Article Text

Abstract
Objective Antibodies against contactin-associated protein-like 2 (CASPR2-Abs) have been described in acquired neuromyotonia, limbic encephalitis (LE) and Morvan syndrome (MoS). However, it is unknown whether these constitute one sole spectrum of diseases with the same immunopathogenesis or three distinct entities with different mechanisms.
Methods A cluster analysis of neurological symptoms was performed in a retrospective cohort of 56 CASPR2-Abs patients. In parallel, immunological features and human leucocyte antigen (HLA) were studied.
Results Cluster analysis distinguished patients with predominant limbic symptoms (n=29/56) from those with peripheral nerve hyperexcitability (PNH; n=27/56). In the limbic-prominent group, limbic features were either isolated (LE/−; 18/56, 32.1%), or combined with extralimbic symptoms (LE/+; 11/56, 19.6%). Those with PNH were separated in one group with severe PNH and extralimbic involvement (PNH/+; 16/56, 28.6%), resembling historical MoS descriptions; and one group with milder and usually isolated PNH (PNH/−; 11/56, 19.6%). LE/− and LE/+ patients shared immunogenetic characteristics demonstrating a homogeneous entity. HLA-DRB1*11:01 was carried more frequently than in healthy controls only by patients with LE (94.1% vs 18.3%; p=1.3×10−10). Patients with LE also had serum titres (median 1:40 960) and rates of cerebrospinal fluid positivity (93.1%) higher than the other groups (p<0.05). Conversely, DRB1*11:01 association was absent in PNH/+ patients, but only they had malignant thymoma (87.5%), serum antibodies against leucine-rich glioma-inactivated 1 protein (66.7%) and against netrin-1 receptor deleted in colorectal carcinoma (53.8%), and myasthenia gravis (50.0%).
Interpretation Symptoms’ distribution supports specific clinical phenotypes without overlap between LE and MoS. The distinct immunogenetic characteristics shared by all patients with LE and the particular oncological and autoimmune associations of MoS suggest two very different aetiopathogenesis.
- CASPR2
- HLA
- limbic encephalitis
- Morvan syndrome
- neuromyotonia
Statistics from Altmetric.com
Introduction
Antibodies against contactin-associated protein-like 2 (CASPR2-Abs) are found in patients with acquired neuromyotonia (NMT), limbic encephalitis (LE) and Morvan syndrome (MoS).1 2 Initial descriptions of MoS included both peripheral nerve hyperexcitability (PNH) and central nervous system (CNS) features,3 4 but the co-occurrence of LE and NMT in some patients has raised doubts about whether these cases should be labelled as MoS, blurring the lines between these three different clinical presentations.5 6 Moreover, a recent case series suggested that instead of well-delineated syndromes, CASPR2-Abs associate with a set of core symptoms forming random combinations.5 The recent description of a shared human leucocyte antigen (HLA) association (DRB1*11:01) has also supported the assumption of CASPR2-Abs disease as a single aetiopathogenic entity.7 Systematic studies of the distribution of neurological symptoms among CASPR2-Abs patients are therefore of major importance in order to establish a clear classification by describing the defining characteristics of each phenotype and the existence and range of overlap among them, which will provide better insight into their underlying mechanisms. Herein, we performed a cluster analysis, which is a statistical tool that allows classifying subjects of similar types into respective categories,8 to explore the distribution of symptoms in a cohort of CASPR2-Abs patients. We then aimed to search for physiopathological clues by studying whether the immunological and genetic (HLA) characteristics differed according to the clinical phenotypes previously defined by the cluster analysis.
Methods
Subjects
All patients with CASPR2-Abs found in serum and/or cerebrospinal fluid (CSF) in our centre from July 2010 to November 2018 were identified and the clinical and paraclinical features retrospectively collected from hospital charts (table 1). Patients without enough data were excluded. Written consent was obtained from all patients.
List and definition of the clinical and paraclinical features
Antibody detection
CASPR2-Abs and antibodies against leucine-rich glioma-inactivated 1 protein (LGI1-Abs) were detected as previously described by immunohistofluorescence on rat brain sections and a cell-based assay (CBA).9 10 Titration of CASPR2-Abs in serum and CSF was done by endpoint dilution using CBA on HEK293-cells transfected with CASPR2-coding plasmids; titres were determined as the lowest dilution with positive signal.
