Article Text

Abstract
Objectives Antiepileptic drug (AED) exposure during pregnancy increases the risk of major congenital malformations (MCMs). The magnitude of this risk varies by AED exposure. Here we provide updated results from the UK Epilepsy and Pregnancy Register of the risk of MCMs after monotherapy exposure to valproate, carbamazepine and lamotrigine.
Methods Fifteen-year prospective observational study from 1996 until 2012. The main outcome measure is the MCM rate.
Results Informative outcomes were available for 5206 cases. 1290 women were exposed to valproate monotherapy, 1718 to carbamazepine monotherapy and 2198 to lamotrigine monotherapy. The MCM risk with valproate monotherapy exposure in utero was 6.7% (95% CI 5.5% to 8.3%) compared with 2.6% with carbamazepine (95% CI 1.9% to 3.5%) and 2.3% with lamotrigine (95% CI 1.8% to 3.1%). A significant dose effect was seen with valproate (p=0.0006) and carbamazepine (p=0.03) exposed pregnancies. A non-significant trend towards higher MCM rate with increasing dose was found with lamotrigine. MCM rate for high-dose lamotrigine (>400 mg daily) was lower than the MCM rate for pregnancies exposed to <600 mg daily of valproate, but this was not significant (3.4% vs 5.0%, p=0.31).
Conclusions In utero exposure to valproate carries a significantly higher MCM risk than lamotrigine (p=0.0001) and carbamazepine (p=0.0001) monotherapy. In contrast to prior findings, high-dose lamotrigine was associated with fewer MCMs than all doses of valproate. While lamotrigine has a favourable profile compared with valproate for adverse pregnancy outcomes, the requirements for seizure control should not be overlooked.
- EPILEPSY
- ANTICONVULSANTS
Statistics from Altmetric.com
Introduction
Exposure to antiepileptic drugs (AEDs) during pregnancy increases the risk of major congenital malformations (MCMs) from a background risk of 1–2% to between 4% and 9%.1–4With the establishment of several epilepsy pregnancy registers over the last 15–20 years, the differential effect of exposure to individual AEDs during pregnancy is now widely recognised.4–6
In 2006, we published results showing an increased risk of MCMs with exposure to all AEDs, in particular valproate (MCM rate 6.2%). Initial data for lamotrigine and carbamazepine were reassuring (MCM rates 3.2% and 2.2%, respectively).4 Similar results have been observed by other pregnancy registries, with the North American AED Pregnancy Registry5 and the International Registry of Antiepileptic Drugs and Pregnancy (EURAP)6 also confirming high MCM rates for valproate monotherapy (9.3% and 9.7%, respectively) and lower rates for lamotrigine (2.0% and 2.9%, respectively) and carbamazepine (3.0% and 5.6%, respectively). The International Lamotrigine Pregnancy Registry also published data suggesting low risk for MCMs in lamotrigine-exposed pregnancies (MCM rate 2.2%).7
Strong evidence now exists that AED total daily dose is also an important factor in determining the magnitude of risk for MCMs. We previously found a dose–response for all three drugs, with exposure to higher doses being associated with an increase in MCM rates. However, this was only statistically significant for lamotrigine (p=0.005) and not for carbamazepine or valproate.4 Data from the North American AED Pregnancy Registry have also shown a trend for increasing risk for MCMs with increasing valproate dose, but no such trend was seen for other AEDs.5 However, data from EURAP suggested that MCM risk increased in a dose-dependent manner with all three of these drugs, as well as phenobarbital.6
Together with recently published data on the effects of valproate on neurodevelopment, IQ8 and the increased incidence of autistic spectrum disorders,9 which also seem to be dose-related,8 these data have led to a significant prescribing shift away from valproate in the UK.10 This prescribing shift may be partially responsible for the reduction in the total MCM rate in women with epilepsy (WWE) in the UK from 4.3% to 3.2% from 2000 to 2010.10
Although generally considered to be a safer drug, closer analysis of these data has raised concerns about MCM rates for lamotrigine taken in higher doses. In both the UK Epilepsy and Pregnancy Register (UKEPR)4 and EURAP6 studies, high doses of this drug (>200 mg daily and >300 mg daily, respectively) were associated with similar or higher MCM rates than low doses of valproate (<600 mg daily and <700 mg daily, respectively).
