Article Text

Abstract
A 48-year-old man with severe Guillain-Barré syndrome suffered complete paralysis, and for 31 days could not communicate with the outside world, while remaining fully conscious. After recovery, he provided feedback on aspects of his care, such as mechanical ventilation, physical therapy, and communication. Conventional low tidal volume normocapnic ventilation induced ongoing and profound dyspnoea, occasionally relieved by modest increases in minute ventilation. Routine and apparently benign physical therapy was extremely painful, which was not reflected in heart rate or blood pressure changes. When he eventually re-established communication after many weeks, via slight eye movements, his first message was to express a particular distressing symptom. His case is a valuable reminder of the sometimes large gap between clinical measurements and assumptions and the subjective patient experience. We propose several approaches to address such issues in other paralysed but conscious patients.
- Guillain-Barre syndrome
- neuropathy
- intensive care
Statistics from Altmetric.com
Background
Ventilated patients in intensive care units are usually unconscious. However, for conscious patients, many factors besides partial pressure of carbon dioxide (PCO2) can induce the sensation of breathlessness. This can be particularly important for those who cannot communicate their distress due to advanced neuromuscular disease.
We report the experiences of a 48-year-old professional man with severe Guillain-Barré syndrome who was ventilated in an intensive care unit for 170 days. He was totally paralysed and completely unable to communicate for 31 days, despite being fully conscious. During this time, he received methadone, oxycodone and gabapentin for pain relief, but was not sedated. This protocol had been established in the weeks before, while he could still communicate through slight movement of his left eye. He eventually recovered and left hospital on day 190. We interviewed him 6 weeks later.
Breathlessness
During his weeks of being ‘locked-in’, he had an ongoing and intensely distressing sense of breathlessness, present ‘most of the time’, made worse by reductions in tidal volume or ventilatory rate.
It was like being buried at the beach with only a straw protruding for breathing.
I was … chasing those breaths all the time … and trying to count my way through it … just constantly trying to calm myself down.
The mean tidal volume over that period was 7 mL/kg, but this varied with the different daily treating teams. From carefully listening to conversations around him, he concluded that tidal volumes of 800–850 mL (~9 mL/kg) were comfortable and did not induce dyspnoea. He learnt to recognise individual staff members by voice, and even by footsteps, and knew who was likely to adjust the ventilation either up or down.
Sometimes I would lie there thinking: ‘just keep walking, just keep walking’.
Then I could feel it start to happen … I could feel my blood pressure go up … I could hardly hear anything … it was just thumping in my head … I couldn’t hear people talking … it was deafening.
Only one nurse routinely responded to the autonomic signs by increasing the ventilatory rate, which greatly improved his symptoms.
As soon as the ventilator was put up, usually two breaths, it would stop virtually straight away.
Unfortunately, this intervention—so important to him—did not become an established part of the protocol for the core treatment team and he could not communicate this until after his recovery. Instead, the ventilator settings were frequently adjusted to achieve ‘normocapnia’.
As he slowly regained muscle function, the treating teams instigated ‘spontaneous breathing trials’ to evaluate recovery. He found these very taxing due to their induced sense of suffocation and panic. He strongly felt that teams should not instigate such an approach to ventilator weaning in a conscious patient, unless there was established reliable communication.
Physical therapy
Some of the physical therapy sessions were clearly beneficial.
When my chest was getting blocked up, I would feel progressively anxious. After a physiotherapy session, I always felt better, and calmer.
Others, however, provoked intense pain—in particular, the passive stretching of calf and masseter muscles.
It felt like they were trying to tear the muscles off the bone … I’ve never known pain like it. It was that painful I could see light white fuzz, then the pain went even more … and you just basically pass out.
During this therapy, staff would sometimes refer to heart rate and blood pressure as indicators of pain; however, at the time, he was receiving beta blockers for autonomic dysregulation, rendering these signs unreliable. The patient himself realised this reasoning was spurious, compounding feelings of frustration with the treating team.
Disorientation
Although his vision was preserved, he could not open his eyes and so could not orientate himself to the world around him.
I felt totally disconnected from everything, like I was living in a shell. But as soon as my eyes were open, I could reconnect with the world. It made all the difference.
When they rolled me, it consistently felt like I was going through the bed and then the next minute I settled upside down.