Serum antibodies against the netrin-1 receptor deleted in colorectal carcinoma (DCC-Abs) were investigated by CBA, using HEK293-cells transfected with the plasmids encoding DCC and green fluorescent protein. Twenty-four hours after transfection, patients sera (two series were performed with sera diluted 1:20 and 1:100) were added and cells were incubated for 2 hours, then fixed with paraformaldehyde 1%, and incubated with the secondary goat antihuman antibody Alexa Fluor 555 (ThermoFisher Scientific, Waltham, Massachusetts, USA). The CBA were read by two different investigators (A-LP and VR) using a Zeiss Axiophot microscope (Zeiss, Oberkochen, Germany).
HLA analysis
HLA genotyping was performed in peripheral blood using next generation sequencing (NGS) technology as previously described,11 using the MiSeq sequencer system (Illumina, San Diego, California, USA) in CASPR2-Abs patients with available DNA. HLA genotyping was reported at a six-digit level whenever technically possible. Once the genotypes were obtained, the most likely haplotypes according to ethnical origin were selected based on the public database HaploStats of the National Marrow Donor Program. An ethnically matched sample of 300 healthy controls was provided by the HLA Laboratory from the French Blood Service (EFS Auvergne-Rhône-Alpes) with their genotypes at four-digit level for class I HLA (A, B, C), and DRB1 and DQB1 for class II HLA, also obtained by NGS technology (Omixon, Budapest, Hungary).
Statistical analysis
We selected 22 features of interest, including clinical features and signs of PNH on electroneuromyographic (ENMG; as a measure of PNH severity) recordings that were categorised into binary variables (presence/absence) and summarised as numbers and percentages. Other six variables, such as age, the presence of a malignant thymoma, polysomnographic recordings, brain MRI, electroencephalogram (EEG) and CSF analysis, were excluded from classification analysis. First, non-supervised analyses were performed using hierarchical clustering with Jaccard distance. The groups identified with the non-supervised analysis were then considered as outcomes for supervised analysis in order to clarify clinical profiles for each group. The random forest method was used in order to identify variables with the greatest importance for clustering. The features of interest were introduced in the random forest (ntree=1000, mtry=6). Thereafter, diagnostic test results (eg, brain MRI, CSF analysis, CASPR2-Abs titres, HLA genotypes) were compared between the groups that had been identified through classification analysis. Categorical variables were first compared with the Fisher’s exact test (two tailed), and continuous variables were evaluated with Mann-Whitney U test or Kruskal-Wallis H test. Bonferroni’s correction was applied to limit alpha risk inflation. Pairwise comparisons were then performed using the Holm procedure whenever statistically significant.12 Bonferroni’s method was also used for correction for multiple allelic comparisons in HLA analysis, multiplying the p value by the number of alleles for each locus. Corrected p<0.05 were considered significant. OR with 95% CI was used as a measure of the strength of associations.
All analyses were performed using the R software (R Core Team, 2014. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. URL http://www.R-project.org/), and SPSS software package V.25.0 (IBM Corp).
Results
Demographic features and ancillary tests
A total of 79 patients with CASPR2-Abs were diagnosed from July 2010 to November 2018 in the French Reference Center of Paraneoplastic Neurological Syndromes and Autoimmune Encephalitis. Twenty-three (29.0%) patients were excluded from analysis due to insufficient data (figure 1). Among the 56 patients analysed, 31 of them previously reported,9 46 were men (82.1%), and median age was 61 years (range: 27–82). The extension of the workup was found to be variable as it was based on clinical criteria and decided by each referral physician. Polysomnographic studies were performed in 15/56 (26.8%) of the patients, all had severe sleep symptoms (major insomnia, or suspicion of parasomnia or sleep apnoea), and demonstrated agrypnia excitata in 6/15 (40.0%) patients, and obstructive sleep apnoea in 9/15 (60.0%) patients. Patients with non-characterised insomnia did not undergo polysomnography. ENMG was performed in 35/56 (62.5%) patients, including 28 with PNH symptoms. Needle ENMG examination found spontaneous motor unit activities in 25/28 (89.3%) patients, including features considered as severe in 21/28 (75.0%). A length-dependent polyneuropathy of unknown aetiology was found in three patients (with axonal, n=1; and mixed pattern, n=2), while in other four patients the polyneuropathy was related to concomitant diabetes mellitus (n=3), and previous chemotherapy (n=1). Brain MRI found mesial temporal lobes signal changes typical of LE in 18/44 (40.9%) patients, consistent in all cases with the presence of limbic symptoms. EEG was reported as abnormal in 22/44 (50.0%) patients, including abnormal focal or generalised slowness, intercritical epileptiform activity and electroclinical seizures. Inflammation of CSF was found in 26/47 (55.3%) patients. The presence of oligoclonal bands (OCB) was investigated in 38/56 (67.9%) patients, and was positive in 7/38 (18.4%).

