET, positron emission tomography. With permission, Dr Zarni Win.
Positive scans, using 18F-florbetapir, have either two or more brain areas of reduced or absent grey–white differentiation, or one or more areas in which grey matter activity is intense and clearly exceeds activity in adjacent white matter (see figure 1A and B). Not all scans are easy to read—visual interpretation of 18F amyloid tracers is technically challenging and requires experienced raters. In our experience, most scans (85–90%) are ‘type A’ (common or typical appearance) and this correlates with high inter-observer agreement and a high confidence of read.23 The confidence of read is lower when reporting ‘non-type A scans’ (atypical or less common appearance).23
It is important to emphasise that amyloid positivity does not establish the diagnosis of AD or necessarily differentiate it from other disorders where Aβ deposition may occur, such as dementia with Lewy bodies and cerebral amyloid angiopathy.24 In particular, cerebral amyloid angiopathy—a common vasculopathy characterised by Aβ deposition within the walls of small arterioles and capillaries of the leptomeninges and cerebral cortex—often co-occurs with parenchymal amyloid deposition.61 A recent meta-analysis62 showed that cerebral amyloid angiopathy (without dementia) is, at the group level, associated with higher global amyloid-PET burden when compared with age-matched healthy controls and patients presenting with spontaneous deep intracerebral haemorrhage. A negative amyloid PET scan could therefore help to exclude cerebral amyloid angiopathy; however if positive, differentiation from underlying AD is challenging.23 So far no approach (regional values, ratios, visual assessment) seems specific enough to discriminate cerebral amyloid angiopathy from AD, which may in part reflect the neuropathological overlap between these two amyloidopathies.63 Thus, careful clinical assessment is essential before requesting the scan.
Case 1. Amyloid Imaging Taskforce indication 1: patients with persistent or progressive unexplained MCI
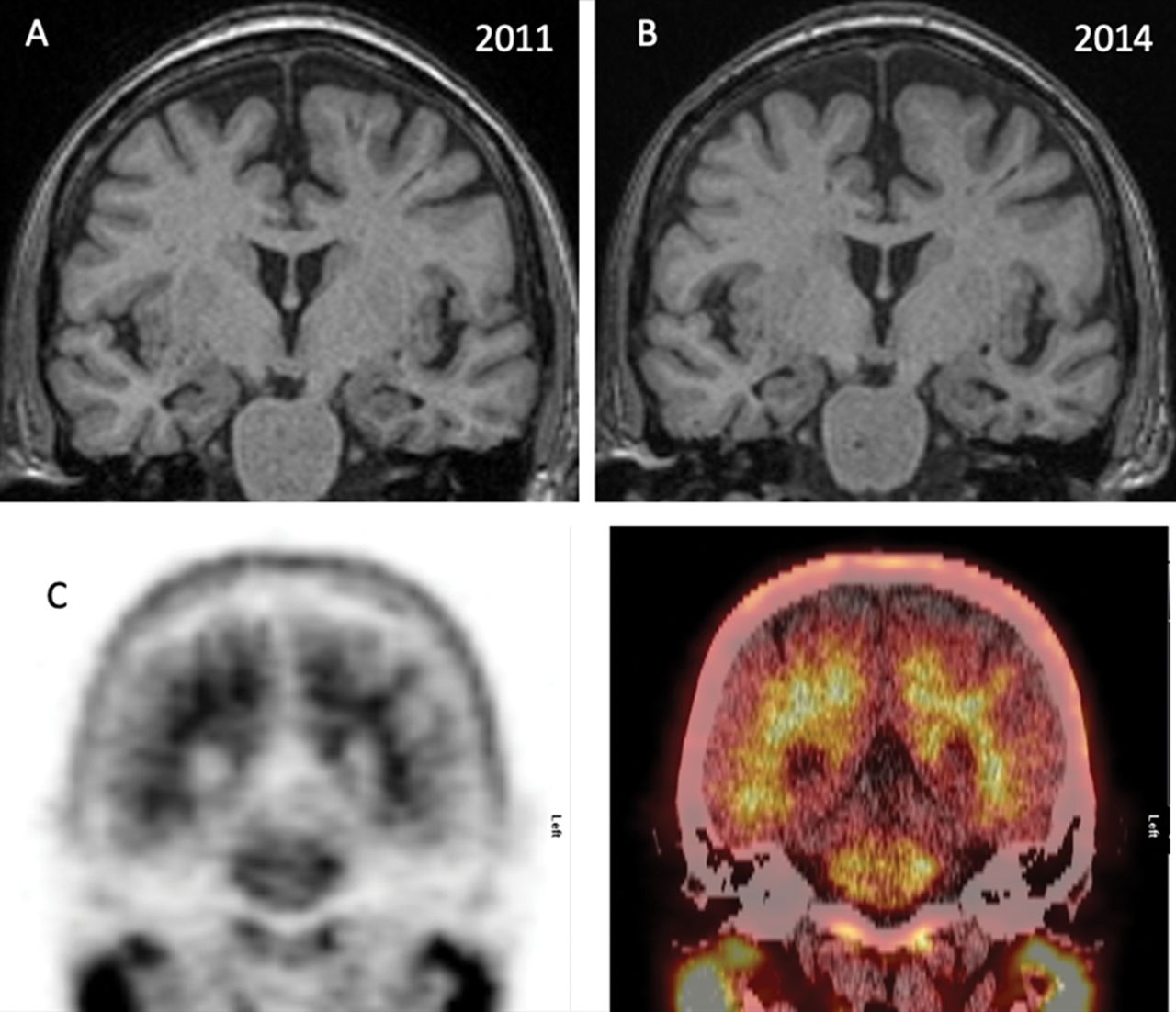
A woman presented with a 2-year history of short-term memory difficulties that had begun in her late 50s. However, she was living independently, still doing her own finances, shopping and keeping up with appointments using lists and calendars. She described a family history of AD in her father and two cousins. She performed well on bedside testing, and her initial neuropsychological assessment showed no definite objective abnormality. Her MR brain was