Article Text

Abstract
This case is reported to raise awareness of herpes simplex encephalitis as a persisting brain disorder. A 66 year old immunocompetent man developed status epilepticus and died of pneumonia in the course of progressive hemiparesis, cognitive decline, and atrophy of the brain over a five year period after herpes simplex encephalitis. In addition to a completely destroyed left temporal lobe, necropsy revealed active encephalitis consisting of necrosis and lymphocyte infiltration with a large number of intranuclear inclusions in the neurones and glial cells in the markedly oedematous parenchyma of the right frontal and parietal lobes. Herpes simplex virus type 1 (HSV-1) antigen was detected by immunohistochemistry, HSV-1 DNA by in situ hybridisation, and herpes simplex virus nucleocapsids by electronmicroscopy. These clinical and pathological findings suggest that direct viral reactivation might result in a relapse of herpes simplex encephalitis, causing progressive clinical deterioration associated with the persistence of HSV-1 in the brain. This is the first case report demonstrating HSV-1 antigen, HSV-1 DNA, and herpes simplex virus nucleocapsids in a case of relapsing herpes simplex encephalitis.
- encephalitis
- herpes simplex virus
Statistics from Altmetric.com
Herpes simplex encephalitis is the most common non-epidemic form of viral encephalitis. Its typical clinical presentation is of an acute febrile illness with behavioural abnormalities, decreased level of consciousness, and focal neurological signs. The common neurological sequelae of this disease include memory impairment, behavioural and cognitive abnormality, and secondary epilepsy.1 It has been reported recently, on the basis of the detection of viral DNA and persistent immunohistochemical activity in the brain, that herpes simplex virus type 1 (HSV-1) might persist within the human central nervous system following recovery from encephalitis.2,3 However, the role of persistence of the viral infection and its contribution to neurological sequelae after herpes simplex encephalitis remains obscure.
We report the necropsy findings in a case of relapsing herpes simplex encephalitis presenting as progressive neurological deterioration over a five year period following the initial episode of herpes simplex encephalitis. The role of persistent herpes simplex virus infection and the pathogenesis of relapsing herpes simplex encephalitis are discussed in relation to the therapeutic problem.
CASE REPORT
A 61 year old man with a 10 year history of pneumoconiosis presented at our hospital with high fever and confusion. Three days later, he was admitted to our department because of a tonic-clonic seizure. On admission, he had global aphasia with no limb weakness or sensory disturbance. The initial diagnosis of herpes simplex encephalitis was made by the presence of intrathecal synthesis of antibodies specific to HSV-1 and the presence of HSV-1 DNA in the cerebrospinal fluid detected by polymerase chain reaction (PCR). Brain computed tomography (CT) and magnetic resonance imaging on the day of admission were normal, but single photon emission computed tomography (SPECT) showed hyperaccumulation of 99mTc-HM-PAO in the left temporo-occipital area. Treatment with acyclovir (30 mg/kg daily) was begun and continued for 14 days. After the treatment period, the patient became alert and was able to obey simple commands. He was discharged with mild aphasia. Brain CT on the 60th day showed slight atrophy of the left temporal lobe (fig 1A⇓).

Progression of brain atrophy on brain computed tomography (CT). (A) CT on the 60th day after disease onset. (B) CT during the final episode.
After this initial episode, the patient experienced many right sided partial seizures as well as some tonic-clonic seizures over the next five years. Two years after the initial episode, gradual paralysis developed in the left arm, becoming total in the third year. His level of cognition also gradually declined and he became impatient and easily excited by the third year. In the fourth year, his left leg became paralysed and he became wheelchair-bound. He seemed to lose the volition to move and stayed in bed all day long.
Five years after the initial encephalitis, the patient developed status epilepticus without any prodromal symptoms. On admission, he was cyanotic, unresponsive to pain, and breathing faintly. His pupillary reflexes to light were slow. Brain CT showed marked atrophy of the whole brain and diffuse white matter changes (fig 1B⇑). He soon developed a severe bacterial pneumonia caused by Klebsiella pneumoniae and remained in coma. At this time a clinical diagnosis of “anoxic encephalopathy” caused by status epilepticus was made. He died of respiratory failure on the 15th hospital day.