Flow chart presenting the study design, with the classification cluster analysis represented by a dendrogram and a heat map. The dendrogram shows how patients were progressively classified by the cluster analysis according to the distribution of clinical and paraclinical features, which are reflected in the heat map enabling to identify the main characteristics that define each group. CASPR2-Abs, anti-CASPR2 antibodies; ENMG, electroneuromyography; LE, limbic encephalitis; PNH, peripheral nerve hyperexcitability.
Classification analysis
We used non-supervised classification analysis to categorise our 56 patients based on similarities of symptoms’ combinations (figure 1); those with symptoms of limbic origin (ie, anterograde amnesia and temporal lobe epilepsy) were distinguished from those with PNH symptoms, as 27/31 (87.1%) of the patients with temporal lobe epilepsy and/or memory impairment were clustered separately from the 27/28 (96.4%) of patients with PNH symptoms.
Moreover, within the limbic-predominant group of patients (29/56, 51.8%), classification analysis grouped together 11 patients (11/29, 37.9%; 11/56, 19.6% of the overall cohort) who had frequent additional non-limbic CNS symptoms, including cerebellar ataxia (permanent in 8/11, 72.7%; and paroxysmal in 6/11, 54.5%) and hyperkinetic movement disorders (4/11, 36.4%), as well as dysautonomia (3/11, 27.3%) and weight loss (8/11, 72.7%). Extralimbic symptoms were uncommon in the 18 patients from the rest of the limbic-predominant group (18/29, 62.1%; 18/56, 32.1% of the overall cohort), being present in only 5/18 (27.8%) patients (permanent ataxia, n=1; paroxysmal ataxia, n=2; hyperkinetic movement disorders, n=1; PNH symptoms, n=1). These groups were therefore labelled LE/− (isolated LE, n=18), reflecting the prominent isolated limbic involvement, and LE/+ (extensive LE, n=11), in order to emphasise the frequent association with extralimbic features.
Among the 27 patients with predominant PNH features (27/56, 48.2%), classification analysis clustered 16/27 patients (59.3%; 16/56, 28.6% of the overall cohort) with severe PNH, as indicated by ENMG signs (15/15, 100% of those performed), functional impairment due to motor PNH signs (12/16, 75.0%), generalised PNH motor symptoms (13/16, 81.3%), neuropathic pain (12/16, 75.0%) and severe dysautonomia (11/16, 68.8%). All 16 patients had additional non-PNH symptoms, including non-limbic CNS involvement such as hyperkinetic movement disorders (8/16, 50.0%), permanent cerebellar ataxia (7/16, 43.8%), sleep disorders such as nocturnal hallucinations (7/16, 43.8%), any kind of insomnia (9/16, 56.2%) or proven agrypnia excitata (5/6, 83.3% from those with polysomnographic recordings), weight loss (9/16, 56.2%), and dyspnoea (8/16, 50.0%); no patient had clear limbic symptoms. In the remaining 11/27 patients with predominant PNH (40.7%; 11/56, 19.6% of the overall cohort), PNH was less severe (severe PNH ENMG signs in only 6/11, 54.5%; functional impairment due to motor PNH signs in 1/11, 9.1%; generalised PNH signs in 4/11, 36.4%; severe dysautonomia in 1/11, 9.1%; neuropathic pain in 6/11, 54.5%), and limbic symptoms were seen in 4/11 patients (36.4%), reflecting the presence of patients with the association of limbic and PNH features. These groups were therefore labelled, PNH/− in order to reflect mild and usually isolated PNH symptoms (n=11), and PNH/+ to reflect the association of severe PNH with extralimbic CNS involvement (n=16).