reported as normal (figure 2A) and CSF examination showed normal Aβ 1–42 level of 611 pg/mL (>171pg/mLi) and elevated total tau level of 585 pg/mL (<377 pg/mL). Despite relatively normal investigations, she and her family remained concerned about her memory. Neuropsychological tests repeated 2 years after initial presentation showed some impairment of episodic memory. A repeat MR scan (figure 2B) showed no significant change from previous scans. Review of all previous imaging suggested that the hippocampal volumes might be mildly reduced bilaterally but unchanged since 2011. The multidisciplinary team agreed that amyloid PET imaging would be useful to exclude AD pathology as a basis for persistent and progressive MCI, as the MR appearances and neuropsychological testing did not explain the nature of patient’s problems. Amyloid PET was negative (figure 2C). Given ongoing cognitive problems and a family history of dementia, she underwent genetic testing for frontotemporal dementia, which has shown a heterozygous mutation in the granulin gene (GRN):C.1446 C>A p.(Cys482*).
Over the following years, there has been a steady decline in her cognitive function (mini-mental state examination (MMSE) Score 27/30 in 2016 18/30 in 2018), with the development of obsessive behaviours and occasional disinhibition. She is now participating in research studies for frontotemporal dementia.

MR scan of brain T1-weighted coronal images showing little change in hippocampal volume between 2011 (A) and 2014 (B). The amyloid PET scan was negative (C) with a clear differentiation between grey and white matter and absence of tracer uptake in the cerebral grey matter. PET, positron emission tomography.
Case 2. Amyloid Imaging Taskforce indication 2: patients satisfying core clinical criteria for possible AD (ie, atypical clinical course or aetiologically mixed presentation)
A woman in her early 60s presented with a 5-year history of cognitive difficulties, which had gradually progressed with a more rapid deterioration in the preceding 2 years. She was unable to keep up with her job or do her own finances. When she first presented to local memory services, her Addenbrookes Cogntive Examination (ACE)-Revised score was 76/100, MMSE was 27/30 and she was diagnosed with MCI. She was reassessed 3 years later at another hospital, and at that time her ACE score was 63/100 and MMSE was 19/30. It was felt that most of her problems were secondary to emotional issues and that there was a major affective component to her symptoms. She was referred for psychological therapy.
