Article Text

Abstract
Objectives To evaluate the prevalence of late-onset neutropenia and its complications in patients treated with rituximab (RTX) for rheumatoid arthritis (RA) and other autoimmune diseases (AIDs) in a prospective registry.
Methods The AutoImmunity and Rituximab registry is an independent 7-year prospective registry promoted by the French Society of Rheumatology. For each episode of neutropenia, data were validated by the clinician in charge of the patient.
Results Among 2624 patients treated with RTX for refractory AIDs, and at least 1 follow-up visit (a total follow-up of 4179 patient-years in RA and 987 patient-years in AIDs), late-onset neutropenia was observed in 40 patients (25 RA (1.3% of patients with RA, 0.6/100 patient-years), and AIDs in 15 (2.3% of patients with AIDs, 1.5/100 patient-years)). 6 patients (15%) had neutrophils <500/mm3, 8 (20%) had neutrophils between 500 and 1000/mm3, and 26 (65%) had neutrophils between 1000 and 1500/mm3. Neutropenia occurred after a median period of 4.5 (3–6.5) months after the last RTX infusion in patients with RA, and 5 (3–6.5) months in patients with AIDs. 5 patients (12.5%), 4 of them with neutrophils lower than 500/mm3, developed a non-opportunistic serious infection and required antibiotics and granulocyte colony-stimulating factor injections, with a favourable outcome. After resolution of their RTX-related neutropenia, 19 patients (47.5%) were re-treated, and neutropenia reoccurred in 3 of them.
Conclusions Late-onset neutropenia might occur after RTX and may result in serious infections. Thus, monitoring of white cell count should be performed after RTX. However, in this large registry of patients with AIDs, the frequency of RTX-induced neutropenia was much lower than that previously reported in patients treated for blood malignancies or AIDs.
- Rheumatoid Arthritis
- Autoimmune Diseases
- Treatment
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
Key messages
What is already known about this subject?
Late-onset neutropenia rituximab was mainly reported in patients treated for lymphoma but data in patients with rheumatoid arthritis and other AIDs are very limited.
What does this study add?
The incidence of LON is much lower in RA and other AIDs than in blood malignancies. Neutropenia is usually mild and might not be complicated with infections.
How might this impact on clinical practice?
Instead of monitoring whole blood count after each cycle of RTX, a more pragmatic approach could be to have a blood count performed in the event of fever or infection in the months following RTX treatment.
Introduction
Late-onset neutropenia (LON) after B-cell depletion by rituximab (RTX) was mainly reported in patients treated for lymphoma with an observed prevalence of 8%.1 LON can occur from 1 month up to 1 year after RTX.2 The mechanism of this complication remains poorly understood. Several assumptions exist regarding the pathogenesis of neutropenia after RTX in B-cell lymphoma, including the role of antineutrophil antibodies, large granular lymphocytes, competition for growth factors between lymphopoiesis and granulopoiesis,3–7 and the role of genetic polymorphisms in the immunoglobulin G (IgG) receptor FCγ RIIIA.8 ,9 The upregulation of B-cell activating factor of the tumour necrosis factor (TNF) family (BAFF) after B-cell depletion might also play a role by favouring B-cell repopulation to the detriment of granulopoiesis.3 The pathogenesis and concomitant treatments are very different between autoimmune diseases (AIDs) and lymphomas, which are usually treated with associated chemotherapy. Data on LON in patients with rheumatoid arthritis (RA) and other AIDs are very limited.10–15 One series of patients included 209 patients (162 RA and 47 AIDs, including 15 with systemic lupus erythematosus (SLE), 13 with granulomatosis with polyangiitis (GPA), 6 with juvenile RA and 13 with other AIDs), among whom 11 (5.2%: 5 RA and 6 AIDs) developed neutropenia.10 Recently, a retrospective series of 108 patients with RA reported 5 LON, of whom 2 developed infection.15 The aim of the present study was to evaluate the prevalence of LON and its complications in a large prospective cohort of patients treated with RTX for AIDs.
