Article Text

Abstract
Rhomboencephalitis—inflammation of the brainstem and cerebellum—has myriad clinical presentations including encephalopathy, cranial neuropathies, long tract signs and cerebellar dysfunction and is associated with significant morbidity and mortality. There are a variety of potential underlying causes that respond variably to treatment, including infections, parainfective syndromes, inflammatory disorders including autoimmune encephalitis and paraneoplastic syndromes. Here, we review its clinical presentation and outline a practical approach to its investigation, aiming to facilitate prompt diagnosis and confirmation of the underlying cause, to start appropriate management early and optimise the clinical outcome.
- infectious diseases
- immunology
- neuroimmunology
- neuropathology
- virology
- neurovirology
Statistics from Altmetric.com
Introduction
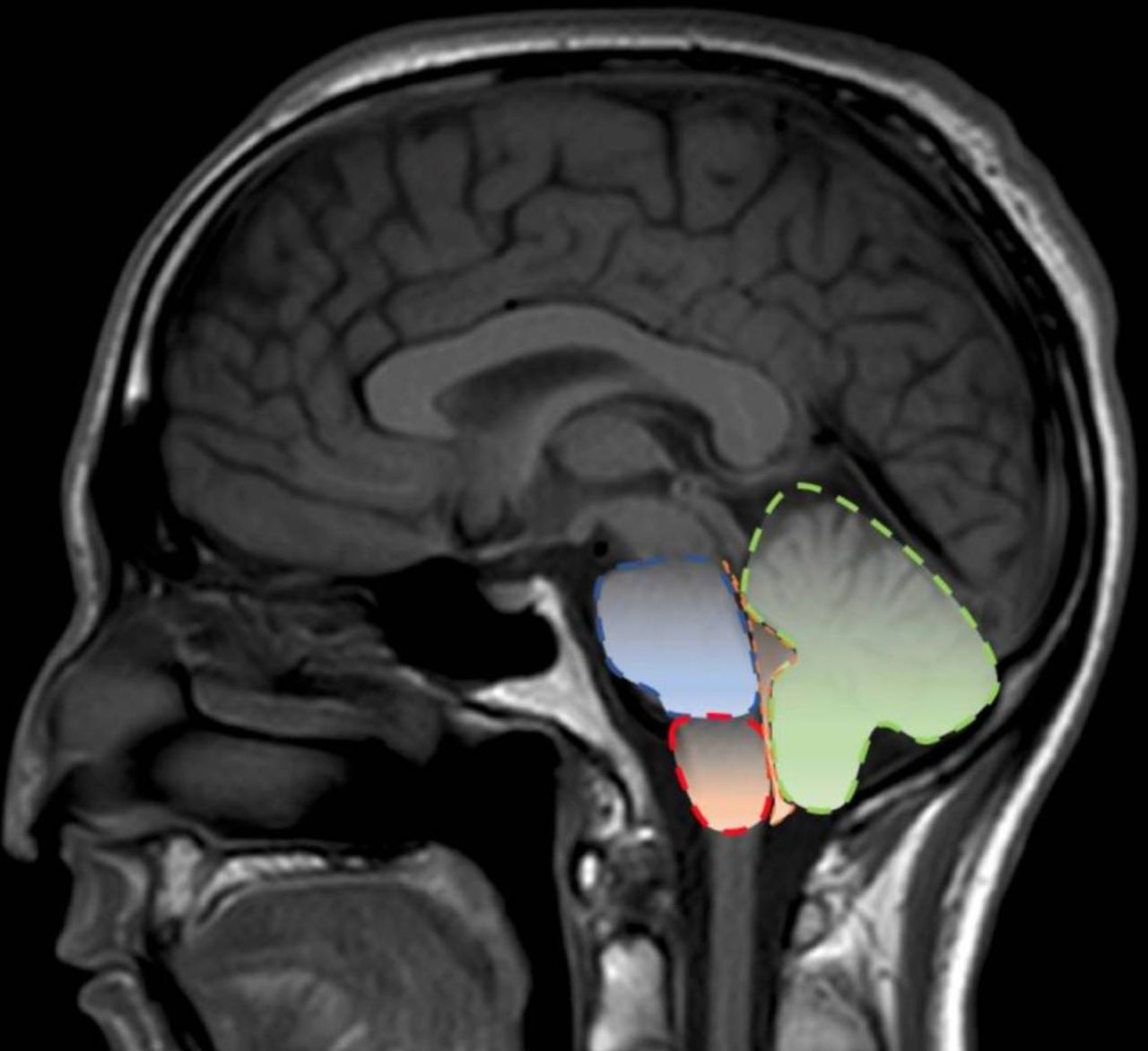
The name rhombencephalon derives from the Greek for ‘rhombus’, meaning diamond-shaped structure and ‘enkephalos’ referring to the brain. It comprises both the metencephalon and myelencephalon of the hindbrain. The metencephalon includes the cerebellum, the pons with its adjacent fourth ventricle and cranial nerves V–VIII. The myelencephalon contains the medulla oblongata with its fourth ventricle counterpart along with the bulbar cranial nerves and a portion of the vestibulocochlear nerve (figure 1).

MR scan of brain (sagittal) showing the anatomy of the rhombencephalon or hindbrain. Highlighted structures include the pons (blue), medulla (red), cerebellum (green) and the mid-region of the fourth ventricle (orange).
Despite the rhombencephalon technically excluding the midbrain, the term rhomboencephalitis (also known as rhomboencephalitis) is often used interchangeably with brainstem encephalitis. For practical purposes, we include brainstem encephalitis in our discussion of rhomboencephalitis.
Causes of rhomboencephalitis
We searched MEDLINE (1946–December 2019) and EMBASE (1974–December 2019), with no limits to language, and identified all the documented causative agents of rhomboencephalitis. We used the primary search terms ‘rhomboencephalitis’, ‘rhombencephalitis’ and ‘brainstem encephalitis’ including their synonyms, individually or in combination, to yield a search result of 1787 papers. We reviewed these and excluded paediatric cases. Table 1 summarises the reported causes of rhomboencephalitis and we discuss the more common presentations below.