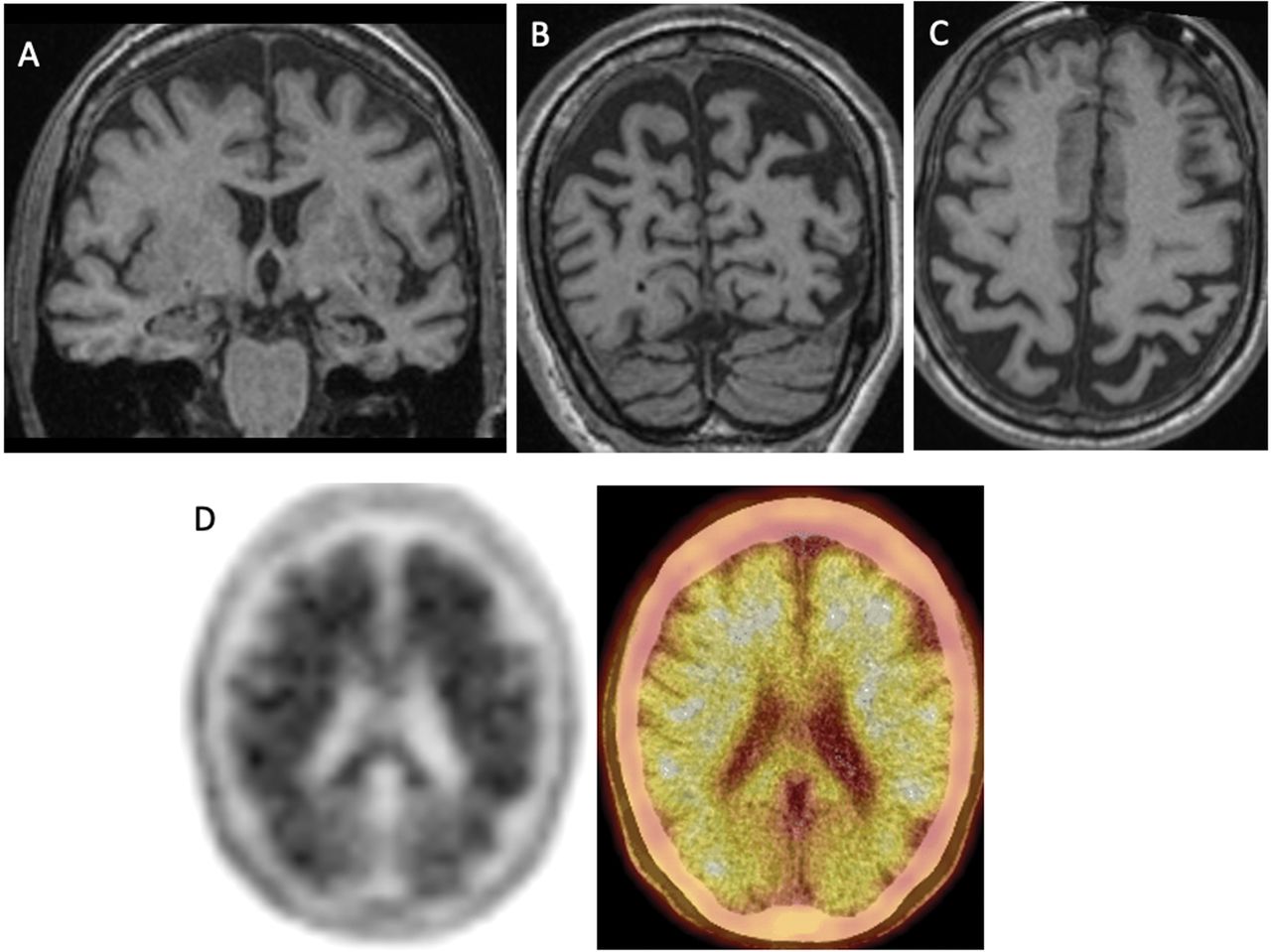
On her first assessment in our clinic, her score on the ACE was 22/100 and MMSE score was 10/30. There was prominent visuospatial impairment and apraxia on examination. Formal neuropsychological testing identified impairment in almost all cognitive domains. The MR scan of brain showed significant atrophy predominantly in the parieto-occipital lobes, with the mesial temporal lobes affected to a much lesser degree (figure 3A– C). CSF analysis showed raised CSF total tau of 1118 pg/mL (<320 pg/mL) with normal CSF Aβ 1–42 of 579 pg/mL (>220 pg/mL). We suspected corticobasal degeneration or a posterior cortical atrophy variant of AD. The multidisciplinary team agreed that amyloid PET would help to determine whether the dementia was secondary to AD pathology. The scan was positive (figure 3D) and a diagnosis of AD was made. She was then started on cholinesterase inhibitor treatment.

