Article Text

Abstract
Background: There is evidence to support both the use of intravenous methylprednisolone (IVMP) in multiple sclerosis (MS) relapse and physiotherapy in the management of MS, but no studies have investigated the combination of steroids and rehabilitation together.
Objectives: To evaluate the benefits of IVMP with planned, comprehensive multidisciplinary team (MDT) care compared to IVMP with standard care.
Methods: In this randomised controlled trial, patients confirmed to have had a definite MS relapse severe enough to warrant IVMP (1 g daily for three days) were randomised to two groups. The control group was managed according to the standard ward routine; the treatment group received planned coordinated multidisciplinary team assessment and treatment. Baseline assessments, including demographics and Expanded Disability Status Scale (EDSS) were carried out on both groups. The primary outcome measures were Guy’s Neurological Disability Scale (GNDS), and Amended Motor Club Assessment (AMCA). The secondary measures were the Barthel Index (BI), Human Activity Profile (HAP), and Short Form Item 36 Health Survey (SF-36). All measures have published data on reliability and validity. Measures were administered at one and three months.
Results: Forty subjects, including 27 females, completed data collection. There were no significant differences between the two groups at baseline. Results showed statistically significant differences in GNDS (p = 0.03), AMCA (p = 0.03), HAPM (p < 0.01), HAPA (p = 0.02), and BI (p = 0.02) at three months in favour of planned MDT care.
Conclusion: This study indicates that combining steroids with planned MDT care is superior to administering them in a standard neurology or day ward setting. Further research is necessary in order to confirm this finding.
- multiple sclerosis
- rehabilitation
- methylprednisolone
- physiotherapy
- AMCA, Amended Motor Club Assessment
- BI, Barthel Index
- EDSS, Expanded Disability Status Scale
- GNDS, Guy’s Neurological Disability Scale
- HAP, Human Activity Profile
- IVMP, intravenous methylprednisolone
- MDT, multidisciplinary team
- MS, multiple sclerosis
- OT, occupational therapy
- PT, physiotherapy
- SF-36, Short Form 36 Item Health Survey
Statistics from Altmetric.com
- AMCA, Amended Motor Club Assessment
- BI, Barthel Index
- EDSS, Expanded Disability Status Scale
- GNDS, Guy’s Neurological Disability Scale
- HAP, Human Activity Profile
- IVMP, intravenous methylprednisolone
- MDT, multidisciplinary team
- MS, multiple sclerosis
- OT, occupational therapy
- PT, physiotherapy
- SF-36, Short Form 36 Item Health Survey
Multiple sclerosis (MS) is the most common cause of progressive neurological disability in young adults in the United Kingdom.1 The course of MS varies, but four patterns have emerged, as described by Lublin and Reingold.2 These subtypes are distinguished by the time course of relapse and progression.3 Current medical management falls into three broad categories: disease modifying therapies, symptom management, and relapse management. The mainstay of relapse management is steroid therapy, usually intravenous methylprednisolone (IVMP).
The use of steroids in MS has been advocated since the 1940s and 1950s.4 Their exact mode of action is unclear, but it is thought that they act to reverse breakdown of the blood-brain barrier,5,6 thus accelerating recovery from the relapse.1 There is extensive literature evaluating the benefits of steroids. The Cochrane review of corticosteroids for MS relapse7 determined the efficacy and safety of steroids in reducing the morbidity from MS. Six trials covering 377 subjects experiencing relapses irrespective of their disease course indicated that intravenous administration may be more efficacious than oral administration of methylprednisolone.7 A study on views of British neurologists on steroid administration suggested that, in the UK, delivery of IVMP varied in dose, mode, and venue for treatment.8
It is also believed that physical therapy, directed at normalising tone and improving movement and posture9,10 during steroid therapy and the acute period afterwards, facilitates improved longer term functional outcome. Anecdotal evidence suggests that many patients, due to the timing of their admission for IVMP, do not receive adequate rehabilitation or education regarding appropriate care after discharge.
Studies conducted on the benefits of physiotherapy (PT) and occupational therapy (OT)11–15 generally have shown therapy to be of benefit to MS patients. Rehabilitation addresses many issues and should be viewed as an opportunity for gains to be made in various aspects of the person’s life, encompassing both physical and emotional aspects. Recent studies16,17 have shown that inpatient rehabilitation by a multidisciplinary team (MDT) is beneficial for people with MS and that some benefits are sustained for periods of up to six months in the community. Further studies also found that limited periods of rehabilitation helped in reducing disability and handicap in the short term.18,19 Patients being treated for relapse should be considered for rehabilitation, but none of these studies included relapsing patients and none of the studies covered in the Cochrane review included any rehabilitation element in their design.
