Article Text

Abstract
Objectives: Patients with intractable epilepsy may benefit from epilepsy surgery especially if they have a radiologically demonstrable cerebral lesion. Dedicated magnetic resonance imaging (MRI) protocols as performed at epilepsy surgery centres can detect epileptogenic abnormalities with great sensitivity and specificity. However, many patients with epilepsy are investigated with standard MRI sequences by radiologist outside epilepsy centres (“non-experts”). This study was undertaken to compare standard MRI and epilepsy specific MRI findings in patients with focal epilepsy.
Methods: Comparison of results of standard MRI reported by “non-expert” radiologists, standard MRI evaluated by epilepsy “expert” radiologists, and epilepsy specific MRI read by “expert” radiologists in 123 consecutive patients undergoing epilepsy surgery evaluation between 1996 and 1999. Validation of radiological findings by correlation with postoperative histological examination.
Results: Sensitivity of “non-expert” reports of standard MRI reports for focal lesions was 39%, of “expert” reports of standard MRI 50%, and of epilepsy dedicated MRI 91%. Dedicated MRI showed focal lesions in 85% of patients with “non-lesional” standard MRI. The technical quality of standard MRI improved during the study period, but “non-expert” reporting did not. In particular, hippocampal sclerosis was missed in 86% of cases. Neuropathological diagnoses (n=90) were predicted correctly in 22% of “non-expert” standard MRI reports but by 89% of dedicated MRI reports.
Conclusions: Standard MRI failed to detect 57% of focal epileptogenic lesions. Patients without MRI lesion are less likely to be considered candidates for epilepsy surgery. Patients with refractory epilepsy should be referred to an MRI unit with epileptological experience at an early point.
- epilepsy
- neurosurgery
- magnetic resonance imaging
- MRI, magnetic resonance imaging
- HS, hippocampal sclerosis
Statistics from Altmetric.com
The prevalence of epilepsy is 0.5%–1%.1 About 75% of patients with epilepsy can be treated satisfactorily with antiepileptic drugs. However, treated success depends on epilepsy syndrome and seizure types. For example, antiepileptic drugs fail to control seizures in up to 75% of localisation related epilepsies.2–5 For medically intractable epilepsy patients, surgical treatment is the major therapeutic alternative. About 70% of patients who undergo epilepsy surgery become seizure free. The success rate may be even higher in patients with medial temporal lobe epilepsy.6,7
As a result of the constant improvement of image quality, magnetic resonance imaging (MRI) has become one of the most important tools in the selection of patients for epilepsy surgery.8 Congruity of a radiologically demonstrable lesion, ictal epileptic discharges in the EEG, and seizure semiology may permit epilepsy surgery without further invasive diagnostic procedures. In patients in whom scalp EEG recordings are insufficient, MRI abnormalities may generate a hypothesis for intracranial electrode implantation.6
Often, MRI is performed repeatedly during the course of a seizure disorder. It may be undertaken to aid the initial diagnostic process and repeated in patients proving refractory to treatment. MRI protocols with high specificity and sensitivity for epileptogenic lesions have been developed and tested in epilepsy centres. These protocols involve thin slice thickness, high resolution, and, in temporal lobe epilepsy patients, orientation perpendicular or parallel to the longitudinal axis of the hippocampal body.9 However, many patients with epilepsy continue to be investigated using standard MRI “head” sequences. A previous, smaller study comparing standard MRI protocols with a protocol dedicated to the investigation of epilepsy patients between 1993 and 1996 focused exclusively on temporal lobe epilepsy patients.10 In our study, we re-evaluate the sensitivity and specificity of standard versus dedicated MRI in an unselected and larger sample of patients. MRI findings were validated by histopathological results after epilepsy surgery.
METHODS
The records of 536 consecutive patients undergoing presurgical evaluation between January 1996 and June 1999 were reviewed. We included all patients whose records contained all of the following documents: (1) report of standard MRI by the performing (neuro-)radiologist; (2) report of “expert” reassessment of standard MRI; and (3) report of MRI using a dedicated epilepsy protocol. Patients were excluded because at least one of the MRI reports was missing (usually because MRI had not been performed outside our centre or standard MRI was not available for reporting by our “expert” neuroradiologists). Patients with rapidly changing epileptogenic lesions (for example, high grade tumours) were also excluded.