Neuropathological findings
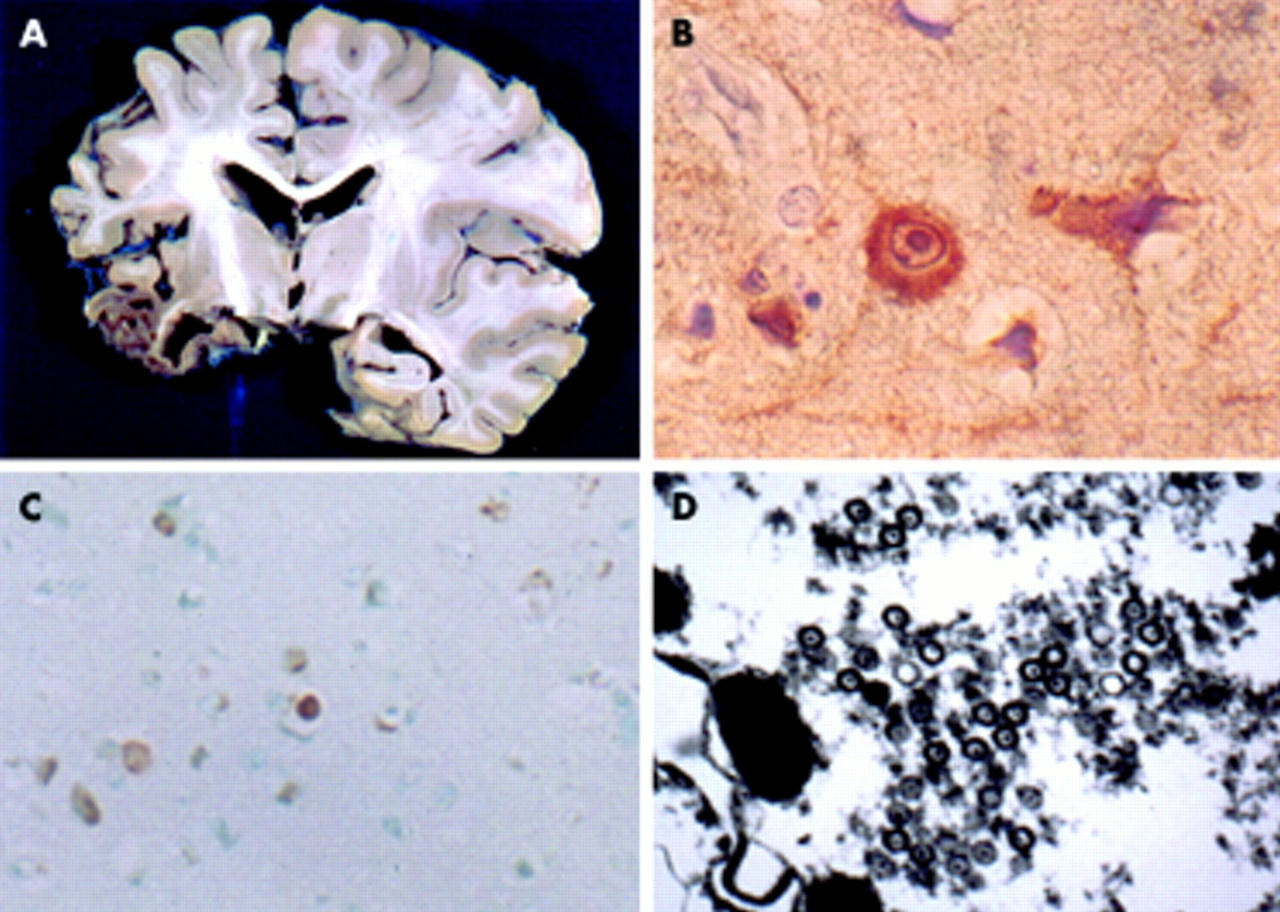
Multiple cavitations and cystic changes were observed in the left temporal lobe, along with apparent swelling in the right frontal and parietal lobes (fig 2A⇓). Microscopic examination showed not only complete destruction of the left temporal lobe with burnt out lesions involving extensive neuronal loss, gliosis, and calcification, but also necrosis of the brain parenchyma with severe oedema and congestion in the right frontal and parietal lobes. In these lesions, perivascular infiltration of lymphocytes was detected and many neurones and glial cells had intranuclear inclusions in the cortex and white matter. However, gliosis and mineralisation were not observed in those regions. HSV-1 antigen was detected immunohistochemically and HSV-1 DNA was demonstrated by in situ hybridisation within the nucleus and cytoplasm of both neurones and glial cells in the right frontal and parietal lobes (fig 2B and C⇓). Herpes simplex virus nucleocapsids were also observed by electron microscopy within the nucleus and cytoplasm of these cells (fig 2D⇓). No anoxic changes were seen in any of the brain regions.

{kind=link}
{kind=link}
(A) Coronal section at the level of the basal ganglia showing destruction of the left temporal lobe and swelling of the right parietal lobe. (B) Immunohistochemical photomicrogragh of the right parietal lobe showing HSV-1 antigens within the cytoplasm and the nucleus of neurones (magnification ×330). (C) Positive HSV-1 DNA in cells in the right parietal lobe, in situ hybridisation for HSV-1 (ENZO; HSV BioProbe labelled probe; magnification ×168). (D) Electron photomicrogragh showing herpes-type nucleocapsids within the nucleus of a neurone in the right parietal lobe (magnification ×24 730).