The UK and Ireland Epilepsy and Pregnancy Registers have now been collecting prospective registrations from WWE around the UK and Ireland from 1996 and have over 8000 completed registrations. Here we present results from the UK and Ireland Epilepsy and Pregnancy Registers in all pregnancies exposed to valproate, carbamazepine or lamotrigine in monotherapy in the first trimester between December 1996 and December 2012.
Methods
The UKEPR is a prospective, observational, registration and follow-up study that was set up in 1996 to determine the relative safety of all AEDs taken in pregnancy. The Irish Epilepsy and Pregnancy Register was set up in 2001 and joined the UKEPR in 2007. The two studies have the same methodology, both have been approved by national and regional ethical committees and obtain written informed consent from participants. Full details have been published previously.4
Suitable cases for this study were defined as WWE who became pregnant while taking valproate, carbamazepine or lamotrigine in monotherapy, and who were referred before the outcome of the pregnancy was known. Cases that are referred following antenatal diagnosis of a probable or definite MCM are excluded.
An MCM is defined as an abnormality of an essential embryonic structure requiring significant treatment and present at birth or discovered in the first 6 weeks of life, according to the definitions and lists of disorders in the EUROCAT registry.11 The timing of follow-up is at 3 months after birth.
Statistical analysis
Malformation rates were calculated as (total number of live births with a malformation)+(total number of pregnancy losses with a malformation)/(total number of live births)+(total number of pregnancy losses with a malformation). 95% CIs were calculated using the traditional method. χ2 test, Student t test, Fisher's exact test and ORs were used to compare characteristics between groups. Individual logistic regression analyses were performed using SPSS V.20, with the presence of an MCM as the dependent variable and AED, maternal age at birth, parity, family history of MCM, folic acid intake and gender of infant as the independent variables.
Results
Through December 2012, complete outcome data were available for 5206 pregnancies on valproate, carbamazepine or lamotrigine monotherapy. Of these 1290 were exposed to valproate, 1718 to carbamazepine and 2198 to lamotrigine. Two hundred and forty-eight pregnancies ended in a pregnancy loss, of which 17 had a MCM. The total MCM rate for all exposures was 3.5% (95% CI 3.0% to 4.0%). Pregnancy outcome details for all exposures and MCM rate for each drug are shown in table 1.
Cumulative outcomes for all pregnancies
The OR for having a child with an MCM on valproate monotherapy was 3.0 (95% CI 2.1 to 4.3, p<0.0001) compared with lamotrigine monotherapy and 2.7 (1.9 to 3.9, p<0.0001) compared with carbamazepine monotherapy. There was no significant difference in MCM risk in pregnancies exposed to carbamazepine compared with those on lamotrigine (OR 1.1, 95% CI 0.7 to 1.7, p=0.6).
The mean daily dose of valproate was significantly higher for infants with MCMs compared with those without (1031.2 mg compared with 897.9 mg, p=0.02). There was no significant difference in mean daily dose for cases with and without MCMs for lamotrigine (283.7 mg compared with 255.4 mg, p=0.20) or carbamazepine (712.8 mg compared with 629.5 mg, p=0.12). However, the MCM rate observed with each drug increased with increasing AED total daily dose (figure 1). This was statistically significant for low-dose valproate compared with high-dose valproate and low-dose carbamazepine compared with high-dose carbamazepine but not for low and high doses of lamotrigine (table 2).
MCM rate by dose for each AED

Major congenital malformation rate by drug dose.