Methods
The French Society of Rheumatology and the Club Rhumatismeet Inflammations have set up the AutoImmunity and Rituximab (AIR) registry. The AIR registry is a multicentre prospective cohort designed to study the safety and efficacy of RTX in the treatment of RA and other refractory AIDs. Follow-up data are collected every 6 months over 7 years. Serious adverse events, including serious infections (requiring hospitalisation and/or intravenous antibiotics), cancers and deaths, are validated by the two coordinators of the registry using chart copies.
The methodology of the registry was reported previously.16 ,17 This study was approved by the French authorities Comité Consultatif sur le Traitement de l'information en matière de Recherche dans le domaine de la Santé and Commission Nationale de l'Informatique et des Libertés. Written informed consent was obtained from all patients. Neutropenia is defined by an absolute blood neutrophil count less than 1500/mm3. Neutrophil count was requested at inclusion and at each follow-up visit (3 months, 6 months then every 6 months, or at any time in case of treatment change). Late-onset RTX-related neutropenia was defined as an absolute neutrophil count of ≤1.5×109/L starting from 4 weeks after termination of RTX therapy until 12 months after the last RTX infusion.2 Neutropenia prior to RTX and other drug-related neutropenia were excluded. At each visit, the crf includes specific questions regarding the potential complications of neutropenia. For each episode of neutropenia, data were abstracted from the electronic crf, validated and completed if necessary, using a specific questionnaire, by the clinician in charge of the patient.