DISCUSSION
This report contributes two important clinical and pathological insights to our knowledge and understanding of herpes simplex encephalitis.
First, the persistence of the virus in the brain following herpes simplex virus encephalitis may be associated with progressive neurological deterioration. Thus long term follow up of neurological sequelae is important. It is not unusual to find a persistent inflammatory process in patients who have survived herpes simplex encephalitis for months or years.4 However, its contribution to the clinical picture has not so far been determined. Two large prospective studies reported that 18% and 42% of survivors of herpes simplex encephalitis treated with acyclovir have severe neurological deficits.5,6 However, the period of follow up in these studies was inadequate. There have been few studies on adult patients with progressive clinical deterioration over a period of years following herpes simplex encephalitis. According to one long term prospective study of the cognitive sequelae of herpes simplex encephalitis, one of eight adult patients with this disease experienced progressive clinical deterioration.7 In children, there are reports describing progressive mental and behavioural deterioration for many years following herpes simplex encephalitis.3,8,9 Most of these patients developed intractable seizures, slowly progressive hemiparesis, and cognitive decline some years after contracting the disease. Neuropathological studies of these patients showed chronic active encephalitis, consisting of meningeal and perivascular infiltration of lymphocytes with severe gliosis and mineralisation. In those brain tissues, herpes simplex virus expression could not be detected by immunohistochemical methods, though specific viral DNA was demonstrated by PCR. These observations suggested that persistence of the virus after herpes simplex encephalitis may be associated with chronic inflammation, resulting in neurological problems in paediatric patients. In a similar manner, our patient developed right sided partial and tonic-clonic seizures, showed insidious development of weakness in the right arm and leg, and experienced progressive deterioration of cognitive function over five years. This clinical deterioration and seizure pattern, together with the progressive brain atrophy observed on brain CT, is compatible with a chronic encephalitis. To our knowledge, no pathological study of an adult patient with documented clinical deterioration following herpes simplex encephalitis has been reported before.
Second, patients may suffer from relapsing herpes simplex encephalitis many years after the initial infection, possibly because of reactivation of the virus. The neuropathology described here in the right frontal and parietal lobes, consisting of many inflammatory cells and necrosis with severe oedema and congestion, without gliosis or mineralisation, is suggestive of acute rather than chronic active encephalitis. We think that our patient experienced a fulminant reactivation of the disease—that is, relapsing herpes simplex encephalitis —in the course of a chronic infection with the virus. Although the pathogenesis of relapsing herpes simplex encephalitis remains unclear, previous studies have suggested that it may be caused either by reactivation of the virus10 or by immune mediated encephalopathy.11 This is the first report to show HSV-1 antigens, HSV-1 DNA (by in situ hybridisation), and herpes simplex virus nucleocapsids in relapsing herpes simplex encephalitis. These findings strongly support the hypothesis of direct involvement of the virus in relapsing herpes simplex encephalitis. Many patients experience relapses of encephalitis, even after acyclovir treatment for the initial infection. In most cases, the relapse occurs early, within weeks of the initial encephalitis. When our patient developed status epilepticus five years after his initial episode of herpes simplex encephalitis, without any prodromal symptoms, we did not suspect that the cause was relapsing encephalitis. It has been suggested that the likelihood of a relapse is related to an inadequate duration of antiviral treatment, and a longer period of treatment is now recommended. The progressive neurological deterioration and relapse observed in this case might reflect the failure of a 14 day course of acyclovir to eradicate the initial infection completely. Acyclovir is a synthetic acyclic purine nucleoside analogue that selectively inhibits herpes simplex virus replication. Thus any virus that is not in a replication cycle might survive the acyclovir treatment. Nevertheless, even with an expanded treatment period the possibility that the virus might persist in the brain after herpes simplex encephalitis and could then cause chronic infection or relapsing encephalitis cannot be excluded. Periodic courses of acyclovir over several years may be indicated.
Conclusions
We believe that the prevalence of relapsing herpes simplex encephalitis may be underestimated and the condition misdiagnosed. As occurred in our patient, the first manifestation of relapsing encephalitis may be the development of status epilepticus, which is difficult to distinguish from secondary epilepsy. Thus when encountering a patient with epilepsy who has experienced herpes simplex encephalitis in the past, it is important to remember that the patient may be experiencing a relapse of the encephalitis, and antiviral treatment should be considered.
REFERENCES
Footnotes
-
Competing interests: none declared