Communication
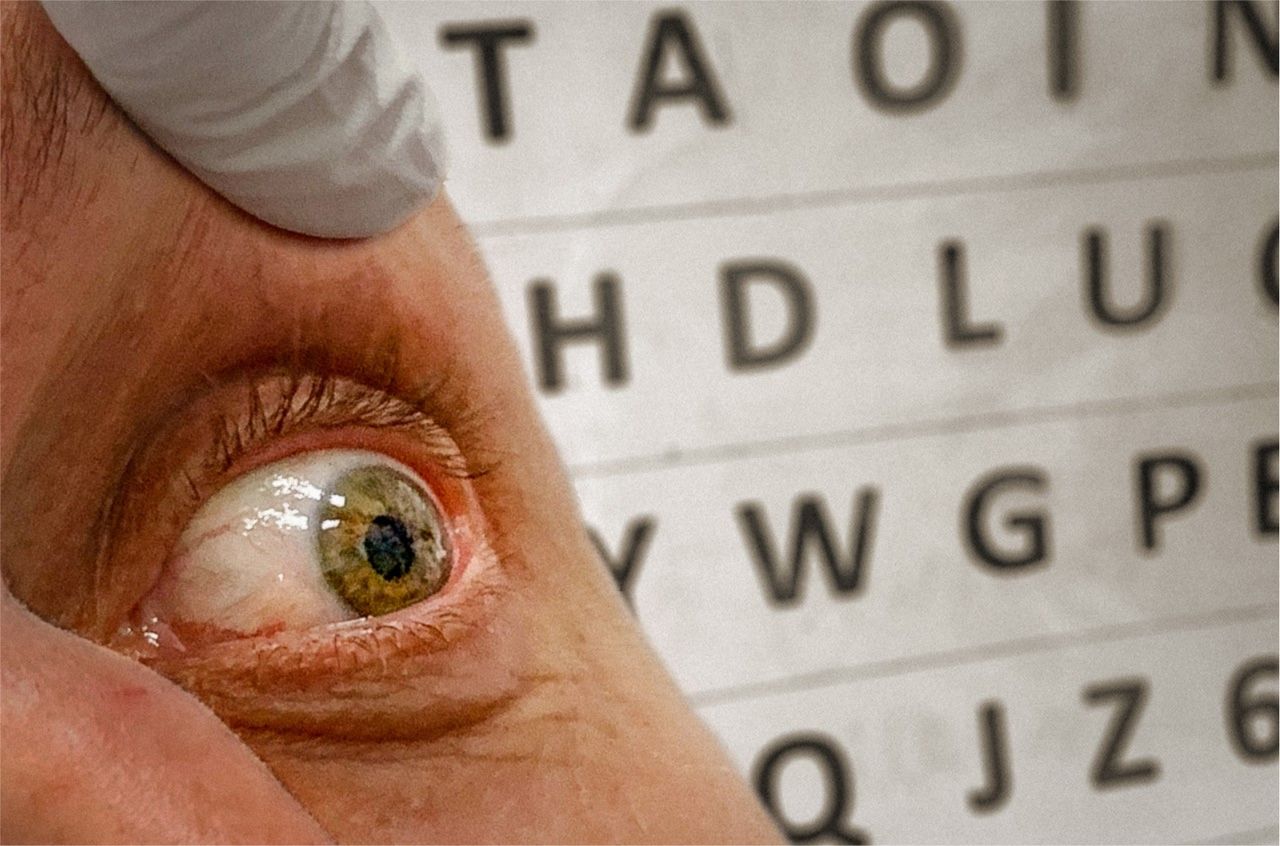
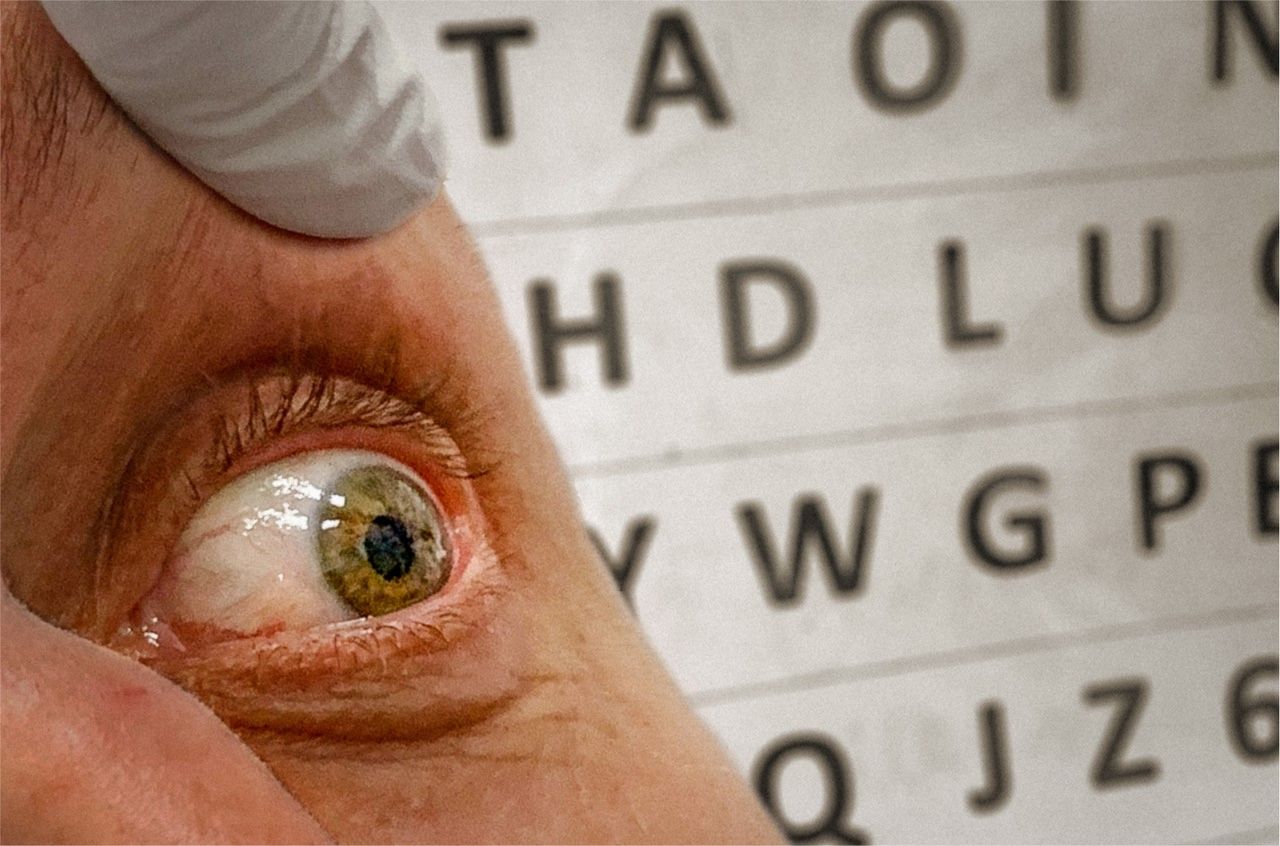
Slight recovery of left eye movement on day 84 allowed communication to be re-established using a two-dimensional frequency-ordered letterboard.1 A nurse read out letters of the alphabet while holding the patient’s left eye open (figure 1). Eye movement indicated letter selection, enabling him to spell individual words.
{kind=link}
For 31 days, this patient was totally locked in and unable to communicate. He slowly regained voluntary muscle function, with slight lateral movement of the left eye returning first. A nurse read out letters of the alphabet while holding his eye open. Eye movement indicated letter selection, enabling him to spell out individual words.
That was a godsend. The nurses who got that started—I can’t thank them enough. That just changed the whole world.
After 31 days of being totally unable to communicate, his first words were,
B O W E L S F U L L
Additional medications were added to his bowel regimen, which resolved the issue.
Between 14 hours and 16 hours, I spent one day just constantly trying to go to the toilet.
Sedation
The treating team decided against sedation during the ‘locked-in’ period, because it would interfere with assessment of recovery, and so potentially prolong the intensive care unit stay, risking further complications. The patient himself would have greatly preferred to have received sedation, had he been consulted.
It was a living nightmare. There was one day where I thought I was going completely mad because I couldn’t control my thoughts … I don’t know what I was given … but I was in a spinning black hole … I didn’t know which way was up and which was down … my mind was bouncing all over the place and I felt like I was going insane. That was the only time that I wished I was dead. I was hoping someone would just put me under.
Discussion
We rarely receive such coherent feedback from our patients, whose recollection is often impaired by illness or drugs. There is little in the intensive care literature directly addressing the issue of the ventilated, locked-in patient who is fully conscious. Nonetheless, even in people with impaired memory, it is important to appreciate that suffering is real even when it cannot be explicitly recalled.
