Article Text

Abstract
Background: Limbic encephalitis is a potentially treatable immunological condition. The presence of voltage-gated potassium channel antibodies (VGKC-Ab) in the cerebrospinal fluid (CSF) and serum of patients with the condition is a marker of the disease associated with a non-paraneoplastic form and good response to treatment. Recent work has highlighted absent serum VGKC-Ab and distinct immunology in patients with the paraneoplastic form of limbic encephalitis.
Methods: The cases of four patients with the typical clinical presentation, neuropsychological features and brain imaging of acute limbic encephalitis, in the absence of any evidence for associated cancer during a follow-up of at least 18 months are described here.
Results: All patients had negative testing for VGKC-Ab measured during their acute presentation. All patients made some recovery, although they were left with marked cognitive deficits and persistent seizures.
Conclusion: These cases demonstrate that the absence of VGKC-Ab in limbic encephalitis does not necessarily imply a paraneoplastic form. Further work is required to establish the immunological basis for the disorder in these patients, and the optimal treatment regimen.
- CPS, complex partial seizures
- CSF, cerebrospinal fluid
- VGKC-Ab, voltage-gated potassium channel antibodies
Statistics from Altmetric.com
- CPS, complex partial seizures
- CSF, cerebrospinal fluid
- VGKC-Ab, voltage-gated potassium channel antibodies
Limbic encephalitis is characterised by three features: a core amnesic syndrome, complex-partial and secondary-generalised seizures, and a variable affective prodrome.1,2 The core memory syndrome includes profound anterograde amnesia with variable recovery.1,3 The syndrome is associated with an isolated high signal in the mesial temporal lobes on MRI scan4 and histological inflammatory change in these areas.5,6
Limbic encephalitis was initially identified as a paraneoplastic phenomenon, occurring more commonly with occult small-cell bronchial carcinoma (in association with autoantibodies to Hu), testicular carcinoma and thymoma (in association with antibodies to CRMP5/CV2).7 In recent years, a non-paraneoplastic variant has been characterised.2,8 Patients with this form have been shown to express increased levels of voltage-gated potassium channel antibodies (VGKC-Ab) in their serum. This antibody is also expressed in Morvan’s syndrome,9 also with affective and memory components. The detection of such antibodies in serum was established by radioimmunoprecipitation asssays using α-dendrotoxin, which binds to the Kv1.1, Kv1.2 and Kv1.6 ion channel subunits.10,11
More recently, a second antibody has been identified in patients with a paraneoplastic form of the disorder, a subacute course (where the syndrome can evolve over weeks rather than days) and negative VGKC-Ab.12 This antibody in the serum and cerebrospinal fluid (CSF) reacts to the neuropil of the hippocampus and cerebellum. This is in contrast with other paraneoplastic syndromes where the antibody reacts either to oligodendrocytes or to the neuronal cytoplasm. The work suggests the existence of immune-mediated bases for both paraneoplastic and non-paraneoplastic forms of the disorder, where these bases are distinct. Consistent with an underlying immunological cause, non-paraneoplastic2,13 and paraneoplastic6,14,15 types of the condition have both been shown to respond to immunotherapies including intravenous steroids, immunoglobulins and plasma exchange. Moreover, the antibody titre in non-paraneoplastic2,12,13 and paraneoplastic types12 has been shown to reflect clinical response to treatment.
The above studies suggest characteristic antibody “profiles” for neoplastic and non-paraneoplastic forms of the disorder, where the non-paraneoplastic form of the disorder is associated with VGKC-Ab. Here, we provide evidence for a broader immunological spectrum of non-paraneoplastic limbic encephalitis. We describe four patients with the typical features of acute limbic encephalitis with no evidence of associated cancer in the absence of serum VGKC-Ab.
METHODS
Patients were referred to the neurology service at the Newcastle Hospitals Trust between 2002 and 2005 and seen in the cognitive neurology clinic. All patients had an amnesic syndrome associated with seizures. Measurement of serum VGKC-Ab titres by radioimmunoassay using rabbit brain homogenate10 was carried out within 4 weeks of admission (John Radcliffe Hospital, Oxford, UK) and defined as negative if <100 pM.
All patients had screening memory assessment during the acute presentation using measures including the Addenbrooke’s Cognitive Examination.16 All patients received subsequent detailed assessment including assessment of current intellectual function (Wechsler Adult Intelligence Scale, 3rd edition17) and memory function (Wechsler Memory Scale, 3rd edition17,18). Executive function was assessed at outcome using the Trail Making and Controlled Verbal Fluency Tests.19,20 Patients 2 and 3 underwent detailed neuropsychological assessment at 2 months and at intervals of <12 months thereafter. All four patients underwent detailed assessment of neuropsychological outcome at 18, 20, 27 and 26 months. At presentation and during follow-up, seizures were identified clinically and seizure activity was assessed using EEG.