There were five patients of the cohort with combined PNH and limbic symptoms; they were distributed between the LE/− (n=1) and PNH/− (n=4) groups. Malignant thymoma and myasthenia gravis were found only in the PNH/+ group (14/16=87.5%, p=1.9×10−10; and 8/16=50.0%, p=2.7×10−4; respectively).
Table 2 presents the distribution of all collected variables and table 3 highlights the prominent clinical features in each group. Supervised random forest analysis identified PNH symptoms, severe PNH signs on ENMG, altered general state and weight loss, as the most important variables for classifying the patients into the four diagnostic groups.
Distribution of the clinical and paraclinical features in the overall cohort and the clinical groups defined in the cluster analysis
Description of the prominent features (seen in at least 50% of the patients) included in the classification analysis that statistically define the four clinical groups
Regarding the ancillary tests not included in the cluster analysis, the presence of mesial temporal signal changes in brain MRI was significantly more frequent in LE/− patients compared with PNH/+ patients (12/17, 70.6%; vs 0/13, 0.0%; p=5.2×10−4); there was no significant difference between the other groups (12/17, 70.6% LE/−, vs 3/8, 37.5% LE/+, p=0.58; 12/17, 70.6% LE/− vs 3/6, 50.0% PNH/−, p>0.99; 3/8, 37.5% LE/+, vs 0/13, 0.0% PNH/+, p=0.17; 3/8, 37.5% LE/+, vs 3/6, 50.0% PNH/− p>0.99; 0/13, 0.0% PNH/+, vs 3/6, 50.0% PNH/−, p=0.1). CSF inflammation was significantly more frequent in LE/− and LE/+ patients (14/17, 82.4%; and 8/11, 72.7%; respectively) compared with PNH/+ patients (1/13, 7.1%; p=6.9×10−4 and p=0.011, respectively) but not to PNH/− patients (3/6, 50.0%; p=0.8 and p>0.99, respectively). Brain MRI abnormalities (3/6, 50.0%) and CSF inflammation (3/6, 50.0%) in the PNH/− group were attributable to the 4 patients of this group who had overlapping limbic and PNH features. The presence of OCB was only detected in 7/38 (18.4%) patients, all had limbic features, but there was no significant difference when comparing the 4 groups (4/13, 30.8% LE/−; 3/9, 33.3% LE/+; 0/11, 0.0% PNH/+; 0/5, 0.0% PNH/−; p=0.84).
Immunological features
All but 1 of the sera tested for CASPR2-Abs (n=52: 16 LE/−, 9 LE/+, 16 PNH/+, 11 PNH/−) were found positive; there was no significant difference in the detection of serum CASPR2-Abs between groups (p=0.5). Among all tested CSF, 31/48 (64.6%) samples were positive for CASPR2-Abs. CSF detection rates of CASPR2-Abs did not differ between LE/− and LE/+ groups (16/18 vs 11/11, p=0.5); when comparing all patients with LE (27/29, 93.1%) to PNH/− and PNH/+ patients, detection of CASPR2-Abs in CSF was significantly more frequent in patients with LE than in those from both the PNH/− (27/29 vs 4/7, p=0.04) and PNH/+ (27/29 vs 0/12, p=3.5×10−8) groups. In addition, CASPR2-Abs were more commonly found in the CSF of PNH/− than of PNH/+ patients (4/7 vs 0/12, p=0.018); these were the four CSF-positive PNH/− patients who had overlapping PNH and limbic features. Serum LGI1-Abs were analysed in 50 patients (25 LE (16 LE/−, 9 LE/+), 15 PNH/+, 10 PNH/−) and only detected in PNH/+ patients (10/15, 66.7%, vs 0/45; p=1.1×10−5) and only in those with malignant thymoma (10/13 vs 0/37, p=2.8×10−8). Among the 46 CSF also tested for LGI1, only 1 (0.02%) was positive at very low titres (endpoint dilution, 1:20), belonging to a patient of the PNH/+ group. Serum DCC-Abs were analysed in 44 patients (22 LE (14 LE/−, 8 LE/+), 13 PNH/+, 9 PNH/−) and only detected in PNH/+ patients (7/13, 53.8%, vs 0/31, p=4.9×10−5; figure 2); all of them had a malignant thymoma (7/12, 58.3%, vs 0/32, p=2.1×10−5).