MR scan of brain T1-weighted coronal (A,B) and axial (C) images showing severe marked parietal atrophy with the prominence of sulci and CSF spaces predominantly in the parietal lobes. There is an asymmetrical atrophy of the left hippocampus (A). Amyloid PET scan (D) shows a widespread tracer uptake with loss of grey-white differentiation indicating moderate or severe amyloid plaque deposition. PET, positron emission tomography.
Case 3. Amyloid Imaging Taskforce indication 3: patients with atypically young-onset dementia (<65 years)
A woman in her late 40s presented with a 2-year history of memory problems and word-finding difficulties. She had to be signed off work because of her memory dysfunction and struggled with activities of daily living such as using her mobile phone or remembering her computer password. However, she was still driving and doing her own finances. Her maternal uncle, grandmother and great-aunt all developed dementia in their 50s or 60s. She was initially seen in a general neurology clinic where it was felt that low mood was a significant contributor towards her cognitive problems. She was referred for neuropsychological testing but unfortunately could not complete it as she became very emotional during the appointment. An urgent psychiatric opinion was advised and she was subsequently admitted to a private psychiatric health clinic, from where she was referred to our cognitive neurology clinic. On her first assessment, her ACE score was 64/100 and MMSE was 23/30. There was impairment across all domains with profound speech deficits. Her MR scan of brain showed generalised minor prominence of CSF spaces and prominent colloidal fissures, indicating minor hippocampal volume loss (figure 4A and B). Following discussion at the multidisciplinary team meeting, she fulfilled Amyloid Imaging Taskforce appropriate use criteria (young-onset dementia) and went on to have a florbetapir PET scan, which was positive (figure 4C and D), providing evidence for an underlying diagnosis of AD. She was then started on donepezil, and introduced to an Alzheimer’s Society support worker as well as being enrolled into a clinical trial.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
MR scan of brain T1-weighted coronal (A) and sagittal (B) images showing mild widening of the parieto-occipital sulci and widening of the choroid fissures (left greater than right). Amyloid PET scan (C) was positive with marked patchy loss of grey–white differentiation and abnormal tracer uptake within the grey matter within the cerebral cortex. The characteristic ‘tree-in-bloom’ appearance on coronal images is seen (D). PET, positron emission tomography.
HOW MUCH DIFFERENCE DOES IT MAKE? CLINICAL UTILITY
There is increasing evidence to suggest that amyloid PET improves diagnostic accuracy, increases diagnostic certainty and results in therapeutic changes. Several retrospective and prospective studies investigating the clinical utility of amyloid PET have reported changes in diagnosis varying from 9% to 55% and changes in clinical management in 37–87% of patients.36 64–72 A recent review pooled the results from several studies investigating the clinical utility of amyloid imaging and reported that mean weighted (by the study cohort size) change in diagnosis was 29% post amyloid imaging and change in patient treatment was 64%.73 Another systematic review and aggregated analysis on the impact of amyloid PET in 1142 patients show that its use in the absence of CSF or FDG-PET prompts a diagnosis change in up to 31.3% cases.74
However, most of these published studies included selected research populations, which may differ from clinical populations, and the research inclusion criteria often differed from the Amyloid Imaging Taskforce appropriate use criteria for amyloid PET. More recent studies with large unselected cohorts of patients in the ‘real-world’ clinical settings have confirmed that the addition of amyloid PET to the routine investigations in patients with cognitive impairment significantly affected diagnosis, diagnostic confidence and drug treatment. For example, the Alzheimer's biomarkers in daily practice (ABIDE) project showed that in a large unselected memory clinic cohort of 507 patients, amyloid imaging led to a diagnosis change in 25% of patients (28% in patients who met the Amyloid Imaging Taskforce appropriate use criteria, and 23% in those who did not; for example, patients with subjective cognitive decline).75 The study reported an average increase in diagnostic confidence of 10%, while changes in clinical management post-amyloid PET occurred in 60.2% of patients with MCI and 63.5% of patients with dementia.