The types of MCM observed with exposure to each drug were also different (table 3). All subtypes of MCM were observed more frequently in the valproate-exposed infants than in either of the other groups. This reached statistical significance for several subtypes. Neural tube defects and facial clefts were more likely to occur with exposure to valproate than with exposure to carbamazepine (OR 4.45; 95% CI 1.45 to 13.69, p=0.009) or lamotrigine (OR 11.29; 95% CI 2.54 to 50.12, p=0.0002). Hypospadias and genitourinary defects were also significantly more likely to occur with exposure to valproate than carbamazepine (OR 4.11; 95% CI 1.49 to 11.35, p=0.006) or lamotrigine (OR 2.60; 95% CI 1.16 to 5.81, p=0.03). Skeletal defects were more common with exposure to valproate than with exposure to carbamazepine (OR 3.41; 95% CI 1.07 to 10.91) or lamotrigine (OR 5.77; 95% CI 1.59 to 21.02, p=0.007). Cardiac defects were significantly more likely to occur with exposure to valproate than lamotrigine (OR 2.69; 95% CI 1.16 to 6.25, p=0.03), but no significant difference was observed between rates of cardiac defects between valproate and carbamazepine (OR 1.36; 95% CI 0.64 to 2.87).
Types of major congenital malformation with each AED
Folic acid supplementation had no significant effect on pregnancy outcome. Total MCM rate for women taking folic acid during the first trimester was 3.6% (95% CI 3.1 to 4.2) compared with 2.7% (95% CI 1.5 to 4.8) for those not taking folic acid (p=0.39). For individual AEDs, no difference in MCM rate was observed (p=0.23 for valproate, p=0.57 for carbamazepine and p=0.77 for lamotrigine). Among the women exposed to valproate, neural tube defects were slightly less frequent in those taking periconceptual folic acid compared with those taking folic acid only in the first trimester or not at all (0.9% compared with 1.2%), although this was not statistically significant (p=0.78).
Discussion