Statistical analysis
Patients contributed person-years of follow-up between the first infusion of the first cycle and death, or the last follow-up visit. For the incidence rate calculation of neutropenia, the time of neutropenia was used as the right censoring rule. Rates of neutropenia are presented as event/100 patient-years. Data are presented as median (IQR) for quantitative values and proportions for qualitative values. All analyses were performed using SAS software V.9.3 (SAS system SAS Institute, Cary, North Carolina, USA). In univariate analysis, a χ2 test or Fisher's exact test was used for qualitative data according to application requirements. A non-parametric Mann-Whitney U test was used for quantitative values. A p value <0.05 was defined as significant.
Results
Characteristics of patients with neutropenia
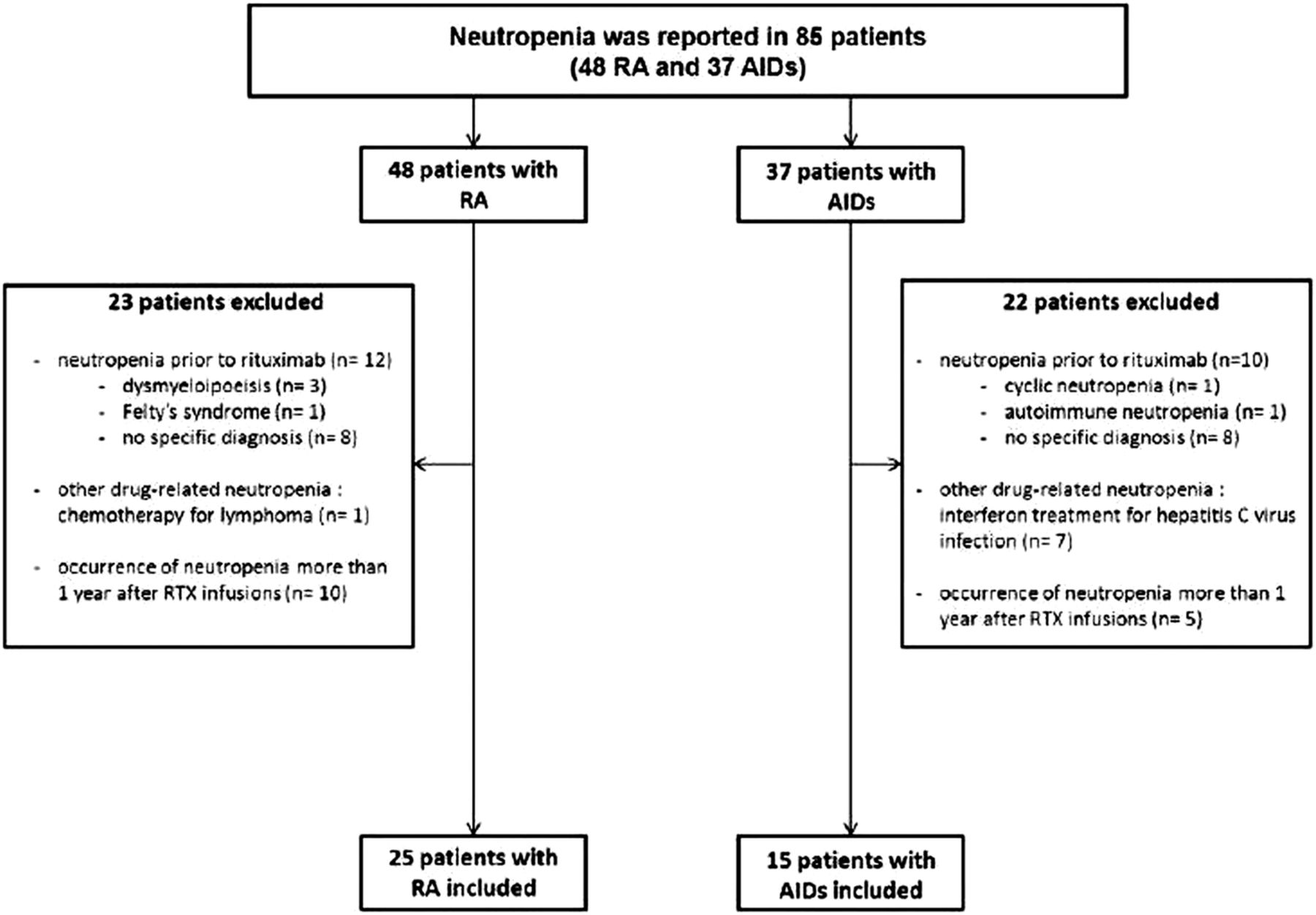
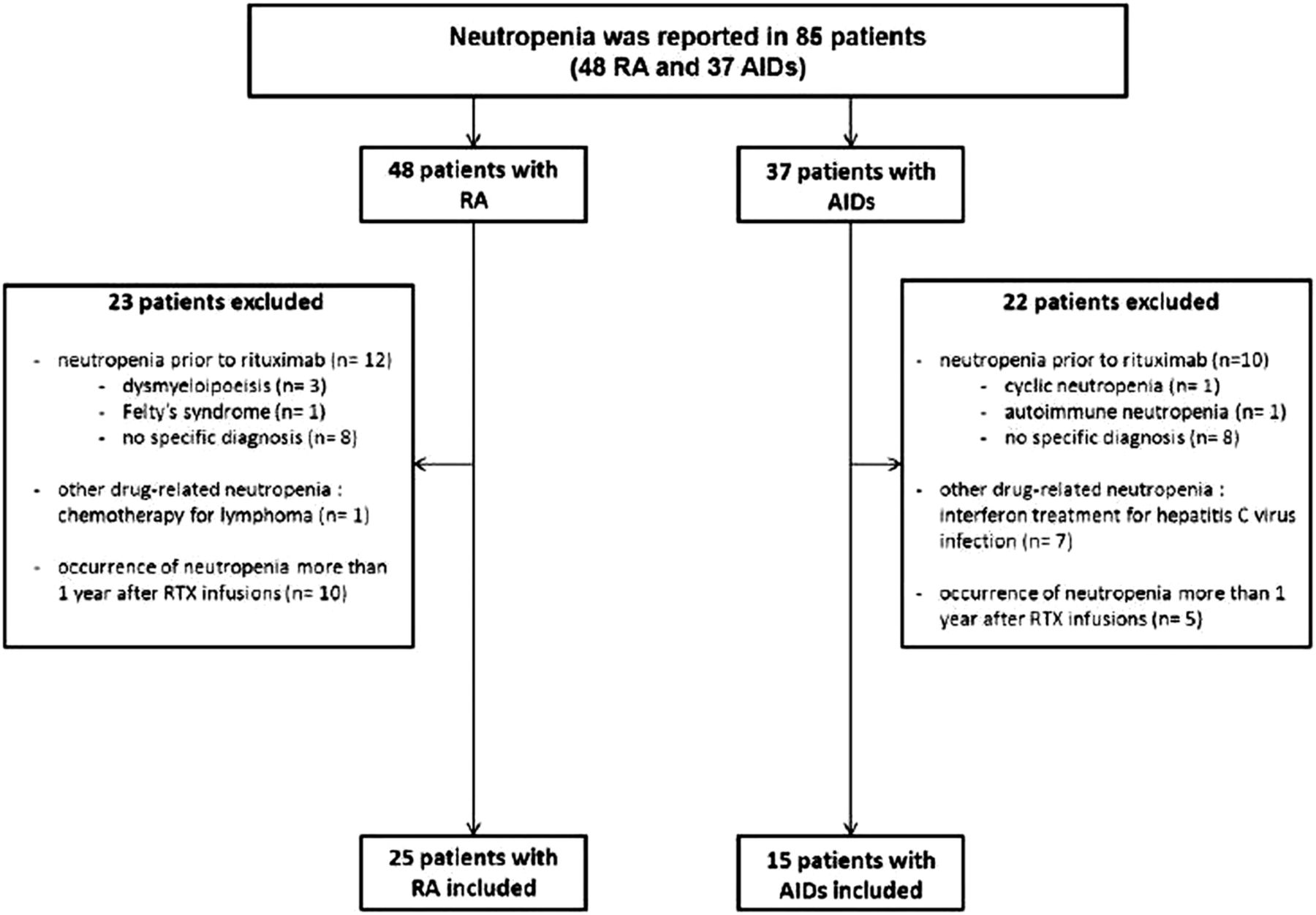
At the time of analysis, 2624 patients had at least one follow-up visit, including 1975 patients with RA and 649 patients with other AIDs. The median follow-up of patients with RA was 24.2 months (14.7–35.3) (4179 patient-years) and that of patients with AIDs was 17.4 months (5.6–29.1) (987 patient-years). The median follow-up after the last regimen of RTX was 14.4 