Article Text

Abstract
Objective To describe the spectrum and outcome of central nervous system complications associated with immune checkpoint inhibitors (CNS-ICI).
Methods Patients with CNS-ICI were identified and their characteristics compared with ICI-related peripheral neuropathy (PN-ICI).
Results We identified 19 patients with CNS-ICI. The patients were receiving nivolumab (n=8), pembrolizumab (n=6), a combination of ipilimumab-nivolumab (n=3), ipilimumab-durvalumab (n=1), or atezolizumab (n=1). Underlying malignancies included non-small-cell lung cancer (n=8), melanoma (n=3), and other less common tumours (n=8). Neurological phenotypes were limbic encephalitis (n=8), meningoencephalitis (n=4) and cerebellitis (n=4). Two patients developed isolated confusion and one parkinsonism. Associated autoantibodies included onconeural (Ma2, n=7; Hu, n=1), astrocytic (glial fibrillar acidic protein, n=2) and neuronal surface (contactin-associated protein-like 2, n=1) specificities. ICIs were withheld and corticosteroid treatment was given in all cases. Five patients received intravenous immunoglobulin, two rituximab, one plasmapheresis and one infliximab. Overall, six patients died. Readministration of ICI was attempted in three patients, without further relapses. Non-small-cell lung cancer was significantly more frequent in patients with CNS-ICI (p<0.01), while melanoma and ipilimumab treatment were more common in PN-ICI (p<0.01 and p=0.01). Conversely, CNS-ICI cases were more frequently antibody-positive than PN-ICI (p<0.01) and showed a strong trend towards poorer outcome (p=0.053).
Conclusion Three main clinical phenotypes characterise CNS complications of ICIs, each with distinct immunological background, disease course and response to treatment. Other clinical manifestations (including parkinsonism and steroid-responsive confusion) are also possible. Underlying cancers, antibody prevalence and outcome appear different from those of patients with PN-ICI.
Statistics from Altmetric.com
Introduction
Immune checkpoint inhibitors (ICIs) are novel oncological treatments which show remarkable clinical efficacy in various malignant tumours, including melanoma and lung cancer.1 ICIs act by enhancing the patient’s immune system to fight cancer. This action is possible because these monoclonal antibodies (Abs) have the ability to block intrinsic downregulators of immunity. In particular, ipilimumab inhibits the cytotoxic T-lymphocyte antigen 4 (CTLA4), nivolumab and pembrolizumab block the programmed cell death 1 (PD-1) pathway, while atezolizumab, avelumab and durvalumab act on the PD-1 ligand.1 By increasing the activity of the immune system, ICIs may trigger a number of immune-related side effects, which can involve any organ or system, including the nervous system.1 Moreover, it has been shown, in both experimental and clinical settings, that ICIs can induce paraneoplastic neurological syndromes (PNS).2 3 Overall, the most common neurological complications of immunotherapy involve the peripheral nervous system, and the characteristics of ICI-induced neuropathies,4 myasthenia gravis5 and myositis6 are now well defined. Conversely, central nervous system immune-related complications (CNS-ICI) are much rarer, and knowledge on how to diagnose and treat these conditions is limited.7–9 In particular, details on semiology, neuroimaging findings, Ab prevalence and response to treatment are lacking for CNS-ICI phenotypes. Moreover, although international recommendations contraindicate ICI readministration following CNS-ICI,10 the effect of ICI rechallenge in this selected population remains to be clearly elucidated.
In this retrospective study, we describe the clinical spectrum, treatment and outcome of CNS-ICI.