Standard MRIs were undertaken and reported by radiologists not attached to epilepsy centres (“non-experts”). Standard MRI was reported by general radiologists in 47%, and by neuroradiologists in 25% of cases. The qualification of the reporting radiologist was not specified in 28% of standard MRI reports. Reassessment was performed by one of five neuroradiologists with more than three years epileptological experience based in the radiology department of our epilepsy centre (“experts”). MR images were usually re-reported at the time of the patient's first visit to our outpatient department. The “expert” neuroradiologists were informed of the seizure semiology at the time of re-reporting of standard MRI. MRI using our dedicated epilepsy protocol was performed during inpatient presurgical evaluation and assessed by the same group of “experts”. The “expert” neuroradiologists were informed of seizure semiology to aid MRI orientation but they were blinded to other patient data. In particular, “experts” reporting epilepsy dedicated MRI were unaware of previous “expert” or “non-expert” reports of standard MRI.
The inclusion criteria were met by 123 patients. Imaging results could be correlated with neuropathological findings in 90 of these 123 patients who went on to have epilepsy surgery. Most of the 33 patients who did not undergo an operation were considered poor surgical candidates (because of bilateral seizure onset zones, seizure onset zone in eloquent brain areas, or missing hypothesis for placement of intracranial electrodes). A few patients decided against an operation.
Findings were classified into seven categories according to pathological entity (table 1). Standard MRI were considered technically inadequate if patients were scanned in less than three different orientations, or if image quality was unsatisfactory (for example, because of artefacts, low contrast, or low resolution).
Classification of MRI and histological diagnoses as used in this study.
The interval between MRI scans using standard and dedicated epilepsy protocols was quoted when exact examination dates were available (n=90). Patients were divided into an “abnormal” (n=51) and “normal” (n=39) group according to “non-expert” standard MRI reports, and a Wilcoxon signed rank test was calculated (SPSS 10.0, SPSS, Chicago, IL). As the groups differed in size, 12 patients were randomly excluded from the lesional group before the test was performed. The test was repeated five times with different exclusions to ensure that outcome was not biased by exclusions.
MRI according to our dedicated epilepsy protocol was performed on a 1.5 T scanner (Gyroscan ACS-II Philips Medical Systems, Best, Netherlands). Field of view was 220×220 mm and matrix was 256×256. The protocol included: sagittal T1 weighted spin echo sequence (5.0 mm slice thickness, 0.5 mm interslice gap, TR 650 ms, TE 16 ms), axial T2 weighted TSE sequence (5.0/1.0/2876/120), coronal T2 weighted TSE sequence (2.0/0.3/3719/120), coronal T1 weighted inversion recovery sequence (6.0/1.2/2300/40/TI 470 ms), and axial FLAIR sequence (5.0/1.0/6000/120/1900). In patients with temporal lobe epilepsy, sequences were angulated perpendicularly or parallel to the longitudinal axis of the hippocampal body. The dedicated epilepsy protocol used in this study did not include any quantitative MRI (hippocampal volumetry or T2 relaxometry).
RESULTS
All patients (n=123)
“Non-experts” reported 61% (n=75) of standard MR scans as normal or as showing no focal abnormality (fig 1A, 2, 3A, B). Overall, focal lesions were reported in 39% (n=48) of cases (fig 4A). Hippocampal sclerosis (HS) was detected in 7% (n=8) of patients (fig 1A). In the “non-expert” group there were no significant discrepancies between results of general radiologists or neuroradiologists.

Insufficient quality of standard MRI: T2 weighted standard MRI (A) and epilepsy dedicated MRI (B) angulated coronally, orthogonally to the AC-PC plane (A), and orthogonally to the longitudinal axis of the hippocampus (B) (see fig 3). Standard MRI (A) shows no signal abnormalities or atrophy of hippocampus.

Failure of “non-expert” assessment: coronal T1 weighted inversion recovery (A) and axial T2 weighted fast spin echo sequences (B) of standard MRI reported as normal. The right temporo-lateral ganglioglioma on the margin of the image was not seen.