These findings are consistent with our own experience. To date, 394 patients have undergone amyloid PET imaging in our tertiary cognitive neurology clinic as part of their diagnostic work-up. Their median age was 67.8 years (range 41–92 years). Positive scans represented 45.9% of the whole cohort (n=181). A retrospective analysis of the first 100 patients found that almost half were amyloid positive and the post-amyloid change in diagnosis occurred in 30% of patients.76 Clinical management was altered in 42% of cases, with changes including initiation of new medication and enrolment into clinical trials. Critically, use of amyloid PET also led to fewer further investigations. Furthermore, these data do not take into account the psychosocial effects of the investigation. Many patients with atypical diagnosis may wait several years before being given a diagnosis, and in our experience, amyloid PET has reduced this time. Conversely, it can particularly help in effectively ruling out AD in people who have previously received this diagnosis on clinical grounds alone.
Further evidence for the usefulness of amyloid PET was provided by the large-scale Imaging Dementia—Evidence for Amyloid Scanning (IDEAS) study. This US-based, single-group, multisite longitudinal study assessed its utility in 11 409 Medicare beneficiaries who met appropriate use criteria for amyloid PET. The first phase of the study’s results supported the relationship between amyloid PET findings and post-imaging changes in management. Amyloid PET results were positive in 55.3% of patients with MCI and 70.1% of patients with dementia. Changes between the pre-PET and post-PET composite management end point occurred in 60.2% of patients with MCI and 63.5% of patients with dementia.77 The second phase of the IDEAS study aims to assess whether amyloid PET is associated with improved clinical outcomes. These data, together with the results from other large projects that are still ongoing, for example, the Amyloid Imaging to Prevent Alzheimer Disease study in Europe,78 are likely to provide definitive quantified data concerning the impact on clinical outcomes and the cost-effectiveness of amyloid imaging.
DISCUSSION
The introduction of amyloid PET imaging enables in vivo detection of brain AβAβ deposition, one of the neuropathological hallmarks of AD. The cost-effectiveness of amyloid PET imaging and its impact on clinical outcomes is currently under investigation; therefore, its widespread diagnostic use is not yet justified or feasible. However, recent research has shown that amyloid PET imaging affects clinical management and reduces the number of further investigations, as well as improving diagnostic certainty in patients with progressive cognitive decline, in whom AD is possible but the diagnosis remains unclear despite otherwise comprehensive investigations. Although the current guidelines do not clearly describe a role for amyloid PET in investigating dementia,79 it should be noted that these were produced before a number of major studies that demonstrated its impact, including the ABIDE75 and IDEAS77 studies. Given the clear need for timely diagnosis in AD,59 80 it is evident that amyloid PET will be relevant to clinical practice in specific situations. Appropriate use criteria have been developed to guide the clinicians by predefining certain scenarios in which amyloid PET would be justified. These include (i)persistent or progressive unexplained MCI, (ii) atypical or mixed presentation, and/or (iii) early (<65 years of age) onset of dementia. When used in such atypical groups of patients, and in a multidisciplinary setting, amyloid PET has added value over the standardised diagnostic work-up.
In many centres, CSF analysis remains the first-line molecular Alzheimer’s biomarker of choice. Amyloid PET and CSF Aβ 1–42 show high concordance and similar diagnostic accuracy, suggesting that they may be used interchangeably.81–86 A systematic review and aggregate analysis of more than 1000 patients and controls who underwent both amyloid PET and CSF Aβ 1–42 testing showed that approximately 90% of subjects had concordant amyloid biomarker results. A few had discordant results, with either abnormal CSF Aβ 1–42 but negative amyloid PET (6.6%) or normal CSF Aβ 1–42 levels but positive amyloid PET scans (5.4%).87 The discordant cases may be partly due to technical or methodological or observational variations; however, there is evidence that isolated CSF Aβ positivity is dependent on disease stage, suggesting that CSF Aβ42 may be more sensitive in the early stages of AD, while PET amyloid may still change dynamically during the later stages of disease.88
The use of CSF biomarkers to identify AD is proven to be cost-effective, with lumbar puncture cost estimated at €150 and CSF Aβ42 testing at €35–60 in Europe.89 In comparison, the cost of amyloid PET scan is €2000–2500 (US$2300–2850) in Europe (UK National Health Service cost is £1300–1850) and US$3000–4500 in the USA.88
While increasingly acceptable to patients, CSF collection is still associated with significant morbidity and adverse effects. Furthermore, there is evidence that atypical AD syndromes may have less clear-cut CSF profiles than are normally observed in typical AD. Weston and colleagues36 showed that amyloid PET provides added diagnostic value over CSF, particularly in young-onset, atypical dementias. Moreover, CSF collection, storage and transport need to be carefully managed to maintain consistency.90 Establishing CSF cut-off points is also difficult with a wide variation in normal ranges between different centres.90 In general, as a non-invasive investigation, amyloid PET is very acceptable to patients with a rapid turnaround time for results. The authors of the ABIDE project found that more than 80% of patients experienced the PET scan as not burdensome.75 Furthermore, a recent report published by Alzheimer's Research UK on the public’s attitudes towards early detection and diagnosis of AD showed that at least 75% of people would be willing to undertake cognitive tests, brain imaging, blood tests or eye tests if these could help identify their risk of Alzheimer’s (even without disease-modifying treatments being available), while 40% would be willing to have CSF sampling.91
In the future, less invasive and less expensive blood-based biomarkers will probably be developed, enabling more widespread use. It is likely that such blood biomarkers will play an important screening role in primary care, identifying individuals who would benefit from more expensive and invasive testing with amyloid PET or CSF measurements.