Materials and methods
Patient selection
We searched the database of the French National Reference Center for Paraneoplastic Neurological Syndromes and Autoimmune Encephalitis (Lyon, France) for patients who developed CNS-ICI between 1 January 2015 and 31 October 2019. All patients underwent a comprehensive laboratory examination, including an initial assessment with immunohistochemistry (IHC) on rat brain sections, followed by a second confirmatory test represented by dot-blot analysis on recombinant proteins (Euroimmun, Lubeck, Germany and/or Ravo Diagnostika, Freiburg, Germany) and/or cell-based assays (CBA) (inhouse techniques) to assess the presence of neuronal Abs. Patients with neurological symptoms that were found to be related to cancer and its progression, including brain metastasis and carcinomatous meningitis, or complications of other treatments, were excluded. Clinical and ancillary data (laboratory, neuroradiological and oncological information) were extracted by retrospective review of the medical records. Follow-up, management and outcome were also recorded. Outcomes were assessed using the modified Rankin Scale (mRS) and the Common Terminology Criteria for Adverse Events (version 5.0). CNS-ICI phenotypes were classified a priori as follows: (1) limbic encephalitis: subacute onset of memory deficits, seizures or psychiatric symptoms, in association with cerebrospinal fluid (CSF) inflammatory alterations and/or selective involvement of the limbic system on brain MRI; (2) meningoencephalitis: combination of encephalopathy and clinical or MRI evidence of meningeal involvement, with compatible inflammatory CSF alterations; (3) cerebellitis: subacute onset of signs/symptoms of cerebellar dysfunction (including trunk and/or limbs ataxia, abnormal eye movements, dysarthria) of inflammatory aetiology; (4) basal ganglia encephalitis: prominent movement disorders in association with specific basal ganglia inflammatory changes on brain MRI; and (5) myelitis: symptoms/signs of neurological dysfunction in motor and sensory tracts on both sides of the spinal cord of inflammatory aetiology. Written consent was obtained from all patients.
Comparison between CNS-ICI and PN-ICI
We questioned whether the clinical and oncological features of patients with CNS-ICI were different from those of cases with ICI-triggered peripheral neuropathies (PN-ICI) reported in the literature. For retrieving the literature series, we searched PubMed for records published in the English language between 1 January 2010 and 31 October 2019, using the following search terms: ‘neuropathy’ or ‘neuronopathy’ or ‘Guillian-Barré syndrome’ and ‘immune checkpoint inhibitors’. In addition, the reference lists of all selected articles were perused to identify any articles missed.
Statistical analysis
Descriptive analysis is presented as frequencies and percentages for categorical variables and as median and range for continuous variables. Categorical data were analysed with the Fisher’s exact test (two-tailed). Statistical analyses were performed using IBM SPSS Statistics Software V.25.0. P values <0.05 were considered significant.
Results
We identified 19 patients with CNS-ICI (table 1). Most of them were male (14 of 19; 74%). The median age was 69 years (range: 32–80). The median delay between ICI introduction and onset of the neurological syndrome was 3 months (range: 1–15). Fourteen patients had distant organ metastasis at the time of ICI introduction (n=6 with brain metastases). When the neurological syndrome ensued, the patients with cerebral metastasis had stable or improved lesions on brain MRI, whereas the others showed no evidence of cancer dissemination in the CNS. In no case could the clinical syndrome be related to the presence of brain metastasis (see online supplementary table). No patients had history of neurological disorders. Seven non-neurological immune-related side effects of ICI additionally developed in five patients: colitis (n=2), hypophysitis (n=1), thyroiditis (n=1), arthritis (n=1), vitiligo (n=1) and thrombocytopaenia (n=1). All non-neurological adverse events developed after neurological ones, except hypophysitis which was concomitant with meningoencephalitis. Overall, 14 of 19 (74%) demonstrated objective cancer response after ICI treatment.
Supplemental material
Characteristics of patients with CNS-ICI
CNS complication phenotypes
CNS-ICI phenotypes were limbic encephalitis (n=8), meningoencephalitis (n=4), cerebellitis (n=4) and atypical syndromes (n=3). The latter group included isolated confusion (n=2) and polyradiculoneuritis associated with parkinsonism (n=1).