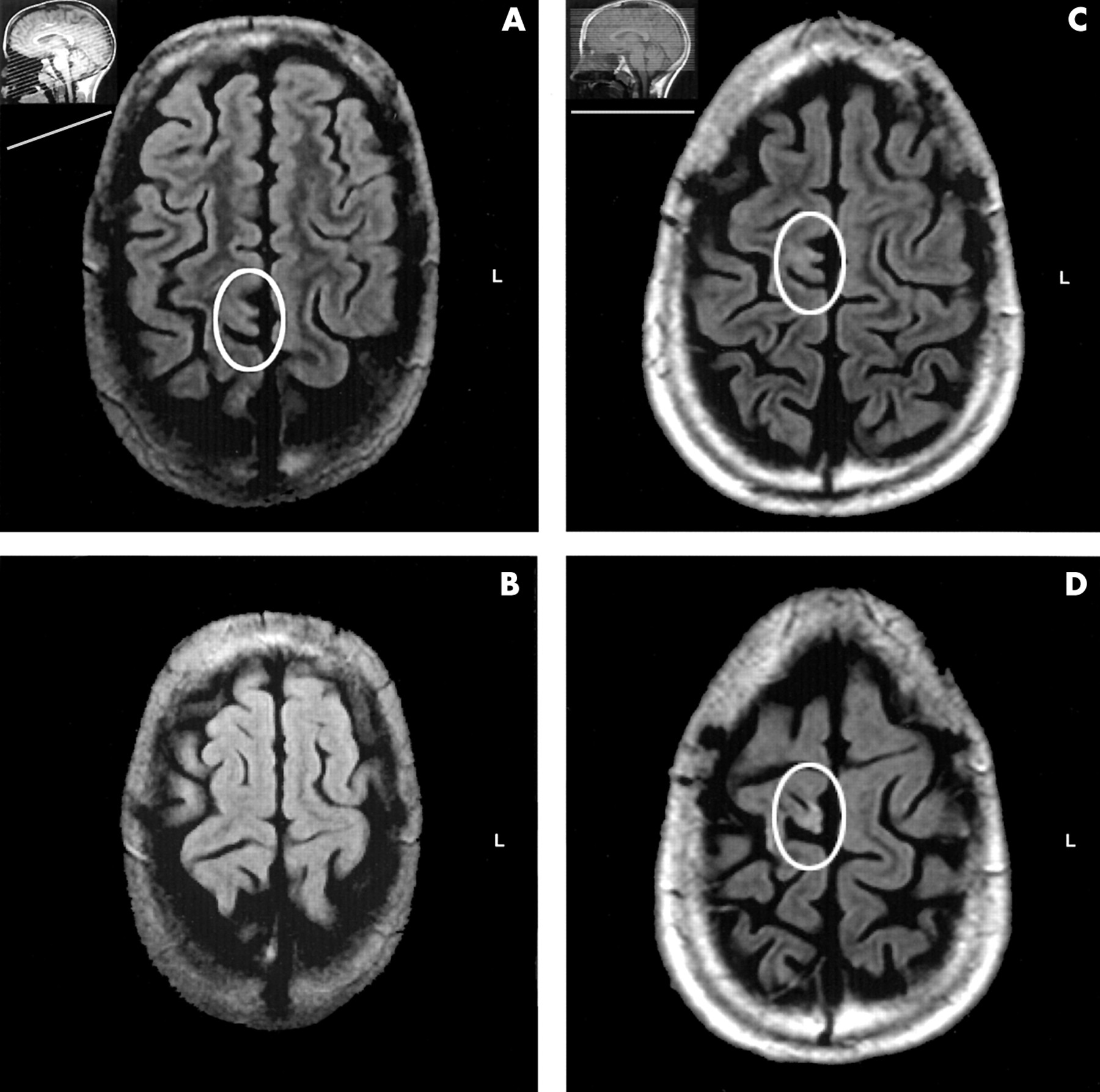
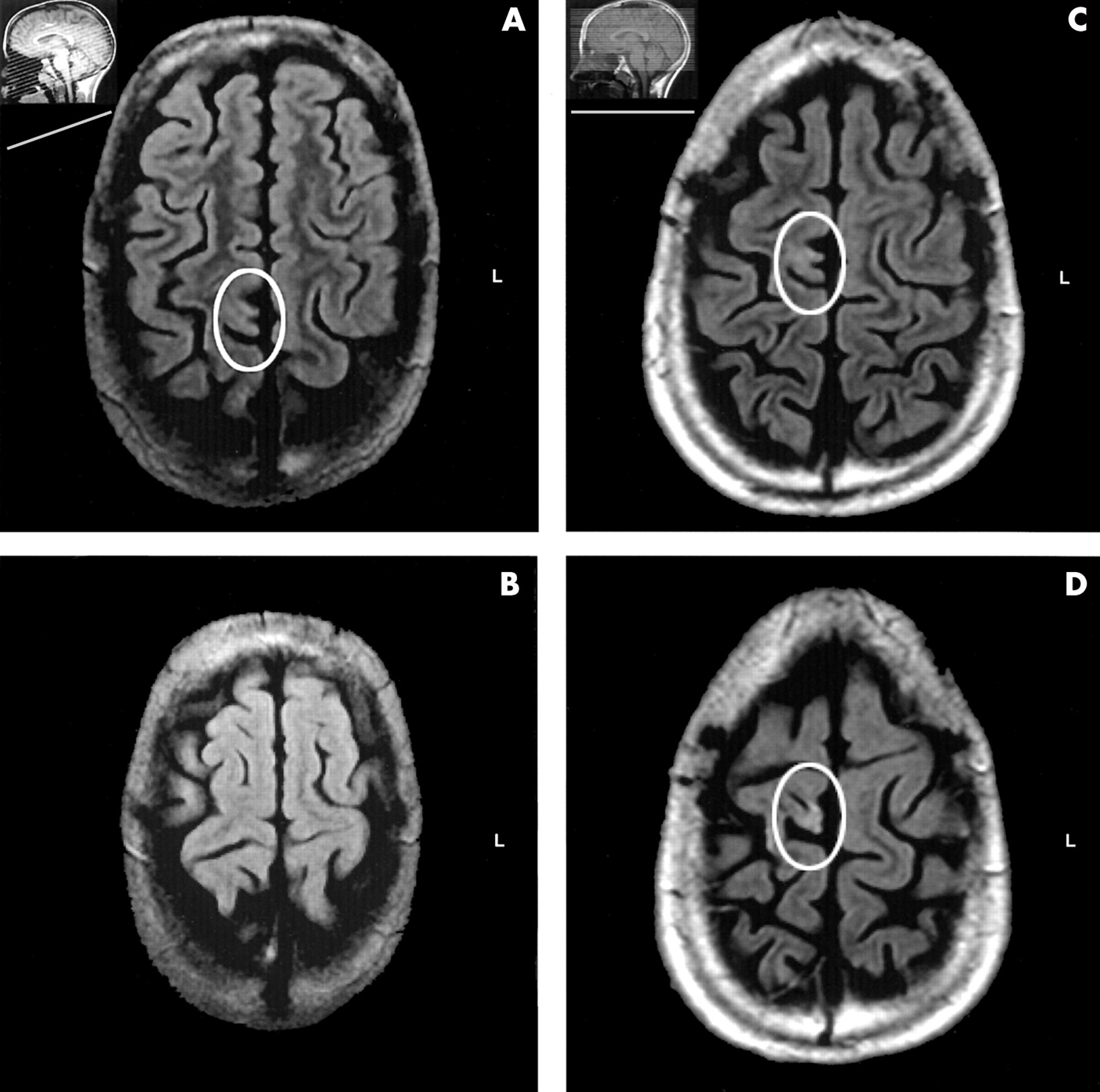
Superiority of a dedicated epilepsy MRI protocol: axial T2 weighted fluid attenuated inversion recovery (FLAIR) sequences of standard (A, B) and specific (C, D) MRI. Despite good image quality of standard MRI, the focal hyperintensity was only visualised in epilepsy dedicated MRI by orientation perpendicular to the sulci and gyrae that corresponds to the AC-PC plane. Scout images in the upper left corner (A, C) indicate different angulation (see fig 1). This example shows that even using a standardised epilepsy dedicated MRI protocol, visualisation