All patients underwent MRI scanning to seek increased signal in the hippocampus. All underwent CSF examination, serological testing for herpes simplex virus and polymerase chain reaction on CSF for herpes simplex virus. Where clinically indicated, serological testing for Borrelia, Coxiella, Epstein–Barr virus, HIV and herpes zoster virus was also performed. All patients underwent an extended autoantibody screen, including serological testing for antinuclear and extractable nuclear antigens and for thyroid-peroxidase antibodies.
Associated cancer was sought on the basis of screening investigations and clinical follow-up of between 18 and 32 months. All patients underwent chest radiography and CT scanning of the chest, abdomen and pelvis. One patient underwent a negative testicular ultrasound after the incidental finding of a possible lesion on examination. Screening investigations included the following autoantibodies as appropriate: onconeural antibodies (anti-Hu and Purkinjie/Yo, CRMP5 extracted using immunofluoresence techniques with monkey cerebellum as substrate), α-fetoprotein, carcinoembryonic antigen, Ca125, Ca153, Ca199 and porcine serum albumin. Serum protein electrophoresis and assessment of urine for Bence–Jones protein was also completed for all patients.
RESULTS
Presentation features
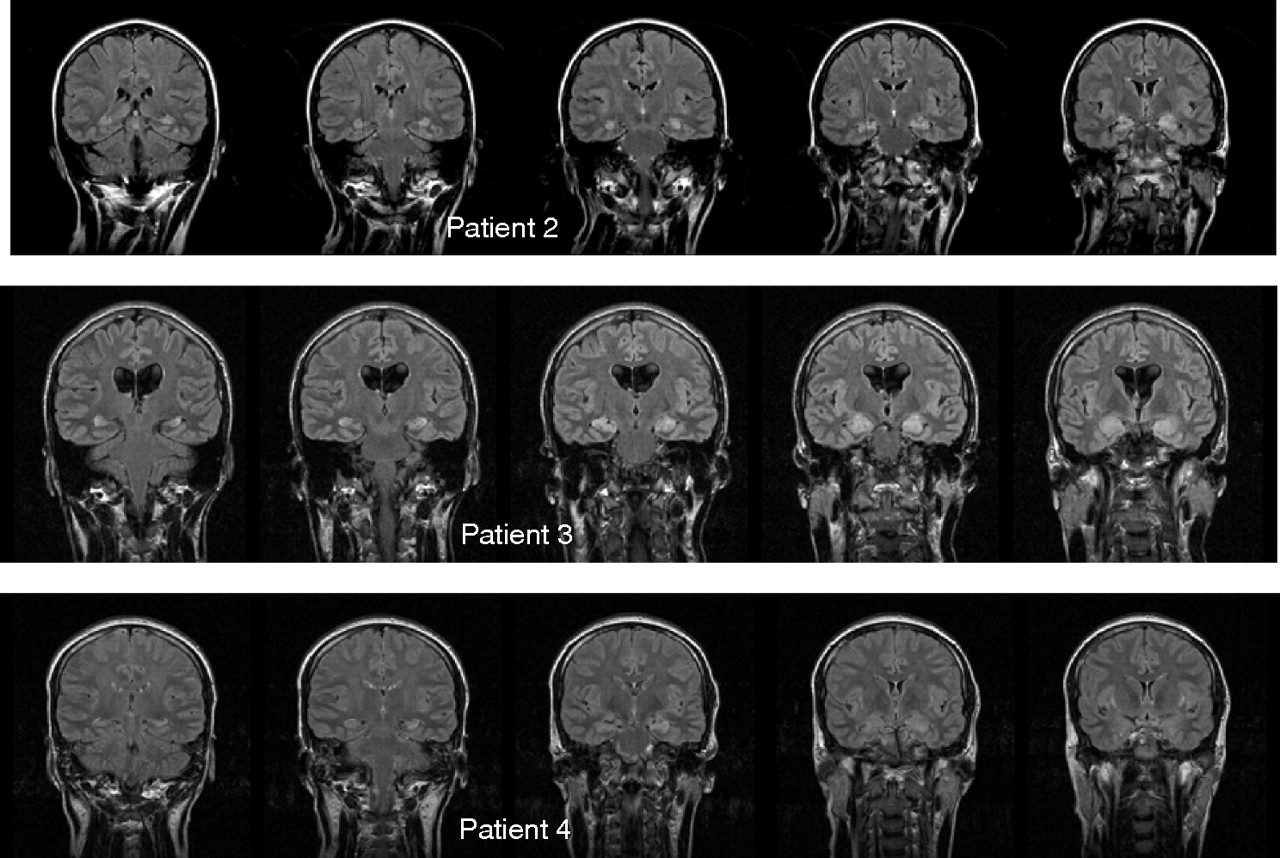
Table 1 details the clinical presentation of the patients and the supplementary information. All the patients demonstrated features similar to acute limbic encephalitis with positive VGKC-Ab. All four patients experienced a prodromal illness before an amnesic syndrome in association with seizures that developed acutely (symptoms evolved over less than 1 week). All patients showed highly localised hippocampal signal change on MRI that evolved during the acute admission (fig 1), and were negative for VGKC-Ab during the first 4 weeks.