Causes of brainstem encephalitis
Infections
Infectious rhomboencephalitides are typically bacterial or viral. They are more frequently reported in immunocompromised people and also occur in the immunocompetent.
Bacterial
Listeria rhomboencephalitis
The most common cause of rhomboencephalitis is infection with the Gram-positive bacterium Listeria monocytogenes. Public Health England recorded 135 cases of listeriosis in the UK in 2017. The bacterium is present in soil and vegetation and 1%–5% of the population are asymptomatic carriers. There have been outbreaks associated with contamination of unpasteurised cheeses or milks, cured meats, pâtés, smoked fish, cooked shellfish and, rarely, prepacked salads, particularly if mixed with meat. Brainstem infection probably results from retrograde axonal translocation via the cranial nerves innervating the oropharynx. It can also occur opportunistically in skull base erosion typically associated with cocaine abuse.1
Although listeriosis can affect the immunocompetent, it typically presents in the elderly, immunocompromised or pregnant population, manifesting as meningitis or meningoencephalitis. The risk appears to be particularly high with infliximab (antitumour necrosis factor-α); first year risk is estimated at 4.3–15.5 cases per 100 000.2 The source of infection may be from contaminated food consumption or chronic faecal carriage, although the predilection for the complication to occur early in treatment may favour re-emergence of latent disease. Patients on anti-tumour necrosis factor (TNF)-α blockers should be advised to take additional precautions with food hygiene for example, avoiding raw or undercooked eggs, pâté, meat and poultry as well as unpasteurised dairy products or soft and blue cheeses.
Rhomboencephalitis develops in about 9% of patients with central nervous system (CNS) listeria infections (figure 2) and can also occur in immunocompetent individuals. Of particular note for neurologists, cases have also been reported in association with disease modifying treatment for multiple sclerosis.3 4 Traditionally, it begins with a biphasic ‘flu-like’ illness followed, over a period of days, by the emergence of encephalopathy and brainstem signs. MR scan of brain may show multifocal abscesses, for example, T2-hyperintensities or ring-enhancing lesions on postcontrast T1-sequences in the thalamus, pons, medulla and cerebellar peduncles (figure 2).5 Diagnosis is confirmed by culture of the organism from blood or cerebrospinal fluid (CSF) although CSF PCR has greater sensitivity. There are limited data to support brain biopsy in cases of diagnostic uncertainty.
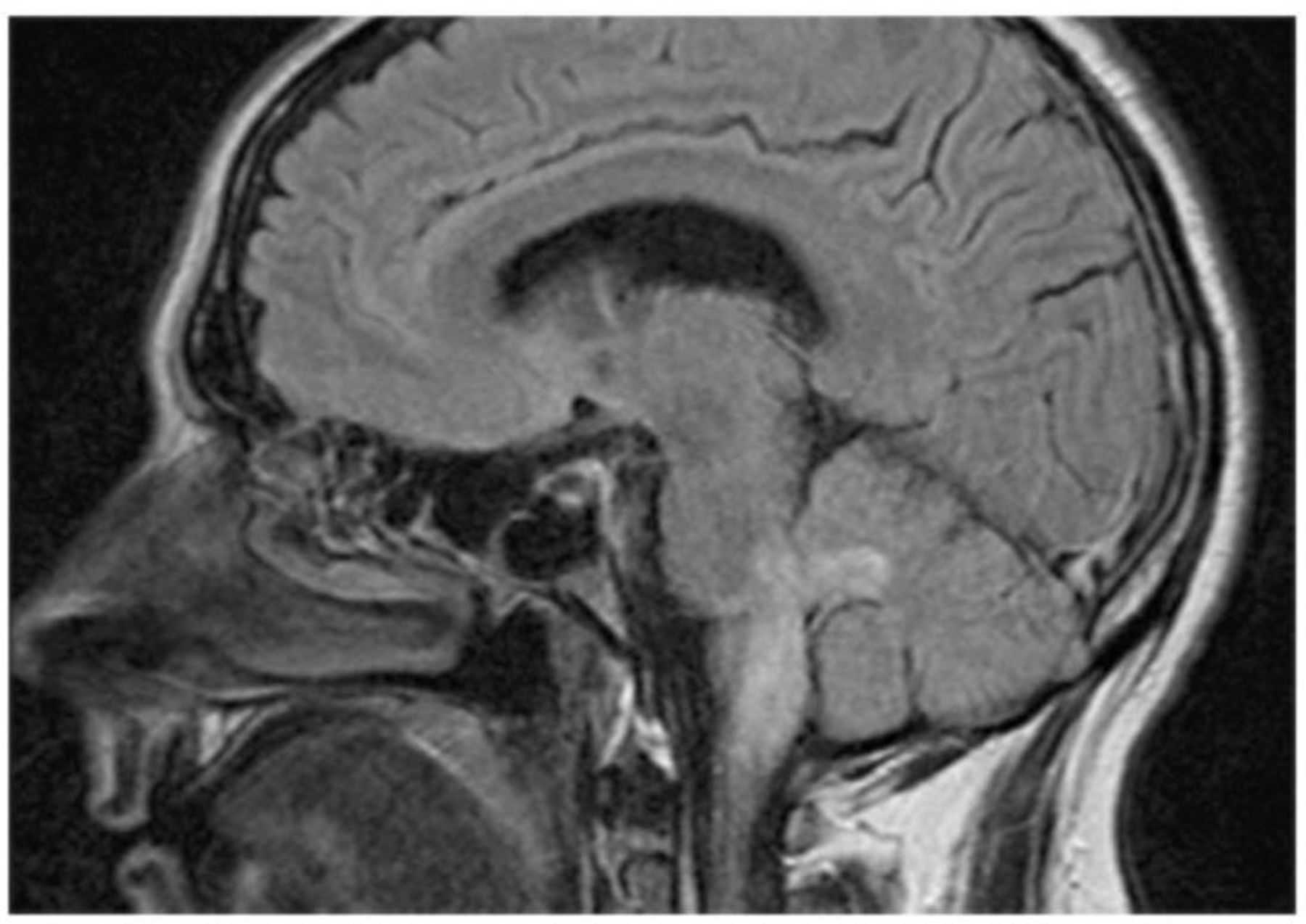
MR scan of brain (sagittal T1-weighted) with changes due to Listeria rhomboencephalitis, reproduced with permission from Abbs et al. Pract Neurol 2012;12:131–2.