A study conducted recently concluded that other rehabilitative interventions should be considered alongside steroid treatment.20 The results of this study indicated that although impairment and disability did improve after steroid treatment, perceived health status only slightly improved. The authors concluded that rehabilitation intervention with steroid treatment may be more effective in improving subjective disease state and suggested a randomised study should address this issue.
In view of this lack of clinical and published evidence, the aim of this randomised trial was to evaluate the benefits of receiving a combination of IVMP and focused MDT management of relapse, compare to IVMP alone. The experimental hypothesis was that steroid therapy for MS patients in relapse combined with focused multidisciplinary team care was more beneficial than steroid therapy alone.
METHODS
Patients and protocol
This was conducted as a randomised controlled trial. Neurologists identified eligible patients, through neurology or MS clinics at the Walton Centre for Neurology and Neurosurgery and satellite clinics. Subjects identified as having a confirmed diagnosis of MS and a relapse requiring admission as either day case or inpatient, for treatment with a three day course of IVMP 1 g/day were included. Block randomisation using blocks of four subjects in a different-subject design was followed. Patients were randomly allocated to treatment or control according to the randomisation list and informed of their study group. Written informed consent was obtained, as was local ethical approval for the study.
Control patients received the equivalent of the current standard ward routine for IVMP management, including three days IVMP, commencing on any weekday. Referral to other disciplines such as general neurological physiotherapy and occupational therapy were addressed within available resources, and patients could be referred for subsequent outpatient therapy if this was deemed appropriate and the service was available in their area.
Treatment patients received a planned, multidisciplinary team assessment, including three days IVMP. All members of the MDT (mainly the MS team members) were aware of this group’s admission beforehand, allowing allocation of assessment time. Treatment depended on goals set during the initial assessments. Advice was given for continuing self management after discharge and if appropriate, referral to other agencies on discharge was arranged. Therapy treatment for both groups was not standardised as symptom presentation varied and therapy was patient focused to meet subjects’ needs at the time. An array of interventions was offered by the multidisciplinary team, ranging from health promotion advice for people with mild disability to passive stretching exercises taught to carers for subjects with more severe disability, or bladder management techniques for those with continence issues.
Assessments
All outcome measures were completed on admission, at one month and three months after the first day of IVMP. All assessments were conducted in the physiotherapy department of the study centre. Other data such as demographic information, baseline Expanded Disability Status Scale (EDSS), number of therapy contacts, duration of therapy sessions, and the number of subjects referred on to other agencies on discharge were collected.
The primary outcome measures used were the Guy’s Neurological Disability Scale (GNDS),21 a questionnaire in which the subject replies yes or no to a series of symptom related questions; and the Amended Motor Club Assessment (AMCA),22 which was assessed by the research physiotherapist. At the beginning of the study it was decided by review of the available literature not to use the upper limb section of the AMCA as it had been shown to have a ceiling effect in an MS population.22 The secondary measures were all self report and comprised the Barthel Index (BI),23 the Human Activity Profile (HAP), which comprises a maximum score and adjusted score domain,24 and the Short Form 36 Item Health Survey (SF-36)25 (see table 1). Because of the nature of the study, neither the patients nor the assessing therapist could be blinded; however, only the AMCA was not self reported by the patient. Due to staff mix within the service, the assessing therapist was also the treating therapist. Levels of accepted clinical significance for each measure were established via a pilot study26 and analysis of previously published data27; table 1 indicates this level where available.
Outcome measures scoring
Statistical methods
All data was entered onto a database on SPSS version 9.0 for Windows. It was established, with statistical advice, that any study effect would be shown at three months compared to baseline; therefore analysis was conducted on this change score data. Initial statistical analysis involved a Schapiro-Wilks test for normality of data. Only the GNDS data were of normal distribution and were tested parametrically (univariate analysis of variance). The AMCA and the secondary measures data were tested non-parametrically (Mann-Whitney test). Other tests completed included establishing effect size of the GNDS and clinical significance of each measure.