months (7.1–27.8) in RA and 18.6 months (8.5–31.8) in AIDs. The median (IQR) number of blood counts was 4 (3–6) for patients with RA. The median (IQR) interval between blood counts was 5.2 (4.1–6.7) months for patients with RA. The median (IQR) number of blood counts/cycles of RTX was 2 (1.4–3) for patients with RA. Neutropenia was reported in 85 patients (48 RA and 37 AIDs). Forty-five patients were excluded since they actually had neutropenia prior to RTX (n=22, including dysmyelopoiesis (n=3), Felty's syndrome (n=1), cyclic neutropenia (n=1), autoimmune neutropenia (n=1), no specific diagnosis (n=16)), had other drug-related neutropenia (n=8, including interferon treatment for hepatitis C virus infection (n=7), chemotherapy for lymphoma (n=1) or had normal neutrophil counts within 1 year after RTX infusions and one occurrence of neutropenia more than 1 year after RTX infusions (n=15) (figure 1). For the remaining 40 patients, including 25 RA (1.3% of patients, 0.6/100 patient-years) and 15 AIDs (2.3%, 1.5/100 patient-years), 7 SLE, 7 vasculitis (including 6 cryoglobulinemia-related vasculitis and 1 GPA and 1 myositis), no other cause of neutropenia but RTX was identified by the clinician. The characteristics of these 40 patients (37 women, 3 men) with LON are summarised in table 1.
Characteristics of the 40 patients who developed rituximab-related neutropenia
{kind=link}
Flow chart of the study (AIDs, autoimmune diseases; RA, rheumatoid arthritis; RTX, rituximab).
