Article Text

Abstract
Context The challenge to provide a palliative care service for individuals with advanced neurological conditions is compounded by variability in disease trajectories and symptom profiles. The National End of Life Care Programme (2010) recommended seven ‘triggers’ for a palliative approach to care for patients with advanced neurological conditions.
Objectives To establish the frequency of triggers in the palliative phase, and if they could be reduced to fewer components. Management of the terminal phase also was evaluated.
Method Retrospective study of 62 consecutive patients under the care of a specialist palliative neurology service, who had died. Principle component analysis (PCA) was performed to establish the interrelationship between triggers.
Results Frequency of triggers increased as each patient approached death. PCA found that four symptom components explained 76.8% of the variance. These represented: rapid physical decline; significant complex symptoms, including pain; infection in combination with cognitive impairment; and risk of aspiration. Median follow-up under the palliative care service was 336 days. In 56.5% of patients, the cause of death was pneumonia. The terminal phase was recognised in 72.6%. The duration of the terminal phase was 8.8 days on average, and the Liverpool Care of the dying Pathway was commenced in 33.9%. All carers were offered bereavement support.
Conclusions Referral criteria based on the triggers can facilitate appropriate and timely patient access to palliative care. The components deduced through PCA have face validity; however larger studies prospectively validating the triggers are required. Closer scrutiny of the terminal phase is necessary to optimise management.
- End-of-life
- Terminal care
- Prognosis
- Neurological conditions
Statistics from Altmetric.com
Introduction
The NHS end of life care strategy in 2008 aimed to improve access to high-quality care for all individuals approaching end of life irrespective of their diagnosis.1 Despite this, research has demonstrated that only a small proportion of patients with non-malignant disease, including neurological conditions, access specialist palliative care services.2 Typically, for individuals with advanced neurological conditions (ANC), the last year of life is one of rapid deterioration, with intractable symptoms and complex cares needs, often resulting in unexpected and unwanted hospitalisation. Death is frequently unforeseen by patients and healthcare teams, thus robbing individuals and their loved ones of the opportunity to prepare for such events.
Barriers are perceived by service providers in delivering effective palliative care to patients with ANC.3 A particular challenge is that these patients present a wide variability in symptoms and disease progression.2 For example, patients with motor neuron disease (MND) may have a prognosis of months, whereas those with multiple sclerosis (MS) and Parkinson's disease (PD) can live for several decades with their condition. Services fear being unable to relieve symptoms or having the capacity to support people over a prolonged period.
Predicting prognosis on an individual basis is also difficult in such patients.4 Some die suddenly following an acute intercurrent illness, such as infection, and others can live for many years despite significant disability. It is crucial, however, to recognise when the end of life is near, and the focus of care should be palliative in its aims. This recognition can enable appropriate referral to palliative care services and also ensure timely discussion of future wishes and preferences in the form of advance care planning (ACP).3
A unified service supporting such patients and their carers, therefore, needs to be flexible, providing care as required, in addition to being well coordinated, with clearly defined referral criteria in order to prevent services becoming overwhelmed. The National End of Life Care Programme (NEoLCP), in their framework for long-term neurological conditions, suggested there are seven ‘triggers’ indicating the need for palliative care input and ACP.3 These included swallowing problems, recurrent infections, marked decline in physical status; as well as the first episode of aspiration pneumonia, cognitive difficulties, weight loss and significant complex symptoms. Services are encouraged to use these triggers as a guide to when a palliative approach to care is appropriate in ANC.3
The triggers were based on expert consensus. In order to initiate the evaluation of the seven triggers, we conducted a retrospective analysis of 62 consecutive deaths of patients with ANC. All patients had been referred to a community specialist palliative neurology service (SPNS) when they were thought to be entering the palliative phase of their illness. The referral criteria are outlined in figure 1. We evaluated changes in triggers during the time the patient was under the SPNS to determine the frequency of triggers during the palliative phase, and whether the triggers could be reduced to fewer components, and to examine the relationship between triggers and death. The terminal phase and its management were also assessed, as this is an important area currently poorly studied.