The mortality rates highlight the importance of early recognition and starting appropriate treatment: 100% for untreated listeria rhomboencephalitis, falling to 76% with suboptimal antimicrobials and 40% with targeted therapy, for example, intravenous amoxicillin or ampicillin 2g every 4 hours±gentamicin or co-trimoxazole. Abscess formation may necessitate longer duration of treatment, and hydrocephalus (in 10%–15% of cases) or intraventricular haemorrhage (in 5%) may need neurosurgical intervention.6 Those responding poorly to standard therapy may need intraventricular antibiotics.6
Tuberculosis
About 10% people with tuberculosis have CNS involvement and 5% of these have brainstem disease. Caseating granulomata can mimic bacterial abscesses and tumour necrosis on neuroimaging, although core T2-hypointensity with vivid peripheral contrast enhancement on MRI representing gliosis and monocyte invasion are suggestive.7
The diagnosis of tuberculosis is confirmed by detecting acid-fast bacilli in, for example, respiratory samples, early morning urine or biopsy of tuberculoma. CSF culture and staining have sensitivities of below 20%, although this increases with repeated sampling. Larger CSF volumes may also increase the diagnostic yield. CSF adenosine deaminase, a marker of cell-mediated immunity, has a reported sensitivity of between 44% and 100%, and a specificity of between 71% and 100%.7 Given the significant morbidity and mortality, clinicians should start treatment for CNS involvement if the clinical findings and investigation results are consistent with the diagnosis, even if a rapid diagnostic test has returned negative results.8
The National Institute of Health and Care Excellence (NICE) for England and Wales recommends treatment for CNS tuberculosis to include rifampicin, isoniazid (with pyridoxine), pyrazinamide and ethambutol for 2 months, followed by 10 months of rifampicin and isoniazid (with pyridoxine).8 High-dose corticosteroids are recommended at the start of treatment, with subsequent taper over 4–8 weeks. Neurosurgical management is typically reserved for complications such as hydrocephalus, reducing mass effect due to tuberculomas and abscess drainage.
Neuroborreliosis
Lyme disease has protean CNS manifestations including lymphocytic meningitis, cranial neuropathies or a painful radiculitis 4–6 weeks after tick exposure. Clinicians need an index of clinical suspicion because only half of patients with neuroborreliosis report a rash consistent with erythema migrans and only one quarter recall a tick bite. Serology (both serum and CSF if suspecting rhomboencephalitis) is recommended, with input from a reference laboratory for extended immunoblotting if results are positive or equivocal. Interval serological testing for example, at 4 weeks can also help if tests are non-corroborative despite ongoing clinical suspicion. Virtually all cases have CSF lymphocytosis. Parenchymal brain changes are rare in neuroborreliosis but there are reports of pontine and cerebellar peduncle involvement. The treatment of Lyme disease that affects the CNS is with intravenous ceftriaxone 4g daily (in total) for 21 days, while looking out for a Jarisch-Herxheimer reaction, which can occur 1–12 hours after starting therapy.
Viral
Herpes simplex virus-1 and herpes simplex virus-2 (HSV-1 and HSV-2)
HSV encephalitis is the most common form of sporadic encephalitis. Neurological involvement typically causes temporal lobe, insular cortex, orbital frontal lobe and angular gyrus inflammation, while sparing of the basal ganglia and lobar white matter. More rarely, it can lead to rhomboencephalitis and, when this does occur, 80% are attributable to the HSV-1 subtype.9 Retrograde spread is thought to occur from the cisternal portion of the trigeminal ganglion into the brainstem and the radiological presentation may mimic an underlying neoplasm. Those with rhomboencephalitis may have isolated brainstem MRI changes although about 50% have concomitant supratentorial lesions,10 and the diagnosis is usually confirmed on CSF PCR. Treatment is with intravenous acyclovir (10 mg/kg three times per day) for a minimum of 2 weeks; current UK guidelines recommend repeat CSF analysis to confirm HSV PCR negative before stopping therapy.11
SARS-CoV-2
Coronavirus disease-2019 (COVID-19) is caused by the newly identified severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). SARS-CoV-2 is known to gain access to the CNS,12 and related viruses are thought to enter the brain via the olfactory bulb, with spread to the thalamus and brainstem. Indeed, brainstem involvement may contribute to respiratory failure in some patients with COVID-19.13 However, at the time of writing, only two cases of rhomboencephalitis have been described in association with COVID-19. One had MR brain scan findings consistent with rhomboencephalitis but normal CSF and improved rapidly with supportive therapy.14 The second was probably a postinfective syndrome, having presented with brainstem features including hyperekplexia, and normal MR scan of brain and CSF, and rapidly improved with corticosteroids.15
Other infectious causes
Multiple additional viral infections have been reported to cause rhomboencephalitis although these are more likely in children.
Enterovirus-71 (EV71) is the second most common infective cause of rhomboencephalitis overall, but predominantly affects those aged less than 5 years.16 Outbreaks have tended to occur in the Asia-Pacific region, with transmission via airborne droplets or the faeco-oral route. It may cause hand foot and mouth disease but, in severe cases, can cause an acute polio-like flaccid paralysis, aseptic meningoencephalitis and rhomboencephalitis. In adults, neurological complications are uncommon.