RESULTS
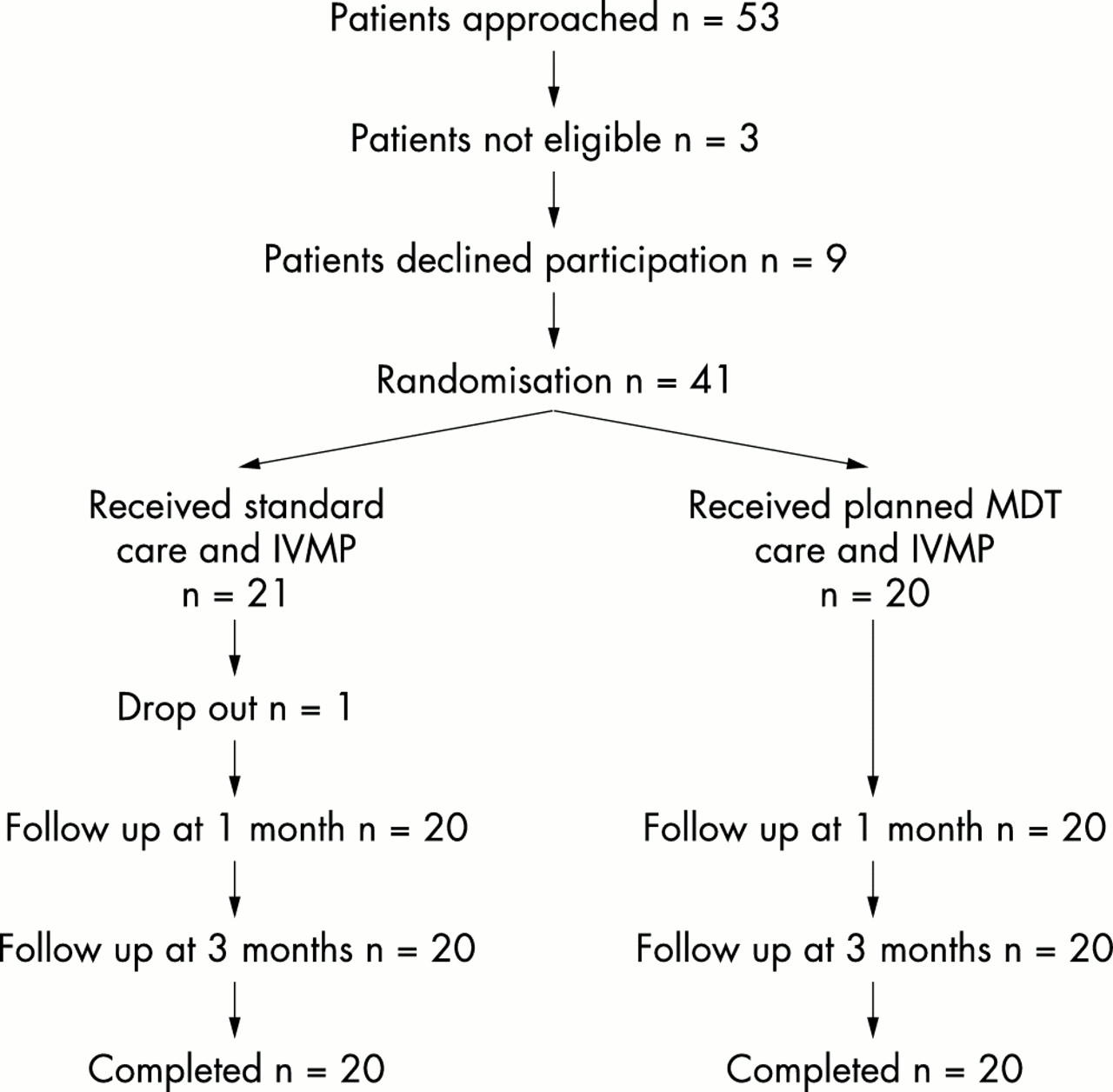
Between September 1999 and February 2001, 53 patients were referred for the study. Of these, three were not eligible, as they were not in a definite relapse. Nine further subjects declined participation for various reasons, including the distance to travel for the assessments and prior commitments. In total 41 patients were recruited to the study. Following baseline measurement one subject dropped out of the study for personal reasons. Forty subjects (20 treatment, 20 control) therefore completed data collection to three months and this data is reported (see fig 1).
{kind=link}
Participant flowchart.
Analysis revealed that the cohort was representative of the relapsing MS population in terms of gender, time since diagnosis, and disability level. Twenty seven females were recruited. Mean time since diagnosis was 6.4 years (range 0–24.1 years). Mean EDSS at the time of presenting with relapse was 5.25 (range 2–8). Further analysis established that there were no significant differences between the two groups. Table 2 describes the groups at baseline.