Description of the indicators used by the specialist palliative neurology service to determine when a palliative care approach is appropriate.
Method
Study design
A retrospective observational study was conducted, as part of a larger study, assessing if a SPNS was meeting the recommendations established by the NEoLCP in 2010.3
Setting
All participants resided within the catchment area of a hospice in Scarborough, UK, and had been accepted under the care of the SPNS. Patients included had died between December 2006 and April 2012, and data was extracted during November 2011 and May 2012 from computerised and paper clinical records.
Participants
Each participant had a diagnosis of an ANC and had been referred to the SPNS either by themselves or their carer, or via a neurologist, general practitioner (GP) or the community multidisciplinary (MDT) team. Patients with inadequately documented information to assess triggers and input from the service were excluded. Patients who were under the care of the palliative care team for another condition, such as disseminated malignancy, were also excluded, as they were not managed primarily by the SPNS. Of the 67 cases reviewed, 62 consecutive deaths were analysed.
Data
Demographic data including age, sex, diagnosis and comorbidities were determined; as well as the time from diagnosis to death and time under the SPNS. The frequency of episodes of change in triggers was established. In addition to the seven triggers suggested by the expert group we also looked at whether pain featured during the palliative phase and predicted death—which became the eighth trigger. The addition of the eighth trigger was prompted by studies highlighting the prevalence of pain in this patient group during the palliative phase.5–7
With regard to the terminal phase, we recorded the cause and place of death, and if dying was recognised. Management of the terminal phase was assessed against the NEoLCP guidance, requiring:
-
regular review and management of symptoms AND
-
documentation of discussions with family members AND
-
management of carer distress AND
-
psychosocial support.
The use of the Liverpool Care Pathway (LCP)8 and bereavement support was noted, as were symptoms and the duration of the terminal phase. The criteria for assessing each outcome were established prior to data collection (table 1). All ambiguous data were classified as missing.