of focal lesions may require individualisation depending on the presumed seizure onset zone.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
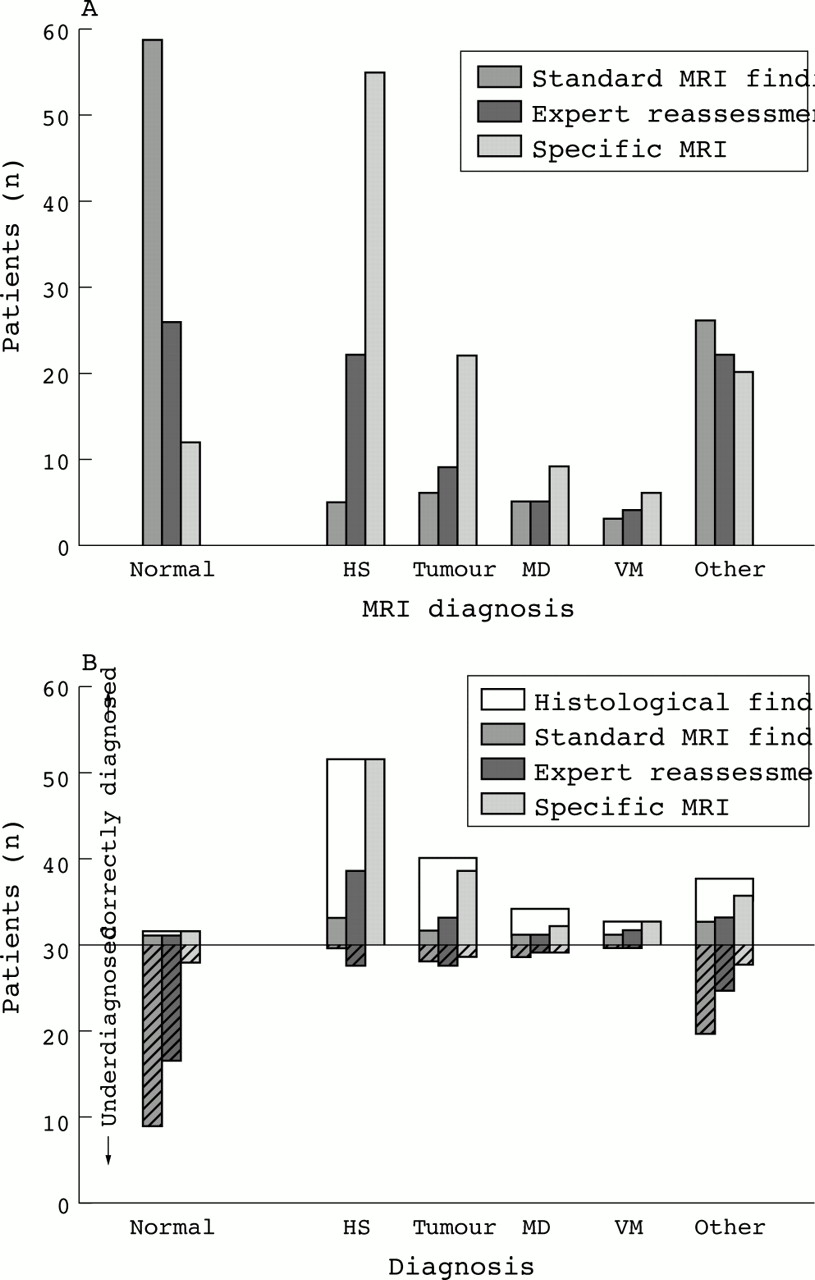
(A) Sensitivity for focal abnormalities of standard MRI, “expert” reassessment of standard MRI by epileptologically experienced neuroradiologists and specific MRI in 123 medically intractable epilepsy patients. Thirty four standard MRI scans classified as technically inadequate by epilepsy “experts” were included in the “normal or no focal abnormality” category. The data indicate that the sensitivity of “expert” reassessment of standard MRI is superior to standard MRI reporting by “non-experts”. Epilepsy dedicated MRI is superior to all. (B) Likelihood of correct diagnosis of the three different MRI results (standard/“non-expert”, standard/“expert”, specific/“expert”) as well as quality of MRI diagnosis in 90 operated patients. MRI misdiagnoses are shown below zero. Data indicate high specificity for epilepsy dedicated MRI and only low specificity for standard MRI as well as many misdiagnoses with standard MRI. Normal=normal or no focal abnormalities, HS=hippocampal sclerosis, MD=migration disorders, VM=vascular malformations, other=other focal abnormalities.