Characteristics of late-onset neutropenia
Six patients (1 RA (0.05% of patients with RA, 0.02/100 patient-years) and 5 AIDs (0.7% of patients with AIDs, 0.5/100 patient-years)) had neutrophils <500/mm3, 8 (7 RA and 1 AIDs) had neutrophils between 500 and 1000/mm3 neutrophils, and 26 (17 RA and 9 AIDs) had neutrophils between 1000 and 1500/mm3.
Neutropenia occurred after a median period of 4.5 (3–6.5) months after the last infusion of RTX in patients with RA and 5 (3–6.5) months in patients with AIDs. In patients with RA, neutropenia occurred after the first cycle in 2 patients, after the second cycle in 4 patients, after the third cycle in 7 patients with RA and after the fourth cycle or later in 12 patients. In patients with AIDs, neutropenia occurred after the first cycle in 9 patients, after the second cycle in 5 patients and after the fourth cycle in 1 patient. Numerous episodes of neutropenia occurred after the second or subsequent cycle of RTX (92% in RA and 44% in AIDs). They were mainly mild neutropenia (blood neutrophil count between 1000 and 1500/mm3 in 17 RA and 2 AIDs; between 500 and 1000/mm3 in 6 RA and 1 AIDs; 3 AIDs had neutrophils <500/mm3).
Five patients (1 RA and 4 AIDs) (12.5% of patients with neutropenia), four of them with neutrophils lower than 500/mm3, developed a non-opportunistic serious infection and required antibiotics and granulocyte colony-stimulating factor (G-CSF) injections, with a favourable outcome. These episodes of neutropenia occurred after the first cycle for 2 patients, after the second cycle for 2 patients and after the fourth cycle for 1 patient. No patient had an opportunistic infection (table 2). In all patients, the outcome was favourable after treatment.
Characteristics of the five patients treated with antibiotics and growth factors
Associated factors with LON in RA
Among the baseline characteristics of patients with RA, including gender, disease duration, RF and anti-cyclic citrullinated peptide activity, the number of previous synthetic disease-modifying antirheumatic drugs (DMARDs), number of previous anti-TNF, disease activities at enrolment, concomitant treatment with DMARD or corticosteroids, serum gammaglobulin and IgG levels, only female gender and age were associated with neutropenia (table 3).
Associated factors with LON in RA
Re-treatment with RTX
Nineteen patients (47.5%) with previous neutropenia after RTX received a new infusion of RTX after resolution of their neutropenia (13 patients with RA with a previous blood neutrophil count between 1000 and 1500/mm3, four patients with RA between 500 and 1000/mm3, and two patients with SLE between 1000 and 1500/mm3). In the patients re-treated with RTX, the median number of cycles was 3 (2–4) in RA and 2 (2–2) in AIDs. The median follow-up of the re-treated patients was 26.1 months (21.8–39.2) in RA and 25.2 months (19.6–30.8) in AIDs. Neutropenia reoccurred in three of them (blood neutrophil count between 1000 and 1500/mm3 in two, and between 500 and 1000/mm3 in one). None of these recurrent episodes of neutropenia required growth factors or was complicated by an infection.
Discussion
The occurrence of late-onset neutropenia after RTX was infrequent in a large prospective registry, and the related complications were moderately severe. However, the rate of late-onset neutropenia after RTX in patients with RA and other AIDs has not been clearly determined. The AIR registry was very well adapted to this purpose since the occurrence of neutropenia and the blood neutrophil count were specifically requested in the e-crf at each follow-up visit. In addition, data validation by the clinician allowed us to identify patients with neutropenia unrelated to RTX. However, the main limitations of the study are related to its observational design, and missing data, notably duration of neutropenia that was not requested by the crf.