Data extraction criteria established prior to data collection
Bias
Bias was limited as one researcher who had no previous contact with the patients collected all data. There was no loss to follow-up, and multiple sources of data were used.
Statistical analysis
SPSS V.19.0 was used for the statistical analysis. Descriptive statistics are provided.
Principal component analysis (PCA) is a way of identifying patterns in data, and expressing the data in such a way as to highlight their similarities and differences. It is used to analyse groups of correlated variables representing one or more common components. This technique was used to explore the different triggers to determine common components. In order to minimise missing data, only patients who had been under the care of the SPNS for the entirety of the last 6 months of their life (n=52) were included.
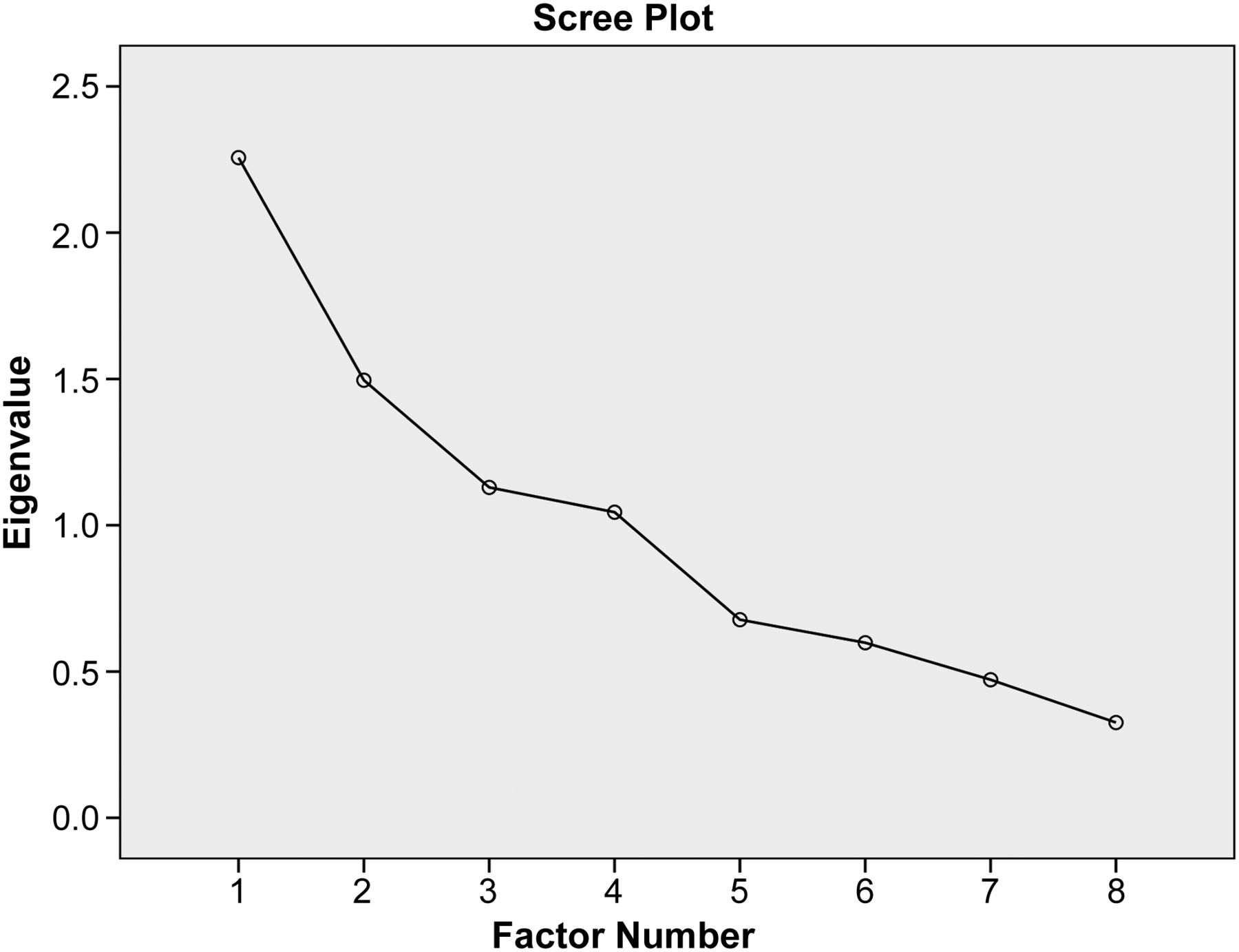
PCA with varimax rotation, commonalities >0.4 and eigenvalues >1 were conducted on the eight triggers. The eigenvalue rises as the proportion of variance explained by a factor increases, and a cut of 1 is often used to identify factors that warrant further consideration. Tests of sampling adequacy (Kaiser–Meyer–Olkin (KMO)), multicollinearity (Bartlett test of sphericity p<0.05) and residuals were undertaken to check that the triggers were appropriate for PCA. A scree plot was also used to help decide on the possible numbers of components to include. This is a plot, in descending order of magnitude, of the eigenvalues of a correlation matrix. It helps the analyst visualise the relative importance of the factors—a sharp drop in the plot signals that subsequent factors can be ignored.
The triggers comprising each component were used to interpret the meaning of the components. The internal consistency and reliability of the derived factors was assessed with Cronbach's α. Results were considered significant at the 5% significance level (p<0.05).
Results
Demographics
Sixty-two patients were included in the final analysis, with an average age of 67.3 years (range 22–87 years), 50% (n=31) were female and they were all white British. Four cases were excluded due to insufficient information and one patient with PD was under the palliative care service due to rapidly progressing malignancy and not their PD, and were therefore excluded.