A high PCO2 is not the only factor that induces dyspnoea, a fact established by studies in which awake volunteers have received neuromuscular blocking drugs.2–5 The first such study in 1947 reported ongoing severe dyspnoea and an overwhelming desire to take a deep breath, which was relieved by increasing the rate of ventilation.2 Some of the later studies, which used tidal volumes of 12–15 mL/kg, did not induce such severe dyspnoea.3 Studies in adults with non-compliant lungs, such as in adult respiratory distress syndrome, have led to near-universal adoption of low tidal volume ventilation strategies. We suggest that conscious patients need a higher tidal volume strategy, and that clinicians should actively seek ventilation strategies that do not induce dyspnoea well before the patient’s illness progresses to the point where communication becomes impossible.
Routine physical therapy should be regarded as painful, until it is established otherwise, and pre-emptive analgesic agents given.
It is essential to have clearly stated daily instructions and reminders to ensure that care is consistent and of high quality. These practice points should not depend on handover but be permanently and clearly visible in the bedspace, for example, on the wall behind the patient’s head. Identifying a core team of nursing staff is an effective way to share daily learnings and to ensure consistency of care.
The general intensive care literature emphasises the concept of minimising sedation with daily interruption to reduce the overall duration of mechanical ventilation and the length of stay. Among other benefits, it allows treating teams to assess the patient’s disease course and plan for extubation as soon as possible. For this patient, it was to enable the earliest detection of ability to communicate with the outside world; thus, sedation was felt to be not in his best interests. However, the decision to sedate a patient requires careful consideration, to avoid such a nightmare ‘locked-in’ experience. This could involve input from the patient in the preceding weeks, when communication is still possible.
This patient was troubled by ongoing ‘flashbacks’ at the time of interview, re-experiencing episodes from his admission with accompanying panic-like physiological responses. Although he has largely recovered from the physical disease manifestations, his psychological wounds persist. It is almost impossible to assess the mental state and suffering of a patient who is completely paralysed. However, post-traumatic stress disorder by definition requires a traumatic emotional experience, and we do think that several months of inability to communicate, complete paralysis, painful physical therapy, and an almost constant sense of suffocation fits that definition. Staff caring for such patients must understand that although the patient cannot move or communicate, they can see and hear and are cognitively intact. They might appear deeply sedated and unaware of their surroundings, when in fact the opposite is true and the individual experience may be profoundly unsettling.
Key points
There may be a large gap between clinical assumptions, clinical measurements and the subjective patient experience.
Clinicians should actively seek optimal analgesic regimens and ventilation strategies that do not induce dyspnoea before the illness progresses to the point where communication becomes impossible.
Conscious patients may experience severe dyspnoea even when the arterial PCO2 is low.
Simple measures can establish communication, even in people with minimal movement.
Apparently benign physical therapy may be intensely painful in a paralysed patient.
Ethics statements
Patient consent for publication
Ethics approval
Institutional ethics approval was not required for this manuscript as it is a retrospective discussion of a single patient’s intensive care admission. Written informed consent was obtained from the patient included in this case discussion.
Footnotes
Contributors NK: literature search and writing—original draft. AC: conceptualisation, literature search, writing—review and editing, and supervision. PS: literature search, writing—review and editing, and supervision. HE: writing—review and editing. AG: writing—review and editing.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned. Externally peer reviewed by Robin Howard, London, UK.
Linked Articles
- Editors’ commentary
- Editorial
Other content recommended for you
- BTS/ICS guideline for the ventilatory management of acute hypercapnic respiratory failure in adults
- The predictive value of serial changes in diaphragm function during the spontaneous breathing trial for weaning outcome: a study protocol
- T-piece versus pressure-support ventilation for spontaneous breathing trials before extubation in patients at high risk of reintubation: protocol for a multicentre, randomised controlled trial (TIP-EX)
- Which spontaneous breathing trial to predict effort to breathe after extubation according to five critical illnesses: the cross-over GLOBAL WEAN study protocol
- Volume-targeted ventilation with a Fabian ventilator: maintenance of tidal volumes and blood CO2
- Use of non-invasive ventilation to wean critically ill adults off invasive ventilation: meta-analysis and systematic review
- General medical care on the neuromedical intensive care unit
- Respiratory support
- Weaning from mechanical ventilation in people with neuromuscular disease: a systematic review
- An observational cohort study to determine efficacy, adherence and outcome of the early initiation of pressure support ventilation during mechanical ventilation