The first important result of this study is the low rate of late-onset neutropenia after RTX in RA (1.3% of patients, 0.6/100 patient-years) and other AIDs (2.3%, 1.5/100 patient-years) in a large multicentre registry of unselected patients. The rate observed in this study is much lower than in the few previous reports concerning AIDs.10–12 Despite the observational setting of this registry study, patients had regular assessments of neutrophil counts approximately every 6 months. However, asymptomatic LON can occur in between blood tests. Thus, it cannot be ruled out that the higher frequency of neutropenia after RTX in patients with haematological malignancies could also be partly related to the more frequent follow-up of blood counts by haematologists than by rheumatologists. Therefore, the actual frequency of LON in this study might be underestimated as reported in lymphomas.18
In our study, the mean time of onset of neutropenia was approximately 5 months, in accordance with what has been observed in this previous studies in AIDs and in lymphoma (around 6 months1–3), confirming their known late onset. No risk factor of neutropenia could be identified among the baseline characteristics of patients with RA, except age and female gender. Concerning gender, this may be simply due to the significantly higher prevalence of AIDs in women. Of note, lymphoma gender-based differences in RTX clearance were reported in elderly (>70 years) female patients treated with RTX for diffuse large B-cell lymphomas.19 The large numeric disequilibrium between 25 patients with RA with neutropenia and over 1900 patients without neutropenia inevitably led to a flawed statistical analysis due to type 2 errors.
The second important result was the low number of complications associated with neutropenia after RTX. First, most of the LONs were mild (>500/mm3), and only a minority of the patients who had a very low blood neutrophil count required growth factors and antibiotics. Among the five patients who required growth factors and antibiotics, two had concomitant cyclophosphamide and were not treated with a concomitant immunosuppressant other than RTX. Concordantly, a previous report also showed that complications usually concern patients with a very low blood neutrophil count.3 However, the overall rate of infections was higher in that previous report than in this study, which might be related to a different distribution of AIDs. No opportunistic infection or death was related to neutropenia. Thus, late-onset neutropenia does not seem to increase the risk for serious infection as much as RTX-related hypogammaglobulinemia.13 ,20 The absence of clinical consequences of most of these neutropenias might explain that more than half of the patients with RA with a history of previous RTX-induced mild neutropenia were subsequently re-treated with RTX. However, data regarding the risk of reoccurrence of neutropenia after re-treatment with RTX are not available in the literature. Interestingly, in this study, a recurrent episode of uncomplicated neutropenia was observed in only 16% of re-treated patients, with only one patient having a blood neutrophil count below 1000/mm3. However, no firm conclusions can be drawn about RTX re-treatment of patients with previous LON, since there was a selection bias in patients who were re-treated, all of whom had previously experienced only mild neutropenia.
Conclusion
Late-onset neutropenia might occur after RTX in patients with RA and other AIDs, but its incidence is much lower than in patients with blood malignancies. In addition, late-onset neutropenia is usually mild and might not be complicated with infections. Regarding clinical practice, it has been recommended to monitor whole blood count after each cycle of RTX.21 Since late-onset neutropenia is not frequent, not predictable and of varying onset and duration, and since it rarely results in significant infection, a more pragmatic approach could be to have a blood count performed in the event of fever or infection in the months following RTX treatment.
Acknowledgments
Roche provided an unrestricted educational grant to the French Society of Rheumatology but was not involved in the design, protocol, data collection or statistical analysis of the study. The authors thank all the investigators who have included patients in the AIR registry, the French Society of Rheumatology (SFR), the Club Rhumatismes et Inflammation, the French National Society of Internal Medicine (SNFMI) for their implication in the AIR registry, Rosemary Jourdan (Roche), Jamila Filipecki and Nadine Mackenzie (formerly Roche). They also thank the 14 research study nurses (A Bourgeois, E Braychenko, F Carmet, MH Da Silva, S Delmas, D Guinement, R Lefebure, C Lehning, N Minot, FMA Ouattara, V Pinosa, M Reau, H Thibault and E Wallet), L Dongmo and V Martin, all working in Euraxipharma, the contract research organisation in charge of data collection in the AIR registry.
References
Footnotes
Contributors All the authors contributed to data collection, interpretation of results and edited the manuscript. IP and PR performed statistical analyses. JHS, JEG and XM initiated the study and wrote the manuscript.
Competing interests None declared.
Patient consent Obtained.
Ethics approval Comité Consultatif sur le Traitement de l'information en matière de Recherche dans le domaine de la Santé.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement No additional data are available.