Baseline results—treatment versus control
Analyses of baseline mean score data for the primary measures revealed that the groups had no statistically significant differences in level of disability. Table 3 shows the mean score for the primary measures over the study period.
Mean scores (SD) for all measures
The difference in mean change score from baseline to three months between treatment and control groups was established and statistically tested with a 95% confidence interval. The GNDS and AMCA both showed a significance of p < 0.05. Table 4 shows the results. Effect size was established for the GNDS; it was −1.12 for the treatment group and −0.24 for the control group.
Change score from baseline to 3 months
Mean scores for both groups in the BI, HAP, and four domains of the SF-36 (Physical Function (PF), Social Function (SF), Role Emotional (RE), and Mental Health (MH)) followed a similar sustained improvement trend as those of the primary measures (see table 3). The other four domains (Role Physical (RP), Energy (E), Pain (P), and General Health (GH)) differed in that these mirrored those of the control group, presenting an improvement at one month but a decline at three months (see table 3).
Analysis of change score data for the secondary measures indicates significant differences of p < 0.05 in the HAP (both maximum score and adjusted score) and BI (see table 4). The SF-36 domains did not show any significance, although the Social Function domain did indicated a trend towards significance (p = 0.051) (see table 5).
Change score from baseline to 3 months: SF-36
Therapy intervention
The duration of therapy and specialist nursing intervention given to the groups differed according to the group protocols, as did the number of subjects referred to local services following steroid treatment. Referrals to other disciplines within the study centre also varied between groups. Table 6 summarises the differences between the groups.
Therapy data
Physiotherapy was the most common intervention administered following initial assessment and had the longest duration of treatment among those given. The physiotherapy intervention offered included provision of mobility aids; exercise programmes for stability, posture, balance, and fitness; health education; and assessment for provision of orthotics. Occupational therapy input included provision of equipment for the home; fatigue and stress management; provision of small aids; and referral to social services for more long term home assessments. Bladder management and advice on coping mechanisms were the main interventions offered by the specialist nurses.
DISCUSSION
This unique randomised controlled trial aimed to investigate the relative benefits of patients with MS relapse receiving a short course of focused, MDT care in combination with IVMP in comparison to standard care and IVMP. It was conducted to address a gap in knowledge identified in clinical practice and in current literature on MS management.20
Of the subjects screened, 80% entered the study and 97% of these completed the study. The sample included subjects treated both as inpatients and day case patients in order to reflect standard practice. This research attempted to establish whether access to enhanced therapy in combination with IVMP produced a preferable outcome. It was therefore important to ensure that standard care for the control group did not change from standard care prior to the trial commencing. Data on standard care were established during the pilot study.26 The referral rate, duration of treatment, and length of stay recorded for the control group indicated that standard care did not alter during the study period.
The distribution of gender, mean age at entry, mean time since diagnosis, and analysis of baseline outcome measure scores indicated no significant differences between the two study groups, suggesting randomisation had been effective.
Some of the improvement in both groups is likely to be spontaneous recovery. A further part of the recovery seen is a direct result of the IVMP itself, by reversing the changes to the blood-brain barrier and minimising symptom presentation and duration.28 This accounts for some of the initial improvement that is seen in the control subjects. However, the level of spontaneous and steroid related recovery should be comparable for both groups.
The main distinction accounting for the statistical differences in change score between groups is the therapy intervention. There were significant differences in the overall duration of therapy given to the two groups and distinct differences between groups, in favour of the treatment group, in the number of subjects seen by different disciplines. The therapy input given to the control group reflects current practice on the wards. The higher number of subjects referred on for further treatment in the intervention group is a reflection of the increased contact with therapists during admission. It was difficult within this study to ascertain whether the benefits obtained in the treatment group were accounted for by the acute intervention or the later community management. This study aimed to evaluate the opportunity to access a package of care, and the benefits are suggested to be due to a balance of a combination of acute and later stage rehabilitation reflected in the greater referral to local services in the treated group.
Statistical testing of the change score data from the primary measures showed a correlation between enhanced therapy intervention and an improvement in impairment and disability. The AMCA measures motor impairment.22 It is expected that change would be effected through therapy, with specific exercise and retraining of muscle activity.13 Changes in range of movement, motor control, and quality of movements become evident. This then has a direct influence on motor functions such as balance and transfers,12,13 both of which are assessed in the AMCA scoring.