Clinical characteristics of the patients
{kind=link}
Coronal fluid-attenuated inversion recovery (FLAIR) sequences for patients 2, 3 and 4 acquired within 4 weeks of onset of acute encephalitis. All patients shown had imaging using identical FLAIR sequences earlier in the course of acute illness showing either normal appearances (patients 2 and 3) or less marked signal change in the medial temporal lobe (patient 4).
Neoplasia screen
The detailed initial screen for cancer was negative in all patients and there was no evidence for cancer during follow-up of between 21 and 33 months.
Outcome
All patients exhibited an acute syndrome with variable recovery and all were left with residual cognitive deficits and seizures (case reports in supplementary information are available at http://jnnp.bmjjounals.com/supplemental). Behavioural and affective features were present in all four patients, and three of the four patients had non-epileptic attacks. The detailed neuropsychological assessment (supplementary tables A–C) revealed outcome measures of intelligence, memory and executive function that were impaired for all four patients relative to estimates of premorbid function. All the patients showed verbal and performance intelligence indices that were considerably below premorbid estimates (supplementary table A), general memory and working memory indices that were considerably below premorbid estimates (supplementary table B) and deficits in outcome executive function assessed by Trail Making19 and verbal fluency20 (supplementary table C).
DISCUSSION
These patients had a stereotyped syndrome characterised by an infective prodrome, an acute amnesic syndrome with seizures evolving over less than 1 week and highly focal hippocampal MRI signal change. The patients showed variable recovery and all had persistent cognitive impairment and seizures. These features are similar to previously reported cases of acute limbic encephalitis in association with VGKC-Ab,2,13,21,22 although the previous cases have not been characterised in such detail in terms of the neuropsychological outcome (see supplementary information). In contrast with the previous reports of acute limbic encephalitis, all the patients had negative VGKC-Ab on the basis of immunological testing at the national testing centre during the first 4 weeks when this would be most likely to be positive.
These cases are distinct from previous cases of limbic encephalitis with negative VGKC-Ab.12 Previous cases exhibited a subacute course (symptoms evolved over weeks or months) and were associated with cancer, in contrast with our patients with an acute syndrome (evolving over less than 1 week after a prodrome) with detailed screening and follow-up for at least 18 months providing no evidence for cancer. Additionally, CSF cell counts in our patients were absent or minimal, in keeping with those of patients with VGKC-Ab2 and in contrast to those with a confirmed malignancy.12 The finding of a mildly increased CSF protein in two of the four patients has been replicated in patients both with12,13 and without2 an underlying malignancy, and is therefore not diagnostic.
Signal change on MRI fluid-attenuated inversion recovery was restricted to the hippocampi and amygdalae in all four patients. Isolated reversible temporomesial change has previously been shown in patients with limbic encephalitis.23 Reversible signal change in the hippocampi, thought to be due to seizure-induced oedema or gliosis,24 has also been associated with prolonged seizures and is therefore a possible explanation in these patients. The specificity of the changes to hippocampal areas is striking; however, in our view, circumstantial evidence for a primary autoimmune process.
The outcome measures in this study show that the disorder has a cognitive profile that is more complex than a simple disorder of memory, with additional deficits in performance intelligence and executive function. All patients also had affective or behavioural features. This combination of cognitive and affective or behavioural features represents a major obstacle to the rehabilitation of such patients.
The striking similarity in the clinical features and imaging in these patients seems consistent with a common autoimmune basis, where this basis is distinct from cases with positive VGKC-Ab, and from cases with negative VGKC-Ab, in association with cancer. Current guidelines regarding the diagnostic criteria for paraneoplastic limbic encephalitis recommend that a 5 year “tumour window” from the time of presentation should have elapsed before a paraneoplastic cause is considered unlikely.25 However, these patients were followed up for at least 18 months, and had prodromal illnesses strongly suggestive of a process with an infectious trigger.
In the absence of a clear-cut immune basis, the place of immune treatment in these patients is not established. One of the two patients given steroids (patient 1) showed a probable response to steroids after 12 months, although the effect of early steroids on the acute illness in patient 3 is harder to infer. On the basis of responses in positive and negative VGKC-Ab cases in association with cancer, we think that immune treatment should be considered carefully in all cases such as these.
Acknowledgments
We thank P Chinnery and T Williams (Department of Neurology, Newcastle upon Tyne Hospitals Trust) for referring patients, and D Birchall, P English and P Colls for opinions about MRI data and practical assistance.
REFERENCES
Supplementary materials
Files in this Data Supplement:
Footnotes
-
Published Online First 10 November 2006
-
Competing interests: None.