“Expert” reassessment of the same standard MRI classified 28% (n=34) of scans as technically inadequate (although abnormalities were suspected in 8 of 34 patients). “Experts” considered 22% (n=27) of standard MRI scans as normal or to show non-focal abnormalities only (fig 4A). “Experts” found focal lesions in 50% (n=62) of standard MRI scans (fig 2), HS was diagnosed in 18% (n=22) of cases.
Using the dedicated epilepsy MRI protocol, the same group of “experts” described focal abnormalities in 91% (n=112) of scans (fig 1B, 3C, D). HS was detected in 45% (n=55) of cases (fig 1B1). For details of results see figure 4A.
With respect to localisation, “non-expert” standard MRI reports described mesial temporal lobe abnormalities in 9% (n=11) and neocortical lesions in 31% (n=38) of patients. “Expert” reassessment of standard MRI revealed mesial temporal abnormalities and neocortical lesions in 28% (n=34) and 23% (n=28), and dedicated MRI in 50% (n=62) and 41% (n=50) of cases.
Epilepsy surgery patients (n=90)
The likelihood of correct diagnosis of “non-expert” standard MRI findings, reassessed standard, and dedicated epilepsy MRI protocols is given in Fig 4B. The overall specificity for focal lesions of standard MRI findings was 22% (n=20), if re-assessed by “experts” 40% (n=36), and of dedicated MRI 89% (n=80). Comparison with histopathological reports revealed that dedicated MRI was best at predicting HS and vascular malformations, whereas the identification of migration disorders was more difficult (fig 4B).
Non-operated patients (n=33)
Standard MRI of non-operated patients failed to detect any focal lesion in 70% (n=23), with “expert” reassessment in 58% (n=19), and dedicated MRI in 40% (n=13) of patients.
Patients with known scan-scan interval (n=90)
The mean interval between standard and dedicated MRI scans (scan-scan interval) was 21.6 months (range 0.6–70.7). Scan-scan interval of “normal” standard MRI was 25 months (range 4.6–70.7) of “lesional” standard MRI 19 months (range: 0.6–59.4). This difference was statistically significant (p<0.001 in all test repetitions). The proportion of technically inadequate MRIs (definition see Methods section) decreased during the study period although the detection rate of “non-experts” reporting standard MRI did not increase in the same way (table 2). The improvement of standard scan quality with time was reflected by a higher lesion detection rate when standard MRIs were reviewed by “experts”.
Annual sequence of standard MRI findings and “expert” reassessment of standard MRI in medically intractable epilepsy patients (n=90). Quality of standard MRI examination improved during the period but external reading of MRI did not. In some patients standard MRI was classified insufficient but focal lesion could be identified anyhow
DISCUSSION
Sensitivity for the detection of focal lesions was low if standard MRI sequences were reported by “non-experts”, significantly higher if the same pictures were analysed by epilepsy “experts”, and higher again with dedicated epilepsy MRI protocols. In terms of likelihood of correct diagnosis, the discrepancy between standard MRI and dedicated MRI was even larger. Our data show that MRI of patients with refractory focal epilepsy should be undertaken by epileptologically experienced neuroradiologists using epilepsy specific imaging protocols.