Improvement in motor function at this level is expected to influence disability level. Improved range of movement, balance, and transfer techniques can reduce the dependency on others, promote acquisition of new or adapted skills, enhance independence, and facilitate improved management of other symptom areas through greater control of movement. The GNDS will reflect any changes achieved through PT, OT, MS nurse specialist, or orthoptic intervention.
The BI and HAP showed significant results in favour of the treatment group when mean change score and mean scores at baseline and three months were analysed. The domains of the SF-36 did not show statistical significance. It was anticipated that improving levels of disability, empowerment of the subjects, and increasing participation would reflect on the SF-36 domains. However, as the mean scores for several domains of the SF-36 showed greater improvement in the treatment than in the control group, there is still some benefit from the MDT intervention in altering health status.
Proving statistical significance does not always ensure that the changes will be clinically significant or relevant to the subjects involved. For each measure interpretation of the change score needs to be placed into a clinical context. Clinical significance can be estimated through assessing change score in comparison to a previously set significance level according to earlier data (see table 1) or via establishing effect sizes.29 Both of these methods were used to establish whether the changes were clinically significant in this patient group. The results highlighted in tables 4 and 6 further support the theory that enhanced therapy improves outcome after steroids by showing, in the primary measures and two of the secondary measures, that changes occurred which were likely to be clinically and functionally relevant to the subjects. The effect size for the GNDS was established. The results showed a large effect size for the treatment group and only a small effect size for the control group,28 which supports the suggestion that the intervention outcome is clinically relevant in this patient group.
In respect of the SF-36, despite no statistically significant difference, a clinically significant change score in six of the domains in the intervention group (the exceptions being the RE and GH domains) was established. However, only the SF and RP domains represented a clinically significant change score for the control subjects.
The main finding was that steroids and rehabilitation as a planned admission on an inpatient or daycase basis was superior to steroid treatment and standard care alone. There was a statistically significant difference between IVMP with standard care and IVMP with focused MDT care for the two primary measures (AMCA and GNDS) and some of the secondary measures (BI, HAP). This change exceeded predetermined evidence based levels for clinical significance for the GNDS, assessing disability, and the AMCA, assessing motor recovery. The SF-36 showed a trend in favour of the intervention.
The outcome measures were chosen to reflect the changes anticipated from the intervention—that is, alteration in motor function and disability level, and were hypothesis driven. Inability to incorporate assessor blinding into the design was a limitation of the trial. The GNDS score is dictated only by the subject responses and therefore is not influenced by the opinion of the person asking the question. The researcher scores the AMCA according to certain set criteria. Careful adherence to AMCA guidelines minimises but does not abolish intra-rater bias. A type I error could potentially have occurred in the AMCA analysis; however, as both the primary measures showed the same trend and the GNDS is self reported by the patient, it is unlikely. The secondary measures that are also all self report concur with this.
The SF-36 especially, but to a lesser degree the BI and AMCA, exhibit floor and ceiling effects. For the AMCA, the range of baseline scores for the study groups indicate a possible ceiling effect still to be present, as many patients were scoring in the higher end of the scoring range. The SF-36 has been shown previously30,31 to exhibit ceiling and floor effects, and the raw data for some subjects concurs with this in certain domains (RP and RE).
Three months was chosen for follow up as it was felt this would allow time for services in the community to be established, equipment required to be put in place, and for subjects to make gradual alterations to their lifestyle as a result of the advice and programme given. It was also felt that three months was soon enough after IVMP treatment that any significant results could be attributed to the intervention and not necessarily to other factors. However, it may be the case that this is still too short a period for any alteration in health related quality of life to be evident.
Conclusions
In conclusion this randomised controlled trial is the first to show that planned, focused MDT care during steroid treatment of MS relapse is beneficial. Changes in the study design would enhance the results. These include conducting the study as part of a multicentre trial (“standard care” and focused MDT care would need to be more standardised between centres); longer follow up period, such as up to 12 months, to allow potential changes in quality of life to be established and to determine the effects of the intervention over a long period; and use of a second, blinded assessor to establish AMCA score.
The findings suggest that introducing a problem focused team integrated approach to the steroid management of MS relapse in the acute setting, including access to appropriate levels of therapy, is of benefit to patients in terms of motor function, disability, and aspects of health related quality of life.
Acknowledgments
The authors would like to thank all the study participants; the staff at the Walton Centre for Neurology and Neurosurgery, Liverpool for assistance and support in administration of the study; and Serono Pharmaceuticals UK for the grant which supported the research therapists.
REFERENCES
Footnotes
-
Competing interests: none declared