Immunological differences among distinct clinical phenotypes. (A) Differences in anti-CASPR2 antibodies (CASPR2-Abs) serum titres obtained by serial endpoint dilution using cell-based assay: levels are significant higher in limbic encephalitis (LE) than in peripheral nerve hyperexcitability (PNH)/+ and PNH/−. (B) Distribution of positivity (%) for CASPR2-Abs in serum and cerebrospinal fluid, and anti-LGI1 antibodies (LGI1-Abs) and netrin-1 receptor deleted in colorectal carcinoma antibodies (DCC-Abs) in serum, according to clinical classification (LE, PNH/+, PNH/−).
Serum was still available for the establishment of CASPR2-Abs endpoint dilution for 43 patients (13 LE/−, 9 LE/+, 12 PNH/+, 9 PNH/−). The median delay between clinical onset and the analysed sample was 384 days (range 24–3660), without significant differences between the groups (p=0.177). The median endpoint dilution was 1:40 960 (range: 1:10 240–1:81 920) for LE/−, 1:40 960 (range: 1:10 240–1:81 920) for LE/+, 1:3840 (range: 1:40–1:20 480) for PNH/+ and 1:160 (range: 1:20–1:40 960) for PNH/−. Serum CASPR2-Abs titres were not significantly different between LE/− and LE/+ patients (p=0.7), but they were significantly higher in all patients with LE combined compared with PNH/+ (p=5.28×10−6) and PNH/− groups (p=0.001); there was no significant difference between PNH/+ and PNH/− groups (p=0.75; figure 2). CSF was still available for CASPR2-Abs endpoint dilution in 31 patients (17 LE/−, 10 LE/+ and 4 PNH/− patients with overlapping limbic features); the median delay between clinical onset and the analysed samples was 384 days (range 24–4123), without significant differences between the groups (p=0.366). The median endpoint dilution was 1:1280 (range 1:20–1:10 240) for LE/−, 1:7680 (1:160–1:20 480) for LE/+, and 1:1280 (range 1:320–1:1280) for PNH/−; there was no difference (p=0.123) regarding the CSF titres between the three groups.
HLA genotyping
DNA was available for HLA genotyping for 30 patients, all were of Caucasian-origin, there were 28 men (93.3%) and the median age was 61.5 years (range: 28–73). The patients belonged, respectively, to groups LE/− (10/30, 33.3%), LE/+ (7/30, 23.3%), PNH/+ (8/30, 26.7%) and PNH/− (5/30, 16.7%). Of note, 7/8 (87.5%) of the PNH/+ patients genotyped had a malignant thymoma, and 5/8 (62.5%) had serum LGI1-Abs.
HLA allele DRB1*11:01 was present in 20/30 patients (66.7%) versus 55/300 (18.3%) in the healthy control group (p=1×10−6, OR=8.909, 95% CI 3.95 to 20.097). DQB1*03:01:01 was found at a similar frequency due to linkage disequilibrium with DRB1*11:01 (22/30 vs 100/300 in controls, p=3×10−4, OR=5.5, 95% CI 2.36 to 12.79).
Among the DRB1*11:01 carriers, 19/20 (95.0%) carried DQB1*03:01:01 along with DQA1*05 when DQA1 was successfully genotyped (17/19), forming the extended haplotype DRB1*11:01:01-DQB1*03:01.01-DQA1*05. The remaining DRB1*11:01 patient (group LE/+) had the DRB1*11:01:02-DQB1*05:02:01-DQA1*01 haplotype. Individual class II HLA genotyping results are detailed in table 4. Twenty-five (83.3%) patients carried at least one copy of DRB3, including all the DRB1*11:01 carriers, the remaining corresponding to DRB1*03:01 or DRB1*13:01 carriers. Thirteen (43.3%) patients carried at least one copy of DRB4, all of them were also carriers of DRB1*04 and/or DRB1*07:01. Only 4 (13.3%) patients carried one copy of DRB5, all of them DRB1*15:01 or DRB1*16:01 carriers.