This large observational study confirms low overall rates of MCMs in women taking an AED in monotherapy during pregnancy, with over 96% of pregnancies resulting in a child without a MCM. In keeping with previously published data, the overall MCM rates seen with exposure to lamotrigine and carbamazepine were not that different from background, particularly when taken in doses of less than 400 mg/day and 1000 mg/day, respectively. This is likely to be of reassurance to WWE and those treating them. In contrast, significantly higher rates of MCMs were observed with valproate.
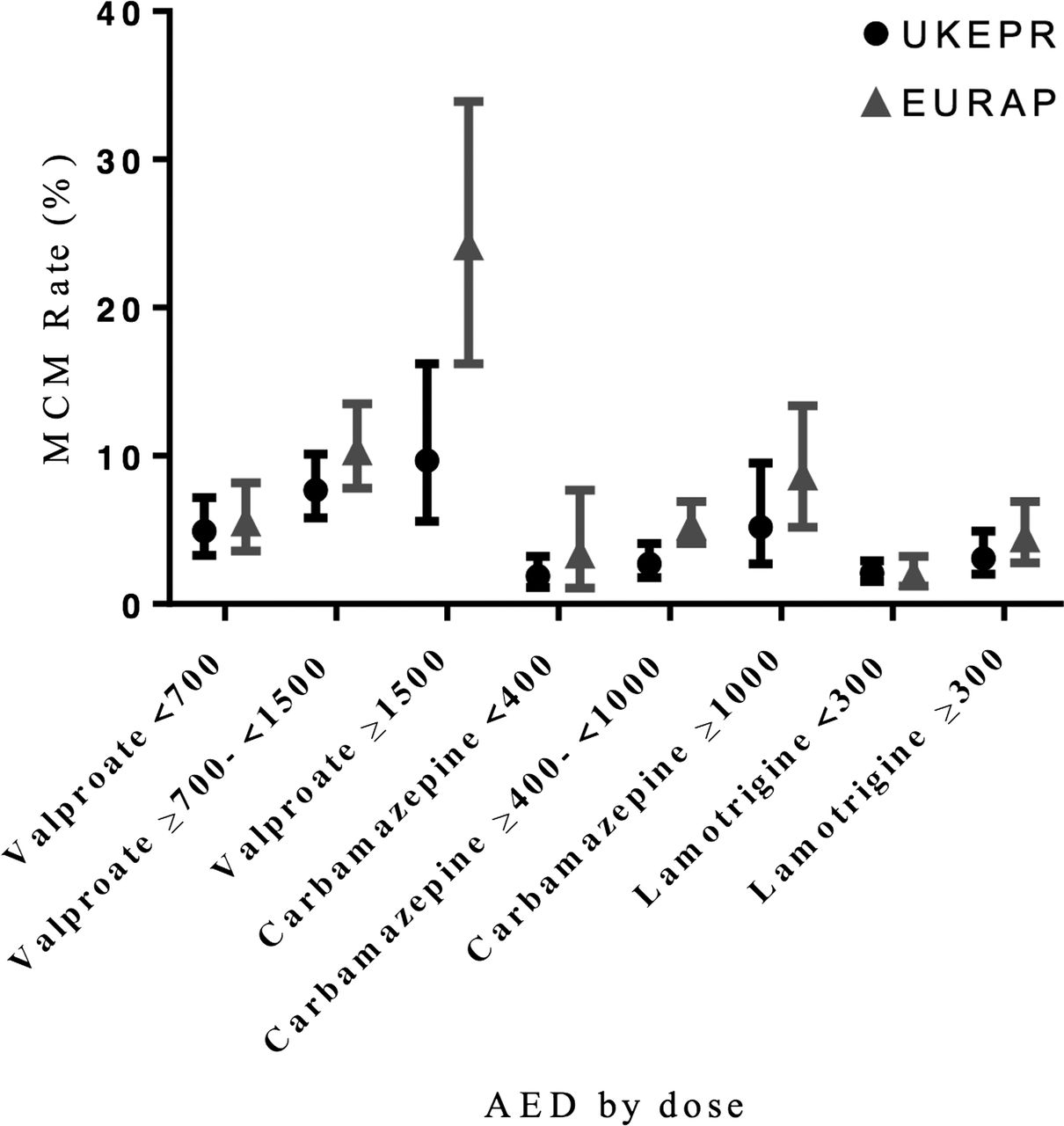
Our data confirm previously reported dose–responses for MCM rates for valproate and carbamazepine. The magnitude of the risk was smaller in our study for pregnancies exposed to the highest doses of valproate and carbamazepine compared with the EURAP cohort,6 where doses of valproate over 1500 mg daily were associated with an MCM rate of 24.2%, with an OR of 5.8 compared with those on <700 mg.6 In contrast, we found an MCM rate of 9.7% with 12 MCMs of 124 cases exposed to >1500 mg daily of valproate. These differences may reflect the small number of women taking high-dose valproate in both studies (124 in UKEPR, 99 in EURAP). For pregnancies exposed to high doses of carbamazepine (>1000 mg), in EURAP an MCM rate of 8.7% was observed, with an OR of 2.9 over lower doses (<400 mg). While the MCM rate seen with exposure to over 1000 mg daily in our results was lower (MCM rate 5.2%), the OR observed is similar (OR 2.7).
Although we also found a dose–response for MCMs with lamotrigine, the magnitude of this risk was smaller than we previously reported in fewer exposures. High-dose lamotrigine (>400 mg daily) was associated with a 1.3% increase in MCM risk over low doses (≤200 mg daily). Due to the minimal difference in MCM rates between low-dose and high-dose lamotrigine exposures, this was no longer statistically significant. High-dose lamotrigine was associated with fewer MCMs than low-dose valproate (≤600 mg daily; OR 0.67, 95% CI 0.31 to 1.46; p=0.31). Since the results did not achieve statistical significance, it is not possible at this time to confirm the trend towards fewer MCMs in favour of high-dose lamotrigine compared with low-dose valproate. This may change with continued recruitment and confirms the requirement for very large datasets to demonstrate differences in dose ranges between AEDs that are of practical use in managing WWE of childbearing age.