Limbic encephalitis (n=8)
Six of the patients with limbic encephalitis have been previously reported by our group,3 and two more cases have been observed since then. Clinical syndrome included altered mental status in five of eight (62%) patients, anterograde memory disturbances in four (50%), and seizures and psychiatric disorders in the same proportion (3 of 8; 37%). Additionally, three (37%) patients developed diencephalitis in the form of increased weight, loss of libido and narcolepsy-cataplexy. Brain MRI revealed bilateral mesial temporal lobe hypersignal in five of eight cases (62%; figure 1A–C), while the remaining three (37%) patients had an unremarkable MRI. CSF examination detected inflammatory alterations in six of eight cases (75%; table 1). Anti-Ma2 Abs were detected in the serum and CSF of seven of eight (87%) patients, while one (12%) patient had an atypical neuropil staining due to an unknown Ab. Overall, the patients had a median mRS score of 4 at disease peak (range: 3–5). Neurological treatment included ICI withdrawal and corticosteroid bolus in all patients. Additionally, four of eight (50%) patients received intravenous immunoglobulin (IVIG), one (12%) underwent plasma exchange and two (25%) were treated with second-line immunotherapy (rituximab). The median follow-up was 4.5 months (range: 1–13). Despite all these measures, four of eight (50%) patients died due to neurological involvement (all four with Ma2 Abs). Importantly, one patient who eventually died manifested central hypoventilation (‘Ondine’s curse’) in the weeks prior to death. One (12%) patient manifested clinical worsening after neurological treatment (mRS 3→4). Two (25%) patients showed stabilisation of symptoms (mRS score of 3 and 4, respectively), and only one (12%) patient clearly improved after treatment (mRS 5→3).

{kind=link}
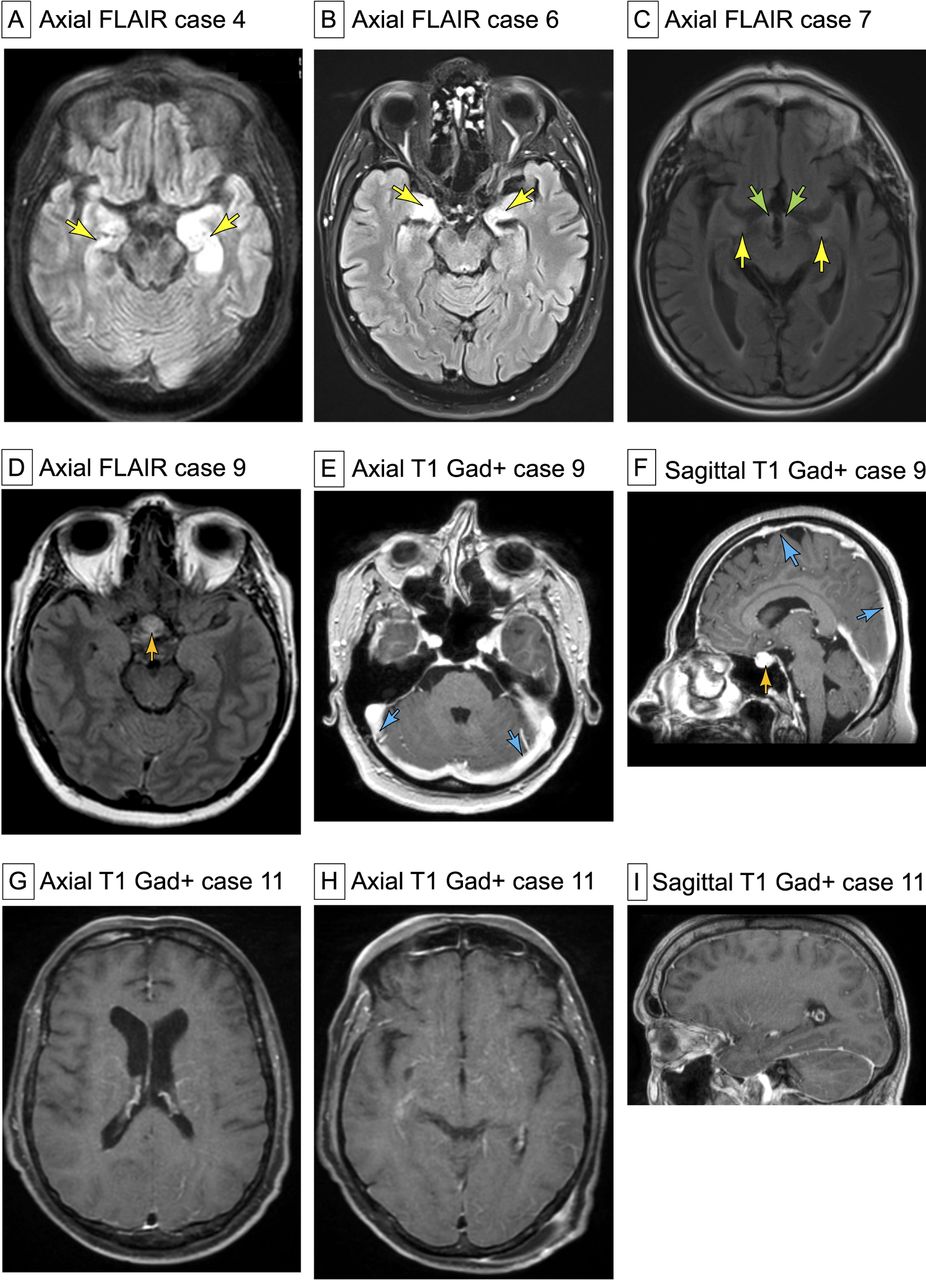
Brain MRI findings in patients with CNS-ICI. (A–C) Brain MRI findings (FLAIR sequences) in three patients with anti-Ma2 limbic encephalitis triggered by ICIs. Note the prominent limbic (A–C, yellow arrows) and diencephalic (C, green arrows) involvement. (D–F) Brain MRI findings in a patient with concomitant pachymeningitis and hypophysitis triggered by ICIs. Axial FLAIR sequence showing symmetric enlargement of the pituitary gland (D, orange arrow). Postgadolinium images revealed intense gadolinium enhancement of the hypophysis (F, orange arrow). Concomitantly, a diffuse, gadolinium-enhancing, dural thickening can be observed (E–F, blue arrows). (G–I) Brain MRI of a patient with GFAP-associated meningoencephalitis reveals a prominent radial pattern of periventricular postgadolinium enhancement (G and H, T1 axial; I, T1 sagittal). Initially, the patient was misdiagnosed as having carcinomatous meningitis. CNS-ICI, central nervous system immune-related complications; FLAIR, fluid attenuated inversion recovery; GFAP, glial fibrillar acidic protein; ICI, immune checkpoint inhibitors.
Meningoencephalitis (n=4)