Class II human leucocyte antigen haplotypes and clinical classification in 30 patients with anti-CASPR2 antibodies
Regarding the clinical presentations, DRB1*11:01 was carried by most LE/+ and LE/− patients (16/17=94.1%) compared with only 25.0% (2/8) of PNH/+ patients (p=0.003, OR=3.765, 95% CI 1.127 to 12.576), and 40.0% of PNH/− patients (2/5, p=0.048, OR=2.353, 95% CI 0.799 to 6.929). The frequency of DRB1*11:01 among PNH/+ (25.0%) and PNH/− (40.0%) patients was not significantly different to that found in the healthy control group (18.3%; p=0.6 and p=0.2, respectively), but significantly higher in patients with LE compared with the healthy control group (94.1% vs 18.3%; p=1.3×10−10, OR=71.3, 95% CI 9.25 to 548.87; figure 3). None of the LGI1-Abs-positive patients carried the DRB1*07:01 allele.

Human leucocyte antigen (HLA)-DRB1*11:01 is only associated with limbic encephalitis (LE). Pie chart representing the carrier frequencies for the allele HLA-DRB1*11:01 in the control (healthy) group, the overall anti-contactin-associated protein-like 2 (CASPR2) cohort and the groups of limbic encephalitis (LE), peripheral nerve hyperexcitability (PNH)/− and PNH/+.
Discussion
CASPR2-Abs are classically associated with acquired NMT, MoS and LE,1 2 but recent studies suggested that their clinical spectrum is in fact more extensive and borders among them may be blurred.5 6 The present study found that symptoms of CASPR2-Abs patients do not associate randomly, but they form preferential combinations instead. In particular, limbic and PNH symptoms tend to cluster separately and their overlap represents only a minority of the patients (figure 4). On one hand, limbic symptoms can either be the only CNS features in the patients (LE/− group), or associate with non-limbic symptoms such as cerebellar ataxia or hyperkinetic movement disorders (LE/+ group), thereby confirming that the phenotype of CASPR2-Abs LE extends beyond limbic symptoms.5 9 13–15 On the other hand, a group of patients who had mild PNH symptoms (PNH/− group) corresponded to patients with NMT, which can appear isolated or combined with limbic symptoms in a minority of patients.9 16 In addition, we identified a group of patients with PNH features that were considered to be severe and with frequent non-limbic CNS symptoms including sleep disturbances and severe dysautonomia (PNH/+). Interestingly, this combination of symptoms is reminiscent of the historical descriptions of MoS,3 and this clinical presentation was strongly associated with an underlying malignant thymoma.4 5 16

{kind=link}
{kind=link}
{kind=link}
{kind=link}
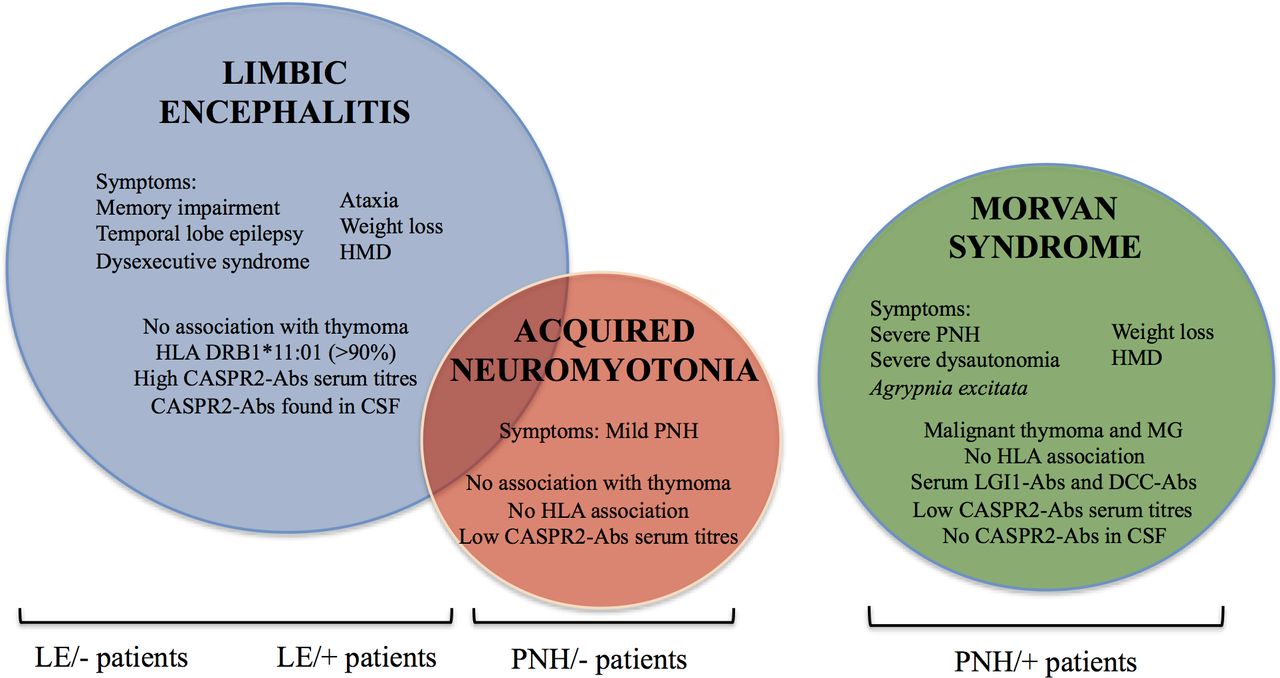
Clinic and immunogenetic features define three major anti-CASPR2 antibodies (CASPR2-Abs) diseases with different pathogenesis. Schematic features and distribution within the present study population of the three main CASPR2-Abs syndromes (limbic encephalitis (LE), acquired neuromyotonia (NMT), Morvan syndrome), as suggest the results of the cluster analysis; a minority of patients had an association of NMT and LE features. CSF, cerebrospinal fluid; DCC-Abs, netrin-1 receptor deleted in colorectal carcinoma; HLA, human leucocyte antigen; HMD, hyperkinetic movement disorders; PNH, peripheral nerve hyperexcitability.