“Non-experts” using standard MRI missed abnormalities in the mesial temporal lobe more frequently than neocortical changes. Most mistakes were made with regard to HS, the most common MRI diagnosis in medically intractable epilepsy. The discrepancy between “expert” reassessment of standard MRI and specific MRI scans of the same patients reflects the superiority of dedicated epilepsy scanning protocols in this clinical context. Such protocols include an individual orientation, thin slice thickness and high resolution. “Experts” using epilepsy dedicated MRI can detect HS with a sensitivity and a specificity of over 90%.11–13
Standard MRI was usually performed before referral for epilepsy surgery evaluation, dedicated MRI during inpatient evaluation resulting in a mean time interval between standard and dedicated MRI of almost 22 months. Patients with normal standard MRI had significantly longer scan-scan intervals, suggesting that the “normal” scan contributed to a delayed referral for presurgical evaluation. The scan-scan delay could have biased our study in favour of specific MRI because of progressive tissue changes. However, most of the detected lesions were non-progressive. Previous MRI studies of HS have shown minimal progression of hippocampal damage over time.14,15 Patients with rapidly growing lesions, like tumours WHO grade III or IV were excluded. Tissue changes occurring during the scan-scan interval in this study are therefore unlikely to explain the different results obtained by standard and specific MRI examinations. Furthermore, “expert” reassessment of standard MRI produced markedly better results than external standard MRI reporting. Interestingly, there were no false positive findings at all in any of the non-expert acquired and reported scans in this study. The main problem detected here is therefore one of underdetection and underreporting, and not of overreporting of abnormalities. We do, however, come across false positive non-expert reports in our clinical practice and results of standard MRI should be carefully verified before a decision about epilepsy surgery is made.
Our results correspond to those of a previous study comparing standard and epilepsy dedicated MRI protocols in medically intractable temporal lobe epilepsy patients.10 In that study, standard MRI failed to show focal abnormalities in 34 of 51 (67%) patients, and missed 32 of 34 temporal lesions including 27 cases of HS. However, the study did not include “expert” reassessment or an evaluation of scan-scan intervals. It was undertaken at a time (1993–96) when the technical differences between standard and specific MRI may have been more significant. Over the period of the present study (1996–99), image quality of standard MRI increased resulting in fewer inadequate scans, but the interpretation of the obtained images by “non-experts” showed no improvement. It is important to emphasise that a dedicated epilepsy MRI protocol can be performed on almost any 1.5 T MRI scanner without additional software. However, the fact that standard MRI reporting of “experts” was superior to reporting by “non-experts” suggests that despite general improvements of image quality best results will be obtained by dedicated MRI assessed by experts at epilepsy centres. It should be noted that, since completion of this study, we have improved our dedicated epilepsy protocol further by including a coronal FLAIR sequence as well as a three dimensional T1 weighted acquisition for further postprocessing analysis such as reformatting and quantitative evaluation. We no longer acquire the sagittal T1 weighted sequence.
Patients with medically intractable epilepsy do not just have recurrent seizures. Their illness causes social stigma and disability.16 Epilepsy is a considerable social burden.17–19 A lesion detected early in the course of a seizure disorder by dedicated MRI, and good surgical prospects can have tremendous consequences for patients with medically intractable epilepsy. Quality of life improves after surgical treatment,20 early surgery is associated with better socioeconomic outcome,21 functional deficits can improve after surgical intervention,22 and the risk of injury and premature death are significantly lower after successful surgery.23–25
Epilepsy patients who do not respond to the first two antiepileptic drugs are likely to have drug resistant epilepsy.5 Our data suggest that such patients should undergo MRI using a dedicated epilepsy protocol, and that there is need for a more appropriate training of (neuro-)radiologists to read the scans by a standardised interpretation approach.26 The use of standard MRI in epilepsy should be limited to the exclusion of abnormalities, which have to be treated irrespective of epileptological considerations at the onset of the disorder like stroke or malignant brain tumours.
Acknowledgments
We would like to thank L Solymosi, J Reul, B Ostertun, and E Keller for expert (re)assessment of standard and epilepsy dedicated MRI during the period described above. Furthermore, we thank the involved epilepsy surgeons, D van Roost and J Schramm, as well as the neuropathologists, I Bluemcke and O D Wiestler, for specimens and analysis.
REFERENCES
Footnotes
-
Competing interests: none declared.