Meningoencephalitis presented with altered mental status in three of four (75%) patients, fever in three (75%), anterograde memory disturbances in three (75%) and headache in one (25%). Additionally, two patients presented involvement of the peripheral nervous system (one sensorimotor peripheral neuropathy and one sensory neuronopathy). Abs against the glial fibrillar acidic protein (GFAP) were detected in the CSF of two (50%) patients, one with non-small cell lung cancer (NSCLC) and one with kidney cancer. One (25%) patient showed an atypical neuropil staining, and in another case (25%) screening was negative for known Abs. Brain MRI was in favour of pachymeningitis in one patient, where concomitant autoimmune hypophysitis was also detected (figure 1D–F). In another case (positive for GFAP Ab), the MRI showed diffuse perivascular postgadolinium enhancement (figure 1G–I). CSF analysis revealed inflammatory changes in all cases (table 1). A comprehensive microbiological screening and search for malignant cells was performed in the CSF in all cases, with negative results. The median mRS score was 5 (range: 3–5). All cases necessitated ICI withdrawal and treatment with corticosteroid bolus. After a median follow-up of 14 months, three (75%) patients were still alive and one (25%) died due to oncological complications. Among the three patients who survived, two showed clear neurological improvement after treatment (mRS 3→0 and mRS 5→2). One patient who was severely affected achieved stabilisation of symptoms (mRS 5→5).
Cerebellitis (n=4)
All patients with cerebellitis but one presented with an isolated cerebellar syndrome; the remaining patient had additional cranial nerve involvement (diplopia and vestibulocochlear dysfunction). The cerebellar disorder manifested as gait ataxia in all four (100%) patients, with additional limb ataxia in one patient and opsoclonus-myoclonus syndrome (OMS) in another (see online supplementary videos 1 and 2). The patients were investigated using brain MRI, which was normal in three (75%) of the cases, while mild cerebellar atrophy was observed in one (25%). CSF was abnormal in all cases (table 1). The antibody search revealed an anti-Hu positivity in the patient with small cell lung cancer (SCLC) treated with atezolizumab who presented with gait ataxia, rotatory nystagmus and nausea. Atypical neuropil staining was observed on immunofluorescence in the other two cases. The patient with seronegative OMS also developed severe inflammatory arthritis. The median mRS score at disease peak was 4 (range: 4–5). Treatment included ICI withdrawal and corticosteroid bolus in all patients; the median follow-up was 4.5 months (range: 2–23). The patient with Hu-PNS was additionally treated with IVIG, which led to a modest clinical improvement (mRS 5→4). The Ab-negative cases of cerebellitis showed a dramatic response to treatment: two completely recovered (mRS: 0) and one recovered with mild remaining symptoms, without disability (mRS: 1). In one seronegative case who achieved complete neurological recovery, a rechallenge with the drug (nivolumab) was attempted, without further relapses, and the patient obtained complete cancer remission (Hodgkin’s lymphoma), which was maintained after 23 months of follow-up.