A sleep recording demonstrating agrypnia excitata is usually considered as the cornerstone of the diagnosis of MoS,17 18 but due to the retrospective collection of the data, systematic polysomnographic recordings were lacking to study this aspect herein. It is however remarkable that sleep disturbances were very common in PNH/+ patients and over 80% with polysomnographic recording had a classical pattern of agrypnia excitata.19 Moreover, a polysomnographic recording was not performed in patients with non-characterised insomnia, and as most of them belonged to the PNH/+ group, it is likely that objective sleep disturbances are underestimated in such patients. Notably, polysomnographic recording of one LE/+ patient having problem of major insomnia also displayed an agrypnia pattern. Of note, obstructive sleep apnea syndrome was also frequently observed in patients outside of the PNH/+ group. This finding could be fortuitous and be due to the over-representation of middle-aged men, although it may also result from autonomic dysregulation.20 More systematic recordings will be necessary to fully apprehend the nature of the sleep disorders in the various CASPR2-Abs syndromes.
Although the PNH/+ patients have highly distinctive features reminiscent of MoS, we found that patients from the LE/+ group can have features resembling those of PNH/+ patients (ie, weight loss, dysautonomia and hyperkinetic movement disorders). Nevertheless, LE/+ patients had no associated malignant thymoma, no PNH symptoms and usually mild dysautonomia. In addition, LE/+ patients had immunological and genetic characteristics similar to LE/− instead of PNH/+ patients, suggesting that LE/− and LE/+ patients share a common pathogenesis and should be considered as a single entity. We also confirm the previous findings that LE is associated with increased serum titres and increased CSF detection of CASPR2-Abs compared with patients with NMT (PNH/−) and MoS (PNH/+).9 21 Interestingly, high CASPR2-Abs serum titres and CASPR2-Abs in CSF in PNH/− patients were only present in those with overlapping LE. Although CASPR2-Abs in CSF have been also reported in other clinical phenotypes different from LE,5 22 this discrepant finding may be due to a distinct clinical classification. For instance, MoS criteria included features of likely limbic origin, such as seizures or cognitive impairment5; it is therefore probable that some patients with LE/+ have been classified as MoS in other studies. Technical differences among laboratories, such as distinct CSF dilutions,2 9 may also explain the difference in CASPR2-Abs detection in the CSF. However, even assuming sensitivity is lower herein, which would entail being unable to detect very low levels of CASPR2-Abs in the CSF of patients with MoS, this would still suggest that high levels of CSF CASPR2-Abs are only associated with LE. Since the epitopes targeted by CASPR2-Abs are similar among patients,23 phenotype determination could depend in part on the site of CASPR2-Abs synthesis.9
Importantly, the differences in the immunological and genetic characteristics in the PNH/+ group are likely related to the increased frequency of malignant thymoma. Here, we demonstrate that HLA-DRB1*11:01, which has been previously reported in patients with CASPR2-Abs without specific clinical links,7 is in fact only found in strong association with patients with LE, while this association was absent in the PNH/+ group, whose carrier frequencies were similar to those of healthy population. Interestingly, an in silico study has shown that DQB1*03:01-DQA1*05:01 (which are in linkage disequilibrium with DRB1*11:01) heterodimer may be involved in CASPR2-derived peptides presentation.7 Therefore, two independent immunological pathways may be involved in CASPR2-Abs patients, depending on the presence or not of a malignant thymoma. In those cases not associated with such tumour, altered peptide presentation to CD4 T-cells mediated by class II HLA may allow evasion of thymic negative selection and/or peripheral self-tolerance mechanisms. Conversely, in patients with malignant