Other infectious causes include Japanese encephalitis, Epstein-Barr virus and cytomegalovirus. In the unvaccinated, Japanese encephalitis tends to affect young adults and children exposed to animals (including pigs) that carry the virus transmitted from the Culex mosquito around the Pacific rim, eastern and southern Asia. Patients with Japanese encephalitis may develop transient parkinsonian features with ‘dull, flat, mask-like facies with unblinking eyes’; tremor may develop and hypophonia may be marked. The MR scan of brain characteristically shows high T2 signal within the thalamus, brainstem and basal ganglia and so is distinct from the typical appearances of HSV encephalitis.17
Epstein-Barr virus encephalitis predominantly affects children, although there are well-recognised cases in adults.18 It may affect the temporal lobes, masquerading as HSV encephalitis, and can also damage the diencephalon or, less frequently, cause rhomboencephalitis. Features suggesting this infection include cervical lymphadenopathy, hepatosplenomegaly and transaminitis.
Cytomegalovirus encephalitis should be suspected in immunodeficient patients who have an Epstein-Barr virus-like constellation of symptoms, transaminitis, diarrhoea, retinitis, pneumonia or painful ulcers in the oesophagus or intestine. It can lead to direct damage of the brainstem through cytomegalovirus inclusions and microglial nodules.19 Importantly, both Epstein-Barr virus and cytomegalovirus can lead to perivascular lymphocytic infiltration with oedema and glial nodules due to Bickerstaff’s brainstem encephalitis.
Parainfectious
Bickerstaff’s brainstem encephalitis
Bickerstaff’s brainstem encephalitis is typically a monophasic, postinfective syndrome involving a triad of ophthalmoplegia, ataxia and depressed level of consciousness. Electroencephalogram abnormalities are common and, although MR scan of brain is usually normal, it can show scattered T2 hyperintensities in the brainstem and basal ganglia with limited enhancement and mild diffusion restriction.20 In contrast to Miller Fisher syndrome and Guillain-Barré syndrome, Bickerstaff’s brainstem encephalitis is associated with hyperreflexia. However, about two-thirds of patients with Bickerstaff’s brainstem encephalitis have peripheral motor axonal neuropathy and detectable anti-GQ1b antibodies. Intravenous immunoglobulin and/or plasma exchange may be considered in an attempt to expedite recovery although, overall, the prognosis is relatively favourable; a retrospective analysis of 62 cases reported 66% complete remission at 6 months.21
Acute disseminated encephalomyelitis
Acute disseminated encephalomyelitis (ADEM) is a rare inflammatory disorder of the CNS causing destruction of myelin and cerebral white matter. Although more common in children, it is well recognised in adults. Patients may present 1–3 weeks after a viral prodromal illness or vaccination and symptoms can include a combination of fever, ataxia, confusion, seizures and/or coma. Characteristically, ADEM is monophasic, progressing over days before reaching a plateau; a minority may relapse and there is a rare, fulminant form, known as acute haemorrhagic leucoencephalitis (figure 3).22

Acute haemorrhagic leucoencephalitis MR scan of brain (sagittal T2-weighted) showing extensive brainstem involvement with hyperintense T2 signal, reproduced with permission from Nabi et al, BMJ Case Reports 2016;2016:bcr2016217215.
The pathophysiology of ADEM is not fully understood but cell-mediated or antibody cross-reaction with myelin autoantigens probably develops in response to an environmental trigger or increased CNS vascular permeability due to inflammation postvaccination or infection. Putative causative organisms include several viruses directly linked to rhomboencephalitis such as Epstein-Barr virus, cytomegalovirus, HSV, human herpes virus 6.
Typical MR brain scan findings in ADEM include fleeting multifocal asymmetrical white matter T2 and fluid-attenuated inversion recovery (FLAIR) hyperintensities with ‘open-ring’ contrast enhancement but no central restriction on diffusion-weighted imaging.23 This has a ‘grass-fire appearance’ with relatively less mass effect than might be expected given the lesion size. Involvement of the thalami, brainstem (figure 3) and cerebral cortex may help to distinguish it radiologically from multiple sclerosis.23 Initial treatment for ADEM is with intravenous methylprednisolone 1 g over 3–5 days followed by plasma exchange or intravenous immunoglobulin (0.4 g/kg/day for 5 days) in steroid-refractory cases. Cyclophosphamide can also be considered in fulminant ADEM. Oral corticosteroids should be tapered over 6 weeks and vaccinations avoided for 6 months following treatment. Decompressive hemicraniectomy may be life-saving when cerebral oedema is refractory to medical treatment.24
Paraneoplastic syndromes
Paraneoplastic antibodies have been well documented to cause rhomboencephalitis and discovery of new cell surface autoantibodies and characterisation of their respective clinical phenotypes is a rapidly expanding field. Table 2 lists paraneoplastic antibodies reported to be associated with rhomboencephalitis, tumour associations and treatment options, although the responsible antibody may not always be identified (figure 4).