Supplementary video
Supplementary video
Atypical syndromes (n=3)
One patient under treatment with ipilimumab-nivolumab combination for melanoma developed subacutely acroparesthesia and proprioceptive ataxia 4 months after ICI initiation. Areflexia and distal motor weakness were observed on examination (mRS: 4). Electromyography was in favour of a polyradiculoneuritis and CSF examination showed pleocytosis. The patient was treated with corticosteroids with gradual clinical improvement. In the following days, symmetric rigidity, postural and action tremor, hypomimia, and micrographia ensued. A diagnosis of parkinsonism was made and a therapeutic attempt with levodopa was started, with clinical improvement. Abs against contactin-associated protein-like 2 (CASPR2) were detected in the serum (1/100 dilution, titre not available). No CSF sample was available in our centre for Ab testing. In close temporal succession, the patient later manifested autoimmune thyroiditis and colitis, and concomitant reduction of the size of all metastatic lesions. Corticosteroid treatment led to improvement of symptoms, but a mild parkinsonian syndrome persisted over time. For this reason, a dopamine transporter scan (DaTSCAN) was performed, which demonstrated the presence of a dopaminergic deficit. A rechallenge of nivolumab was attempted without further autoimmune relapses. At last follow-up, 19 months after onset, the patient still had good motor status under levodopa treatment (mRS: 1).
The other two patients developed isolated confusion. One had concomitant NSCLC and rectal cancer under treatment with nivolumab. CSF analysis found pleocytosis (26 cells/mm3), normal protein content and negative Oligoclonal band (OCB) testing. Brain MRI demonstrated reduction in size of a known occipital metastasis. After a comprehensive diagnostic screening, no structural, metabolic, infectious or neoplastic aetiology was documented. Electroencephalogram (EEG) did not show epileptic discharges. The patient spontaneously improved (final mRS: 2). Nivolumab was restarted and no further confusional episodes were described. The second patient manifested subacute onset of confusion 10 months after pembrolizumab initiation for bladder cancer. Mini-Mental State Examination was 14 out of 30, while the patient was previously described as cognitively normal. Brain MRI did not reveal inflammatory alterations, CSF analysis was normal, but an atypical staining was observed on IHC. Corticosteroid treatment (2 mg/kg/day) permitted a rapid (48 hours) neurological recovery. ICI therapy was interrupted. A severe autoimmune colitis subsequently developed requiring additional treatment with infliximab. Despite this treatment, the patient died 2 months later.
Comparison between CNS-ICI and PN-ICI
A comparison between CNS-ICI (n=19, present series) and PN-ICI (n=77, literature series) is presented in table 2. NSCLC was significantly more frequent in patients with CNS-ICI (p<0.01), while melanoma was more common in patients with PN-ICI (p<0.01). In addition, anti-CTLA4 Ab as a single agent was more frequently reported in PN-ICI (p=0.01). Conversely, CNS-ICI cases were more frequently Ab-positive than PN-ICI (p<0.01). Moreover, CNS-ICI cases showed a strong trend towards poorer outcome (p=0.053).
Comparison between CNS-ICI and PN-ICI
Discussion
In this study, we identified three main clinical patterns (limbic encephalitis, meningoencephalitis and cerebellitis) and another subset of patients with atypical phenotypes characterising CNS complications of ICIs. Moreover, we observed that patients with CNS involvement (1) commonly have an underlying NSCLC, (2) are often Ab-positive and (3) typically show a severe disease, exhibiting a high fatality rate. Importantly, these characteristics are different from those of patients with ICI-induced peripheral neuropathy reported in the literature, in whom the large majority have associated melanoma, very few cases show associated Abs, and the fatality rate is low. The possibility of CNS inflammatory involvement related to ICI in patients with known brain metastases (as it is the case in approximately one-third of the present series) renders this diagnosis particularly challenging. These factors, as well as the wide range of novel Ab specificities recently discovered and the opportunity for effective treatment even in patients with severe disease, highlight the importance of a timely neurology consultation and eventually a referral to specialised autoimmune neurology centres for the management of these patients.