Although all epilepsy pregnancy registers have similar objectives and outcome measures, the results published by individual registries are not considered to be directly comparable due to differences in methodology. Major differences exist between the registries in their methods of enrolment, inclusion criteria, information obtained on confounding factors and methods and timing of follow-up.12 Variation in MCM rates observed with individual drugs between these registries is felt to be, at least in part, a result of these methodological differences. Table 4 displays MCM rate results from each of the major registries. Of note, similar trends are found across all registries, to include the risks for MCMs for individual AEDs stratified by dose (figure 3).
Comparative MCM results from the main epilepsy pregnancy registries

Comparison of major congenital malformation rate by antiepileptic drug dose in the UK Epilepsy and Pregnancy Register and EURAP.6
That the results from pregnancy registries have resulted in a prescribing shift away from valproate and carbamazepine in the UK is manifest from our data. In 2006, of women registering on one of these three drugs, 71.2% were on either valproate or carbamazepine. These drugs now represent only 57.8% of registrations, with only 528 women registering pregnancies exposed to valproate over the last 6 years, compared with 1514 for lamotrigine (figure 2 shows how the total number of registrations for each drug has changed over time.)

{kind=link}
{kind=link}
{kind=link}
Number of informative outcomes for each antiepileptic drug over time.
Rates of folic acid prescription did vary between AEDs, with fewer women on valproate taking folic acid compared with lamotrigine or carbamazepine. This is clearly of some concern bearing in mind this is the AED with the most concerning safety profile in pregnancy. Overall, in keeping with our prior findings13 and those from EURAP, the presence or absence of folic acid supplementation in the first trimester had no effect on MCM rates, although periconceptual folic acid consumption was associated with a non-significant reduction in rates of valproate-associated neural tube defects. Despite these findings, and in the absence of any harm, we continue to support the approach from the NICE14 and SIGN15 guidelines. Even though there is a lack of evidence of any effect on MCM rates, recent studies have suggested that folic acid supplementation may have a positive effect on neurodevelopment. A large cohort study from Norway has suggested reduced rates of autism with periconceptual folic acid supplementation,16 and the results from NEAD, which have shown protective effects of folic acid against reduced measures of cognitive development,8 would suggest that folic acid supplementation should be extended throughout pregnancy.
A suggested weakness of this study is the lack of inclusion of a control group. Although pregnancies should ideally occur without exposure to any medication, to include AEDs, we have chosen not to include these outcomes in this paper as complete withdrawal of treatment is not achievable for the majority of women with active epilepsy. Instead, the main choice faced in these circumstances is typically of which AED to choose, rather than whether to remain on any AED. To December 2012, the UKEPR had recruited 541 registrations to WWE on no AED, of which 13 resulted in a child with a MCM (MCM rate 2.4, 95% CI 1.4 to 4.1). No significant difference exists between the MCM rate for pregnancies on no AEDs and the MCM rates for all monotherapy exposures (p=0.18), carbamazepine-exposed pregnancies (p=0.81) or lamotrigine-exposed pregnancies (p=0.93). The MCM rate for valproate exposures was significantly higher than for pregnancies not exposed to an AED (OR 2.93, 95% CI 1.62 to 5.30; p=0.0002).