Paraneoplastic antibodies associated with rhomboencephalitis
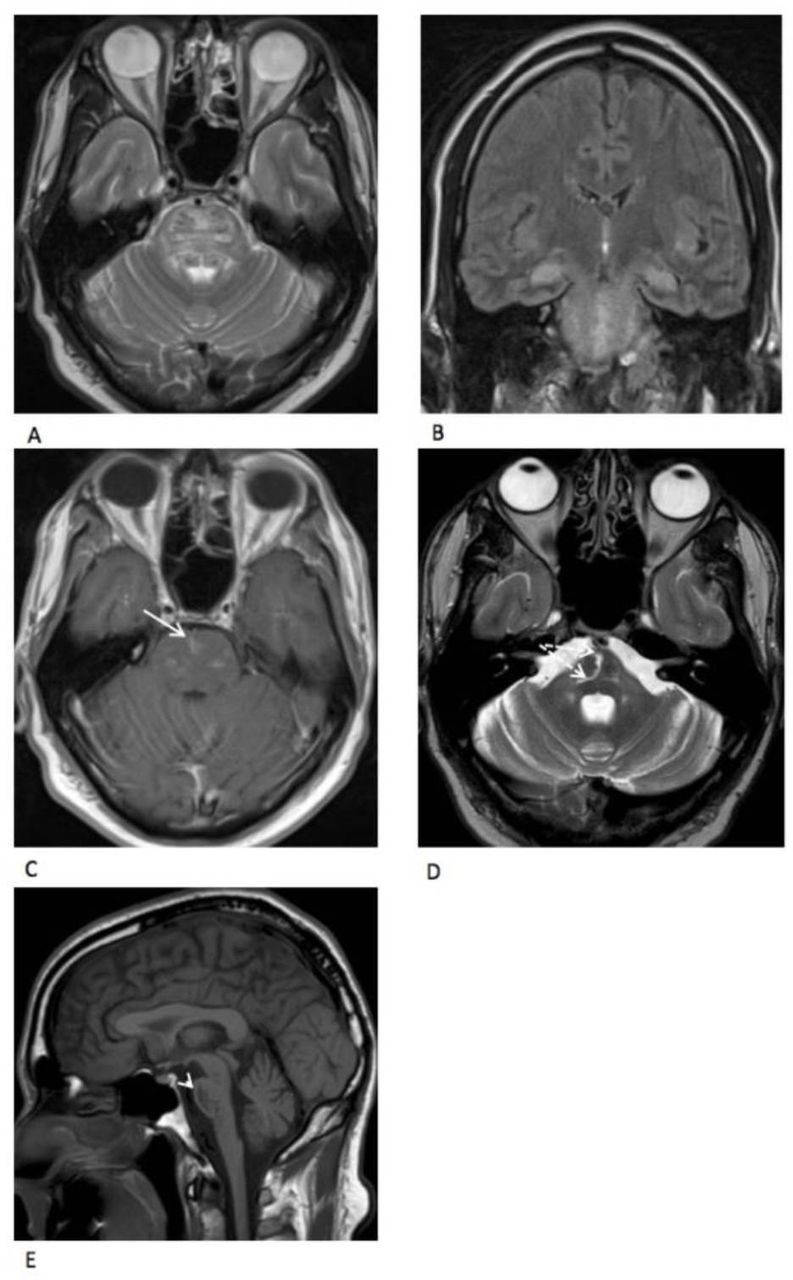
Seronegative autoimmune encephalitis. (A,B) MR scan of brain (axial T2 and coronal FLAIR) showing abnormal hyperintense signal in the pons, midbrain and also bilaterally within the hippocampi. (C) MRI axial postgadolinium T1 showing patchy pontine enhancement (white arrow). (D,E) MRI follow-up axial T2 and sagittal T1 performed 22 months after first presentation showing marked pontine atrophy (arrowhead) with bilaterally symmetrical linear hyperintensity within the pontocerebellar fibres (dotted arrows). FLAIR, fluid-attenuated inversion recovery.
Cell surface antibodies
Anti-NMDA receptor encephalitis
Anti-N-methyl-D-aspartate receptor (NMDAR) encephalitis is the most common autoimmune cell surface-mediated encephalitis. It is characterised by a combination of dysautonomia, seizures, movement disorders and psychiatric symptoms. It is often associated with malignancy, particularly ovarian teratomas, but has also been described following HSV and varicella zoster virus encephalitis.25 26
Anti-NMDAR encephalitis has been associated rarely with rhomboencephalitis in adults although this appears more common in children. Despite the marked clinical features, MR scan of brain can frequently be normal and is recognised as a clinical-radiological paradox. However, there are cases with T2 hyperintensities in the brainstem, mesial temporal lobes and posterior periventricular white matter with cranial nerve enhancement.27 Paired serum and CSF antibody testing is recommended.
First-line treatment for NMDAR encephalitis is high-dose corticosteroids followed by intravenous immunoglobulin or plasma exchange and escalation to cyclophosphamide or rituximab and/or introduction of a steroid-sparing agent as required. There may be clinical uncertainty while awaiting antibody test results but there is emerging evidence to support use of intravenous immunoglobulin in some forms of encephalitis. Indeed, there may be a role for prophylactic immunosuppression in patients with HSV encephalitis to prevent development of secondary NMDAR antibodies,26 and a UK-based, double-blinded randomised trial is currently underway to determine whether intravenous immunoglobulin improves outcomes in children with infective or immune-mediated encephalitis (IgNiTE; ISRCTN15791925).
Immunoglobulin-like cell adhesion molecule 5 (IgLON5) receptor encephalitis
IgLON5 receptor is a neuronal cell adhesion protein of uncertain physiological function. Antibodies against IgLON5 trigger deposition of tau in the hypothalamus and tegmentum and are associated with HLA-DRB1*1001 and HLA-DQB1*0501. IgLON5 receptor encephalitis was first described in 2014 as a disorder of sleep, brainstem and hypothalamic function, movement (particularly chorea), cognition and a progressive supranuclear palsy-like syndrome. Typically, brainstem involvement causes bulbar dysfunction manifesting as dysphagia, sialorrhoea, stridor or acute respiratory insufficiency. A retrospective analysis of 22 patients with anti-IgLON5 antibodies reported 82% had normal/non-specific MR brain scan changes with mild brainstem atrophy in 14% and hippocampal atrophy in 4.5%.28 CSF was unremarkable with 50% showing only a mildly raised protein. Outcome was poor; 59% died of respiratory complications.