Limbic encephalitis was the most frequent CNS complication observed herein and was commonly associated with anti-Ma2 Abs. Indeed, six of these patients were previously reported by our group, in a study that demonstrated an increased frequency of Ma2-PNS following the large-scale utilisation of ICIs in France.3 Four additional patients with Ma2 Abs were reported in the literature, raising further concern.11–14 In our experience, the presence of anti-Ma2 Abs in patients with ICI-triggered limbic encephalitis carries a poor outcome (approximately half of the patients died due to neurological involvement). To this regard, clinicians should consider that the detection of onconeural Abs using commercial immunodots alone is limited by a high rate of false positive results (eg, we recently demonstrated that only 16.6% of Ma2-PNS positive cases are later confirmed by CBA and IHC).15 Hence, confirmatory tests at reference centres are needed to minimise misdiagnosis. Besides Ma2 autoimmunity, 12 cases of Ab-positive encephalitis associated with ICIs have been published so far. In particular, four had Hu,16–19 three glutamic acid decarboxylase (GAD65),20–22 two phosphodiesterase 10A (PDE10A),23 two N-methyl-D-aspartate receptor24 25 and one CASPR2 Abs.26 Overall, most of the patients with Abs other than Ma2 improved with first-line18 20 23 26 or second-line immunotherapies.19 21 24 25 Two died of cancer complications.16 22 Two (one Hu and one PDE10A) died due to neurological syndrome.17 23
Approximately one-fifth of patients with CNS-ICI developed meningoencephalitis. Two of them showed GFAP autoantibody positivity. This finding further underscores the role of dysregulated T-cell function in the pathogenesis of GFAP astrocytopathy.27 It is relevant to observe that GFAP meningoencephalitis poses a diagnostic challenge in patients with advanced cancer, since the clinical presentation and neuroimaging findings may direct the physician in making a misdiagnosis of carcinomatous meningitis (figure 1). Nevertheless, the correct differential diagnosis in this context is crucial, because a divergent management approach is expected in cases with ICI-induced meningoencephalopathy (where ICI withdrawal is recommended)9 versus carcinomatous meningitis (in which ICI therapy might be beneficial).28
Another one-fifth of our series of patients with CNS-ICI developed cerebellitis. Their associated cancer and ICI spectrum were different compared with the other groups, including non-solid cancers (eg, Hodgkin’s lymphoma) and less frequently adopted ICIs (atezolizumab and durvalumab). The only patient with SCLC had Hu Abs, while in the others no known Abs were identified. The response to treatment was excellent for the seronegative cases, while the patient with Hu Abs had a modest response to IVIG. Two patients with cerebellitis triggered by ICIs have been previously reported.29 30 One of them with Hodgkin’s lymphoma showed complete recovery following corticosteroid treatment, closely resembling our experience in the patient with the same type of cancer.
The fourth group comprised patients with atypical neurological manifestations: transient episodes of confusion and a complex syndrome characterised by polyradiculoneuritis followed by parkinsonism. While it is known that many factors can herald the appearance of confusion in patients with advanced cancer, no alternative aetiology was found, and the symptoms promptly responded to corticosteroid treatment in one case. Regarding the patient who developed parkinsonism, several factors suggest that this syndrome is related to ICI. First, anti-CASPR2 Abs were found in the patient’s serum, and parkinsonism is a rare but already reported manifestation of CASPR2 autoimmunity.31 Second, in close temporal association, the patients developed other immune-related adverse events of ICIs, also showing a favourable cancer response to immunotherapy. Third, the onset of parkinsonism was rapid and symmetric, which are highly atypical elements for a diagnosis of idiopathic Parkinson’s disease. Intriguingly, a similar patient with parkinsonism after anti-PD-1 and anti-CTLA4 combination treatment for melanoma was previously reported.32
We did not observe other CNS phenotypes that were rarely reported in the literature as complications of ICIs (eg, myelitis).33 We speculate that this will emerge in the future as a possible fourth clinical phenotype when larger CNS-ICI cohorts will be examined.