However, current evidence suggests that, in a selected group of patients with cognitive impairment, amyloid imaging provides diagnostic clarity and significantly changes clinical management, while reducing the overall burden of investigations. We recommend a multidisciplinary team approach to ensure appropriate patient selection in line with current appropriate use criteria set out by the Amyloid Imaging Taskforce.
Key points
A decision to perform amyloid PET imaging should be made using a multidisciplinary team approach, integrating imaging with comprehensive clinical and cognitive evaluation, in order to maximise the likelihood that the imaging will contribute to the patient’s management.
A positive amyloid PET scan does not constitute, and is not equivalent to, a clinical diagnosis of Alzheimer’s disease.
Amyloid PET imaging should not be used in a typical presentation of Alzheimer’s disease when there is no comorbid confounding condition that could also affect cognition and function.
Further reading
Johnson KA, Minoshima S, Bohnen NI, et al. Appropriate use criteria for amyloid PET: a report of the Amyloid Imaging Task Force, the Society of Nuclear Medicine and Molecular Imaging, and the Alzheimer’s Association. Alzheimers Dement 2013;9(1):e-116.
de Wilde A, Ossenkoppele R, Pelkmans W, et al. Assessment of the appropriate use criteria for amyloid PET in an unselected memory clinic cohort: The ABIDE project. Alzheimer Dement 2019;15(11):145867.
Rabinovici GD, Gatsonis C, Apgar C, et al. Association of amyloid positron emission tomography with subsequent change in clinical management among medicare beneficiaries with mild cognitive impairment or dementia. JAMA 2019;321(13):128694.
REFERENCES
Footnotes
Twitter Paresh Malhotra @PareshMalhotra.
Contributors MAK wrote the first draft of the manuscript. All authors revised the original draft and contributed to the final submission.
Funding The authors receive research funding from the Alzheimer’s Society to examine the clinical use of amyloid PET imaging and are supported by the NIHR Biomedical Research Centre at Imperial College London.
Competing interests RP previously sat on an advisory board for Eli Lilly and received support from GE for research imaging from 2014 to 2018. ZW previously also participated in the Eli Lilly PET advisory board and was an amyloid PET read trainer. CC has taken part in an advisory panel for Roche pharmaceuticals. PM has given an educational talk at a meeting organised by GE. None of the authors currently has funding or support from any commercial organisation involved in amyloid PET imaging.
Patient consent for publication Not required.
Provenance and peer review Commissioned. Externally peer reviewed by Joshua Klein, Boston, USA.
Other content recommended for you
- Clinical utility of amyloid PET imaging with (18)F-florbetapir: a retrospective study of 100 patients
- Amyloid-PET burden and regional distribution in cerebral amyloid angiopathy: a systematic review and meta-analysis of biomarker performance
- Brain imaging in dementia
- Use of plasma biomarkers for AT(N) classification of neurodegenerative dementias
- Biomarkers in dementia: clinical utility and new directions
- Association of brain amyloidosis with the incidence and frequency of neuropsychiatric symptoms in ADNI: a multisite observational cohort study
- How many patients are eligible for disease-modifying treatment in Alzheimer’s disease? A French national observational study over 5 years
- Retinal imaging in Alzheimer’s disease
- CSF biomarkers for dementia
- Biomarkers for the diagnosis of Alzheimer’s disease, dementia Lewy body, frontotemporal dementia and vascular dementia