Anti-IgLON5 disease should be considered in rhomboencephalitis presenting on the background of sleep disorder, chorea, bulbar dysfunction or central hypoventilation. Early treatment with immunotherapy may prevent life-threatening acute respiratory failure and/or avoid further unnecessary investigations.29
Progressive encephalomyelitis with rigidity and myoclonus
Progressive encephalomyelitis with rigidity and myoclonus (PERM) is characterised by painful spasms, autonomic dysfunction, hyperekplexia, brainstem myoclonus and breathing problems;30 it has been labelled ‘stiff-person syndrome-plus’, given the additional brainstem abnormalities. It has only recently been associated with antiglycine receptor (anti-GlyR) antibodies and the clinical phenotype in the largest retrospective cohort of 52 patients included hyperekplexia, stiffness/spasms/rigidity, oculomotor disturbance and facial/bulbar motor involvement. This was followed by seizures, encephalopathy and cognitive defects. Respiratory failure occurred in 27%.30 MR brain scan findings were relatively non-specific although a minority had bilateral temporal lobe hyperintensities. Electromyography may show continuous motor activity and 6/29 had spontaneous or stimulus-induced activity. CSF pleocytosis is typical and there may be unmatched oligoclonal bands.
Anti-GlyR antibodies should be requested in the serum and CSF in patients with suspected stiff-person syndrome and evidence of brainstem dysfunction. CSF antibody testing can help when serum anti-GlyR antibodies are low (<1:20 dilution) and discussion with specialist neuroimmunology laboratories is good practice. PERM has been associated infrequently with other antibodies including anti-dipeptidyl-peptidase-like protein 6, antiamphiphysin and anti-GAD65 (glutamic acid decarboxylase-65) antibodies.31
Intracellular antibodies
Anti-Hu (antineuronal nuclear antibodies-1) antibody is most commonly associated with small cell carcinoma, which targets the cell nucleus. In 15% of patients, it occurs secondary to an extrathoracic malignancy. In the context of rhomboencephalitis, it preferentially affects the medulla, causing dysphagia, dysarthria and central hypoventilation. In contrast, anti-Ma2 paraneoplastic syndrome typically affects the mesencephalon causing a vertical gaze palsy and being associated with T2-hyperintensities in the superior colliculi or periaqueductal grey region.32 These features, particularly if accompanied by malignancy or risk factors including smoking, should raise the possibility of a paraneoplastic syndrome rhomboencephalitis. Importantly, the paraneoplastic syndrome commonly precedes other clinical manifestations of malignancy, and patients in whom a cancer is not initially detected need ongoing screening for a minimum of 5 years.
CSF examination in patients with paraneoplastic syndrome may identify a mild pleocytosis, but extended immunoblotting screens are usually required to search for all additional or atypical antineuronal antibodies in both serum and CSF. Of the three most common neuronal antibodies linked to rhomboencephalitis (anti-Hu, anti-Ri and anti-Ma2), anti-Ma2 has the most favourable prognosis following combination immunotherapy and tumour removal but prognosis is generally poor.
Neuroinflammatory causes
Neuro-Behçet’s syndrome
Although there are diagnostic criteria available, the diagnosis of Behçet’s disease can be challenging (table 3). Clinicians need to question carefully for recurrent orogenital ulceration and symptoms of iritis or erythema nodosum. Pathergy testing and HLA-B51 allele screening may be required. Retinal angiography is also recommended to look for retinal vasculopathy, which is easily overlooked on routine ophthalmological examination.
International Study Group for Behçet’s Disease Classification criteria
Manifestations of neuro-Behçet’s can be divided into a CNS inflammatory parenchymal disease with predilection for the corticospinal, spinothalamic and posterior column tracts and a non-parenchymal vascular form, which typically presents as dural venous sinus thrombosis.
Radiologically, neuro-Behçet’s favours the brainstem—although may sometimes affect the diencephalon—but the mechanism behind this predilection is unclear.33 Acutely, T2-weighted and FLAIR-weighted hyperintensities with corresponding hypo-/isointensities on T1 sequences predominate with patchy T1-gadolinium enhancement (figure 5). There may be a longitudinal myelitis-like, inflammatory lesion extending to the brainstem giving a distinct appearance known as the ‘bagel sign’ due to venous engorgement and/or acute blood products. Occasionally, brainstem and subcortical lesions may mimic multiple sclerosis.33

Parenchymal brainstem neuro-Behçet’s syndrome MR scan of brain showing pontine lesions extending to bilateral middle cerebellar peduncles, which are hypointense on T1-weighted imaging (A), hyperintense on T2-weighted imaging (B), with heterogeneous contrast enhancement (C), reproduced with permission from Yildiz et al, BMJ Case Reports 2013;2013:bcr2013200738.
Systemic lupus erythematosus
Systemic lupus erythematosus (SLE) is a multisystem autoimmune disorder. ‘Neurolupus’ has protean clinical manifestations including seizures, myelopathy, strokes, aseptic meningitis, psychosis and unexpected movement disorders including myoclonus and parkinsonism.34 A prospective study of seven patients with SLE-induced rhomboencephalitis reported headache, vertigo and reduced level of consciousness as the most common clinical features.35 Microvasculopathy leads to ischaemia, antibody-mediated cell injury and cytokine-induced blood brain barrier permeability allowing leucocyte translocation and inflammation.
Radiologically, CNS lupus typically causes subcortical and periventricular white matter changes on MRI with diffuse T2 and FLAIR hyperintensities within the deep white matter, brainstem and cerebellum.35 Brainstem involvement is rare in SLE, although concomitant periventricular lesions necessitate consideration of the diagnosis.
Other demyelinating conditions
Several demyelinating conditions may be associated with inflammatory brainstem lesions such as ADEM (discussed previously), multiple sclerosis and neuromyelitis optica spectrum disorder, including antimyelin oligodendrocyte (MOG) and antiaquaporin-4 antibodies.