The diagnoses across the sample are presented in table 2, with 72.6% of the sample having a diagnosis of either PD, a Parkinson's plus syndrome (PPS) or MS. In terms of comorbidities, 11 (17.7%) patients had a past medical history of malignancy, 3 (4.8%) end-stage respiratory disease unrelated to their neurological condition, 4 (6.5%) were arteriopaths and 3 (4.8%) had a diagnosis of heart failure. Four (6.5%) patients had a history of venous thromboembolism and one haemochromatosis.
Time from diagnosis to death and time under follow-up by the palliative care team
Follow-up
Table 2 illustrates the time from diagnosis to death and follow-up time under the SPNS for the different diagnoses. Patients with MS, in our group, lived on average for 16.7 years, those with PD or PPS survived for 5.9 years and patients with MND lived on average for 1 year. The follow-up time under the SPNS was longer for the MS patients, average 2.7 years, followed by PD/PPS (1.5 years) and Huntington's Disease patients (1.2 years). Patients with MND had a shorter follow-up of 6 months. Across diagnoses, the median follow-up time was 336 days (range 2–2960 days).
Triggers and PCA
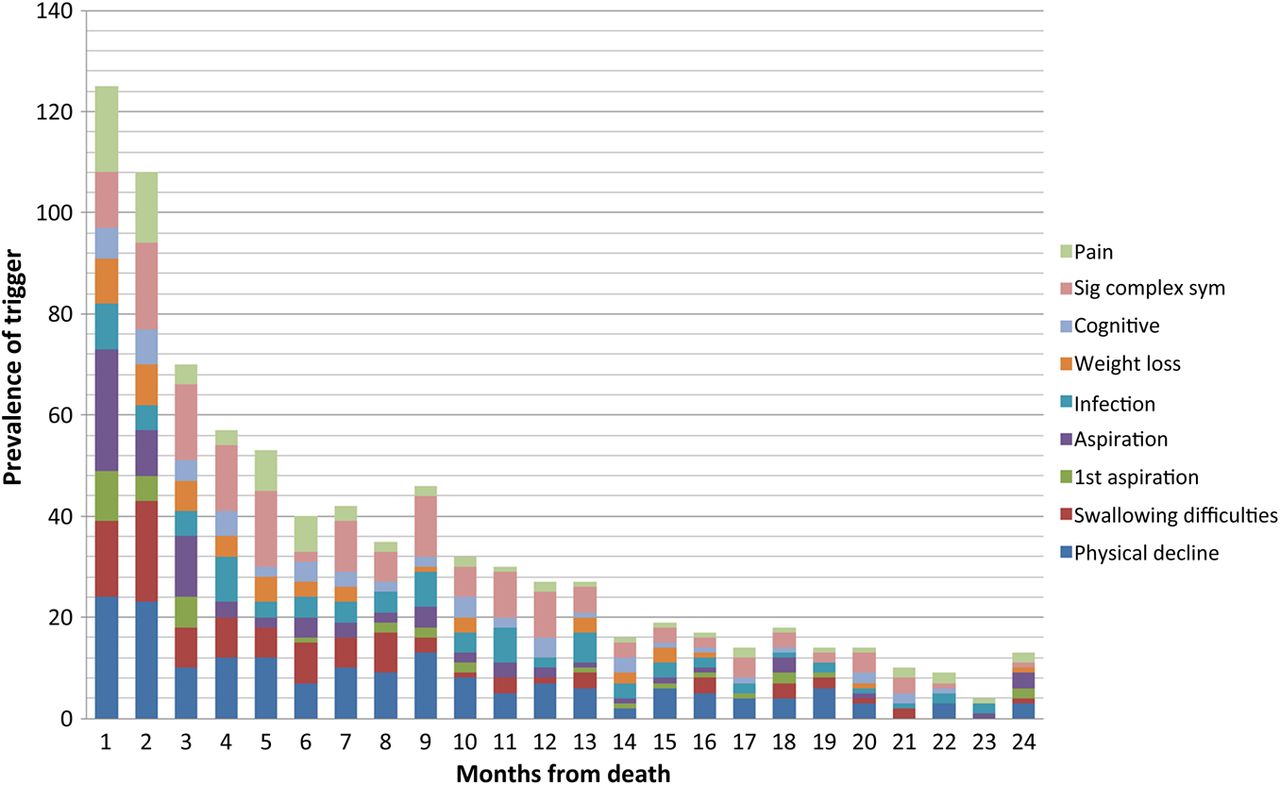
The frequencies of the triggers over the follow-up period are presented in table 3. These include the first episode and subsequent episodes of deterioration for each of the triggers. The commonest trigger across diagnoses was decline in physical function (episodes=217), followed by significant complex symptoms (episodes=178) and swallowing difficulties (episodes=110). Both infection (all infections except aspiration) and aspiration were common with 99 and 90 episodes, respectively. The least frequent triggers documented were cognitive impairment (episodes=70) and weight loss (episodes=55).