thymoma breaking of tolerance is likely to result from abnormal T-cell maturation within the tumour microenvironment, implying a wider and less specific immune response. This is consistent with the frequent presence of myasthenia gravis and LGI1-Abs in patients with malignant thymoma,4 5 16 who, in addition, remarkably lacked the DRB1*07:01 allele recently linked to anti-LGI1 encephalitis.7 24 25 Of note, we have also confirmed the association between the anti-netrin-1 receptor DCC-Abs in patients with CASPR2-Abs and malignant thymoma, illustrating the wide spectrum of the immune response in thymoma-associated CASPR2-Abs diseases.26
The mains limitations of the present study are its retrospective nature and that a comprehensive workup was not performed equally in all patients. Nevertheless, only ENMG was included in the cluster analysis as it has been previously reported that the characteristics of patients with PNH symptoms with and without PNH signs on ENMG are the same, suggesting that ENMG has a quantitative value in PNH diagnosis, instead of a qualitative one.27 In our opinion, this cannot therefore be considered as a bias in the clinical classification, but we believe that it is highly important to conduct complete evaluations in patients with CASPR2-Abs. This strategy would enable to better classify them, and should be followed in future prospective studies. Another limitation is the small sample size for a few of the statistical analyses, specially concerning the CASPR2-Abs CSF positivity and HLA genotyping in the PNH/− group; the results presented herein should therefore be confirmed in larger samples.
In conclusion, the present study shows that symptoms do not combine randomly in CASPR2-Abs patients, and confirms the existence of different clinical phenotypes with only a minor overlap between LE and NMT, and MoS as the most distinctive group. The particular immunogenetic characteristics shared by the two groups of LE support considering them as a single entity, with a completely different aetiopathogenesis from MoS, which has its own specific defining comorbidities. Future studies are needed to clarify how immunological and neurobiological mechanisms determine clinical phenotypes in CASPR2-Abs patients.
Acknowledgments
The authors thank NeuroBioTec Hospices Civils de Lyon BRC (France, AC-2013-1867, NFS96-900) for banking sera and CSF samples. They thank Philip Robinson for help in manuscript preparation (Direction de la Recherche Clinique, Hospices Civils de Lyon).
References
Footnotes
SM-C and BJ contributed equally.
Contributors Conception and design of the study and drafting the manuscript and figures: SM-C, BJ and JH. Acquisition and analysis of data: all authors.
Funding This study is supported by research grants from ANR (ANR-14-CE15-0001 MECANO) and Fondation pour la recherche medicale DQ20170336751. This work has been developed within the BETPSY project, which is supported by a public grant overseen by the French National Research Agency (ANR), as part of the second ‘Investissements d'Avenir’ program (reference ANR-18-RHUS-0012). SM-C is supported by a research a grant from Fundación Alfonso Martín Escudero (Spain).
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval The Institutional Review Board of Université Claude Bernard Lyon 1 and Hospices Civils of Lyon approved the study (ICARE NCT-04106596).
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement Data reported in this manuscript are available within the article. More information regarding the data is available from the corresponding author on reasonable request. Individual data will not be shared to conform to the privacy statement signed by the patients.