An area postrema syndrome may occur with clinical features such as intractable hiccups, nausea and vomiting, which may appear in isolation or together with optic neuritis and myelitis to suggest neuromyelitis optica. This condition typically favours the dorsal region of the medulla and pons surrounding the fourth ventricle. Additional clues suggesting anti-MOG disease include an ADEM-like presentation, bilateral optic nerve involvement, cortical encephalitis and/or the presence of ‘fluffy’ brainstem appearances (30%).36 Serological testing confirms the diagnosis with no current evidence for improved sensitivity with CSF testing suggesting predominantly extrathecal production.
Mimics
It is important for clinicians to be aware of the radiological mimics of rhomboencephalitis (box 1 and figure 6). The most common differential diagnosis is a primary intracerebral malignancy, particularly glioma. Additional investigations may therefore include CSF cytology and flow cytometry (assuming safe to proceed with lumbar puncture) and MR spectroscopy, which may show raised choline/NAA (n-acetylaspartate) ratio suggesting malignancy.
Rhomboencephalitis mimics
Intra-axial neoplasms—primary intracerebral malignancy, CNS lymphomas, metastases.
Tumefactive demyelination.
Vascular: brainstem stroke, vasculopathies and advanced small vessel ischaemic changes.
Central pontine myelinolysis or osmotic demyelination syndrome.
Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS).
Syringobulbia.
Histiocytosis.
Toxins—heroin-induced leukoencephalopathy, cocaine abuse, methylbromide, carbon monoxide poisoning or hyperammonaemia.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Rhomboencephalitis mimics. (A) Lymphoma: coronal FLAIR MRI—abnormal signal hyperintensity within the vermis and left paramedian vermis with minimal local mass effect. The lesion shows abnormal restricted diffusion and homogenous enhancement (not shown) as expected in primary CNS lymphoma. (B) Astrocytoma: coronal T1 postcontrast MRI—irregular peripherally enhancing and centrally necrotic lesion in the lower pons/upper medulla. Mild local mass effect with expansion of the involved structures. (C,D) Osmotic demyelination syndrome: (C) axial non-contrast CT Head—spherical hypodensity involving the central pons which is mildly expanded. (D) Axial T2—well-demarcated central pontine T2 hyperintensity with sparing of the periphery and the descending corticospinal tracts (white arrows) (E,F) CLIPPERS: (E) Axial T2 MRI—florid patchy and linear punctate hyperintensities within the brainstem and bilaterally in the cerebellum with no associated oedema or local mass effect (white arrows). (F) Sagittal T1 postcontrast MRI brain and upper cord—numerous enhancing punctate foci in the brainstem, cerebellum and the upper cervical spinal cord. FLAIR, fluid-attenuated inversion recovery.
Clinical approach
History
Key points to explore when taking a history of rhomboencephalitis include:
A febrile illness suggesting an infective cause (see table 4).
Recreational drug use, particularly cocaine, which can erode the surrounding skull base and sinuses creating a pathway from the nasal cavity to the brainstem.
Smoking history to assess the risk of paraneoplastic syndromes.
‘B’ symptoms (fever, weight loss and night sweats), which could indicate an underlying lymphoma or tuberculosis.
A gynaecological history including postmenopausal bleeding/discharge, menstrual cycle changes, pelvic pain or bloating, which may be associated with an underlying malignancy.
Outcomes of breast examinations/screening in females.
Testicular self-examination findings and investigations in males.
Sleep disorders such as obstructive sleep apnoea or parasomnias, which may suggest anti-IgLON5 disease.
Connective tissue disease symptoms should be probed including mouth/genital ulcers, rash, arthralgia/myalgias xerostomia/xerophthalmia, symptoms of iritis or serositis, Raynaud’s phenomenon and photosensitivity.
Discrete neurological relapses including features of myelitis or optic neuritis may suggest multiple sclerosis or neuromyelitis optica spectrum disorder.
Practical approach to history taking in infective rhomboencephalitis
Examination
Patients need a complete systemic and neurological examination, with particular attention to:
Fever and lymphadenopathy, which may suggest infective causes such as Epstein-Barr virus/cytomegalovirus or an underlying malignancy/paraneoplastic syndrome.
Mouth/genital ulcers, which could suggest HSV, Behçet’s syndrome or SLE.
Inspection of the nasal passage, which may identify erosions suggesting portal of entry for infection.
Autonomic dysfunction (systolic blood pressure drop ≥20 mm Hg on standing, resting tachycardia, constipation and/or urinary retention), which may suggest a cell surface-mediated paraneoplastic syndrome.
Movement disorders including orofacial dyskinesias, dystonias, chorea and stereotypies, which could suggest anti-NMDA receptor encephalitis or Japanese encephalitis.
Breast examination in females and testicular examinations in females and males are needed to look for underlying malignancies.
Vertical gaze palsy may be associated with anti-Ma2 antibodies but, when combined with features of parkinsonism, could suggest anti-IgLON5 disease.
Hyperekplexia in response to auditory or tactile stimulation with rigidity (predominantly axial), which may be a feature of progressive encephalomyelitis with rigidity and myoclonus.
Skin changes such as erythema nodosum, butterfly/discoid rash or pseudofolliculitis, which suggest autoimmune causes.
Investigation and management
Management of rhomboencephalitis is tailored to the cause. However, it may be pragmatic to consider broad spectrum antimicrobials, including cover for viral and listeria, in all cases presenting acutely or subacutely with rhomboencephalitis pending initial investigation results. Box 2 illustrates a framework to guide appropriately tailored investigations.
Investigations to consider in rhomboencephalitis
Infective
Blood
Blood serology and/or PCR (see table 1).
Blood cultures (bacterial infections including listeria).
Cerebrospinal fluid (CSF)
Microscopy, culture and sensitivity for listeria, tuberculosis and others (see table 1).
Standard viral PCR and Epstein-Barr virus/cytomegalovirus/HHV-6/tuberculosis PCR if immunocompromised or on clinical suspicion.