A direct role of brain metastases and/or carcinomatous meningitis in determining the neurological syndrome was excluded in all patients. In particular, among the six patients with concurrent brain metastases, the neoplastic lesions were in regression or stable at CNS-ICI onset. Moreover, four of them had an associated well-characterised neuronal Ab with compatible clinical syndrome (eg, diencephalitis and limbic encephalitis in anti-Ma2 syndrome).3 34–36
The role of auto-Abs into the pathogenesis of neurological adverse events of ICIs is not fully elucidated, but a number of studies suggest that they can be regarded as possible biomarkers of such complications.3 19 24 In some patients, ICI treatment may unmask a PNS with possibly pre-existing cancer immunity (as shown in cases where the retrospective analysis of Abs in samples taken prior to ICI initiation yielded positive results).3 In other patients, a new-onset autoimmune disorder triggered by ICIs seems the most likely explanation. Another proposed mechanism for ICI-triggered limbic encephalitis involves the clonal Epstein-Barr virus (EBV)-like memory CD4+ T-cell activation.37 Intriguingly, the appearance of immune-related complication seems to correlate with efficacy of cancer immunotherapy.38 In addition, circulating neuronal auto-Abs in patients with cancer are associated with limited disease and better overall survival.39
In three patients of this series (none of whom had encephalitis), a rechallenge of ICI therapy was attempted after the onset of immune-related CNS complications. No patient exhibited further neurological relapses, although longer follow-up is needed to establish firm conclusions on the safety of ICI reintroduction.
Finally, we and others4 8 40 have observed a higher incidence of neurological side effects in male patients. We hypothesise that some variables with an unbalanced sex ratio could have a role. A smoking history, for example, can affect both the therapeutic responses and toxicity risk by determining an ‘inflamed phenotype’,41 and the incidence of smoking is higher in men than in women all over the world.42 Second, a slight difference in the epidemiology of the cancers in which ICIs are used can also play a role.
The present study is limited by its retrospective nature and possibly by a referral bias towards more severe cases. Nevertheless, it represents the largest cohort to date of CNS complications of ICI therapy.
In conclusion, we report the clinical spectrum and response to treatment in 19 patients suffering CNS immune-related adverse events of ICI therapy, defining three phenotypes, each with distinct clinical presentation, immunological characteristics and outcome.
Importantly, CNS complications can develop in patients with known brain metastases, or with neuroimaging findings erroneously suggestive of carcinomatous meningitis, as in GFAP meningoencephalitis, making this diagnosis particularly challenging. Intriguingly, the cancer and ICI associations appear different from those of patients with ICI-induced peripheral neuropathies.
Acknowledgments
We thank NeuroBioTec Hospices Civils de Lyon BRC (France, AC2013-1867, NFS96-900) for banking sera and CSF samples. We gratefully acknowledge Véréna Landel (Direction de la Recherche Clinique, Hospices Civils de Lyon) for English language editing.
References
Footnotes
Contributors Study concept and design: AV, JH. Acquisition of data: AV, SM-C, BJ, GP, VR, CM, AMC, EC, FS, AL, FD, JH. Analysis and interpretation of data: AV, SM-C, BJ, GP, VR, CM, AMC, EC, FS, AL, FD, JH. Drafting of the manuscript: AV. Critical revision of the manuscript for important intellectual content: AV, SM-C, BJ, GP, VR, CM, AMC, EC, FS, AL, FD, JH. Study supervision: JH.
Funding This study is supported by research grants from ANR (ANR-14-CE15-0001- MECANO) and FRM (Fondation pour la recherche médicale, DQ20170336751). This work has been developed within the BETPSY project, which is supported by a public grant overseen by the French National Research Agency (ANR), as part of the second 'Investissements d'Avenir' programme (reference ANR-18-RHUS-0012).
Competing interests AV reported receiving a fellowship grant from the European Academy of Neurology (EAN). No other disclosures were reported.
Patient consent for publication Obtained.
Ethics approval The study was approved by the Institutional Review Board of the University Claude Bernard Lyon 1 and Hospices Civils de Lyon.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data are available upon reasonable request. All data relevant to the study are included in the article or uploaded as supplementary information. Patient-related data will be shared upon request from any qualified investigator, maintaining anonymisation of the individual patients.
Linked Articles
- Editorial commentary