At present we estimate that the UK and Ireland Epilepsy and Pregnancy Registers receive registrations from approximately one-third of pregnancies to WWE in the UK and Ireland. The number of registrations received from different regions of the UK varies widely. Based on 2001 census data, the number of registrations from England and Wales has both averaged <1/100 000 population per year over the 16 years that the register has been recruiting (0.7/100 000 population/year and 0.6/100 000 population/year, respectively). This compares to 1.9/100 000 population/year for Scotland and 5.0/100 000 population/year for Northern Ireland. Increasing the proportion of women registering their pregnancies with the UK and Ireland Epilepsy and Pregnancy Registers would allow us to present more timely data on newer AEDs, as well as reducing the possibility of recruitment bias.
In conclusion, these data confirm that overall lamotrigine and carbamazepine can be considered safer alternatives to valproate during pregnancy and for lamotrigine, in particular, support its widespread use in WWE of childbearing age. In contrast to previous data, the MCM rate with high-dose lamotrigine was reassuring and even appeared to be lower than that for low-dose valproate. Taken together with recently published studies that have shown an increased risk of cognitive deficits and neurodevelopmental disorders for offspring exposed to valproate suggests that lamotrigine should be considered before valproate for women with unclassified or genetic epilepsy syndromes who are planning to become pregnant. It is however important to individually weigh up the requirements for seizure control versus the need to minimise teratogenicity, with it still being the case that for some women valproate may be the appropriate AED once other options, for which there are much less outcome data, have been considered.
References
Footnotes
-
Contributors EC: acquisition, analysis and interpretation of data, drafting article and final approval for publication. FK: acquisition, analysis and interpretation of data, revising manuscript and final approval for publication. AR, WHS, LP, PJM, ND, SJH and JC: study conception/design, revising manuscript and final approval for publication. BL: data acquisition, revising manuscript and final approval for publication. BI: data acquisition, revising manuscript and final approval for publication. JM: (guarantor of integrity of data) study conception/design, revising manuscript and final approval for publication. All authors fulfil the journal's criteria for authorship. There are no other parties who fulfil these criteria but have not been included.
-
Funding The UK Epilepsy and Pregnancy Register has received a research grant from the Epilepsy Research Foundation and a number of educational grants from pharmaceutical companies (Parke Davis, Glaxo Smith Kline, Eisai, Novartis, Sanofi-Aventis, Pfizer, Janssen-Cilag and UCB). Funders had no role in performing this research or preparing the manuscript.
-
Competing interests EC, FK and PJM report no competing interests. AR has received a grant from UCB for funding of a research nurse (2006–2009) and received small contributions from UCB, Glaxo Smith Kline, Eisai, Forth Medical, Cyberonics and Optima Medical to cover the costs of the UK Epilepsy Surgery Meeting in Glasgow in 2011. WHS has been invited to attend advisory board meetings for NAPP and Sanofi-Aventis within the last year. LP has received honoraria for presentations from UCB. BL has received honoraria for attending a UCB Pharma Irish Nurse Advisory Board meeting. BI has received sponsorship to attend meetings and honoraria for presentations from Eisai, UCB and Sanofi-Aventis. ND has received unrestricted educational support from UCB Pharma, Eisai, GSK, Janssen-Cilag and Pfizer for running of the Irish Epilepsy Pregnancy Register. He has also received honoraria for giving lectures from UCB, Eisai, GSK and Janssen-Cilag, and has served on Advisory Boards for UCB Pharma, Eisai, GSK and Janssen-Cilag. SJH has received sponsorship to attend meetings from Eisai, UCB and Glaxo Smith Kline. He has also received honoraria for presentations from Pfizer, Eisai and UCB. JC has received grants to undertake research and honoraria for giving lectures from UCB-Pharma, Sanofi-Synthelabo, Glaxo Smith Kline, Janssen-Cilag, Pfizer and Eisai. JM has received unrestricted educational grants from Eisai, Glaxo Smith Kline, Novartis, Sanofi-Aventis, Pfizer and UCB for the running of the UK Epilepsy and Pregnancy Register.
-
Ethics approval NRES Committee Northwest Haydock Park.
-
Provenance and peer review Not commissioned; externally peer reviewed.