Consider Whipple’s disease PCR.
Consider bacterial 16S rDNA real-time PCR for a broad bacterial screen.
Other
Stool cultures/rectal swabs (enterovirus-71).
Nasal/throat swabs (viruses including SARS-CoV-2, enterovirus and influenza).
Sputum sample or early morning urine for tuberculosis microscopy, culture and sensitivity.
If recent exotic foreign travel or atypical presentation discuss with infectious disease team or microbiology.
Paraneoplastic
Intracellular antibodies
Anti-Hu, anti-Ri, anti-Ma2, anti-Yo anti-Tr, antiamphiphysin and anti-GAD65.
Cell surface antibody
Anti-NMDA, anti-IgLON5, antiglycine and anti-DPPX.
Searching for the underlying malignancy
Lactate dehydrogenase and blood film.
Serum α-fetoprotein or β-human chorionic gonadotropin.
CSF cytology and flow cytometry (ideally obtain 10 mL mL).
Imaging as appropriate including: ultrasound scan of ovaries/testes, MR scan of pelvis, chest X-ray, mammogram, CT scan of chest/abdomen/pelvis or CT-PET scan.
Rheumatological
Autoimmune profile
Antinuclear antibody, complements, anti-double-stranded DNA, extractable nuclear antigen, lupus anticoagulant (not if on anticoagulation), anti-cardiolipin and anti-beta2-glycoprotein-1.
Sarcoidosis
Serum/CSF angiotensin converting enzymeACE, CSF soluble interleukin-2 and chest imaging.
Neuro-Behçet’s syndrome
HLA-B51, retinal fluorescein angiography/indocyanine green angiography, skin biopsy and pathergy test.
Sjögren’s syndrome
Schirmer’s test, salivary gland/mucosal lip biopsy or technetium-99m scialoscintigraphy.
Parainfectious
Acute disseminated encephalomyelitis
Anti-MOG antibodies.
Bickerstaff’s brainstem encephalitis
Ganglioside antibodies including anti-GQ1b.
If ongoing diagnostic uncertainty, consider brain biopsy.
DPPX, dipeptidyl-peptidase-like protein 6; GAD, glutamic acid decarboxylase; HHV-6, human herpes virus 6; IgLON5, immunoglobulin-like cell adhesion molecule 5; NMDA, N-methyl-D-aspartate; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
Biopsy and other neurosurgical interventions
Brain biopsy, particularly in the brainstem, is considered a high-risk procedure. However, emerging data suggest that safety has improved and brainstem biopsy can be clinically very helpful in selected cases, particularly where malignancy is a possibility or where there is ongoing diagnostic uncertainty.37 38 The risk of the procedure needs to be weighed against the benefit of diagnostic clarity, treatment optimisation and avoidance of iatrogenic harm for example, from unnecessary immunosuppression. Where there is diagnostic uncertainty in a rapidly deteriorating patient, we recommend early discussion with neurosurgical colleagues to consider a biopsy, particularly where a target lesion is identified.39
Urgent repeat neuroimaging is indicated if a patient with a known brainstem syndrome develops new signs or reduced level of consciousness. Complications including hydrocephalus or haemorrhage may warrant neurosurgical management.6 This is particularly relevant where the underlying cause of rhomboencephalitis is infective, most especially listeria and tuberculosis.
Conclusion
Rhomboencephalitis is an uncommon neurological condition with potentially devastating sequelae, particularly if left untreated. Clinicians therefore need a structured and pragmatic approach. A careful and complete assessment of the history together with systemic and neurological examination are crucial to guide prompt and appropriate investigations and treatment as well as where appropriate, early involvement of neurosurgical colleagues.
Key points
Rhomboencephalitis typically presents with encephalopathy with or without long tract signs, cranial nerve deficits and/or cerebellar dysfunction.
Suspected infection should prompt enquiry about snorting cocaine, which can create an artificial portal of entry.
The most common cause is listeria and clinicians should consider early, empirical treatment.
Specialist review of MR brain scans can refine the differential diagnosis.
Some patients require neurosurgical intervention including diagnostic biopsy, and emergency treatment of hydrocephalus may be required.
Further reading
Jubelt B, Mihai C, Li TM, et al. Rhomboencephalitis/brainstem encephalitis. Curr Neurol Neurosci Rep 2011;11:543–52. doi: 10.1007/s11910-011-0228-5.
Kickingereder P, Willeit P, Simon T, et al. Diagnostic value and safety of stereotactic biopsy for brainstem tumours: a systematic review and meta-analysis of 1480 cases. Neurosurgery 2013;72:873–81. doi: 10.1227/NEU.0b013e31828bf445.
References
Footnotes
Contributors The manuscript was designed by JC and CMR. All authors contributed to drafting and revision of the manuscript for intellectual content.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Commissioned. Externally peer reviewed by Emma Tallantyre, Cardiff, UK.
Linked Articles
- Editors’ commentary
Other content recommended for you
- Infectious encephalitis: mimics and chameleons
- Bickerstaff’s brainstem encephalitis associated with anti-GM1 and anti-GD1a antibodies
- Bickerstaff’s brainstem encephalitis mimicking herpetic encephalomyelitis in a liver transplant patient with anti-GQ1b antibodies
- Nationwide survey of patients in Japan with Bickerstaff brainstem encephalitis: epidemiological and clinical characteristics
- Cortical abnormalities on MRI: what a neurologist should know
- Bickerstaff’s brainstem encephalitis related to Campylobacter jejuni gastroenteritis
- Chronic lymphocytic inflammation with pontine perivascular enhancement responsive to steroids (CLIPPERS) in limited cutaneous sclerosis: a rare disease combination
- An MRI review of acquired corpus callosum lesions
- Neuromyelitis optica presenting as acute bilateral ptosis
- Multicentre comparison of a diagnostic assay: aquaporin-4 antibodies in neuromyelitis optica