Total frequency of triggers during the follow-up period for all participants
Figure 2 illustrates the prevalence of triggers according to the time from death. This shows a trend suggestive of an increase in the number of triggers as the cohort got closer to death, implying the triggers do characterise the progression of the disease. PCA was conducted on the triggers for patients who were under the care of the SPNS for the entire last 6 months of their life. The KMO measure verified the sampling adequacy for the analysis (KMO=0.6). Bartlett's test of sphericity χ2=66.2, p<0.0005, indicated that correlations between items were sufficiently large for PCA. An initial analysis was run to obtain eigenvalues for each component of data. Four components have eigenvalues over Kaiser's criterion of 1, and in combination explained 76.8% of the variance. The scree plot (figure 3) also suggested a model of four components. Table 4 shows the factor loadings after rotation. The triggers that cluster on the same components suggest that component 1 represents rapid physical decline, accounting for 26.7% of the variance and included physical decline, swallowing problems and weight loss. Components 2–4 only loaded significantly onto 2 items, so have to be interpreted with caution. Component 2 accounted for 19.8% of the variance and included significant complex symptoms and pain. Component 3 accounted for 16.6% of the variance and included infections and cognitive decline. Component 4 accounted for 13.7% of the variance and included swallowing and aspiration. The internal reliabilities of the four components, calculated using Cronbach's α were however not very high, ranging from 0.4 to 0.6; this may reflect the small sample in this preliminary study.
Summary of principle component analysis results for the eight triggers

Frequency of triggers according to months prior to death.

{kind=link}
{kind=link}
{kind=link}
Scree plot.
Management of terminal phase
The documented cause of death, either on the death certificate or in the medical records, was aspiration pneumonia or pneumonia in 56.5% (n=35) of the sample. Global deterioration was apparent in 11.3% (n=7) cases; 4.8% (n=3) died suddenly and unexpectedly from respiratory failure, and 3.2% (n=2) were documented as dying following an episode of sepsis, with 6.4% dying of other causes. In terms of place of death, 31% died at home, 24% in a hospice, 26% in hospital and 16% in care homes.
The dying phase was recognised in 72.6% (n=45) cases. This was not the case in 11.3% (n=7) of cases although there was missing data in 16.1% (n=10) of the sample. In 61.3% (n=38) there was documented evidence that the dying phase was well managed, including management of symptoms and psychosocial distress, including carer distress. In 8.1% (n=5) of cases, this was not the case, and in 30.6% (n=19), there was insufficient data to formulate a judgement.
The duration of the dying phase was, on average, 8.8 days across diagnoses, with MS patients dying over a period of 14 days on average, PD/PPS patients over 8.7 days, MND patients 11.8 days and HD 4.3 days. The commonest symptoms during the terminal phase were documented to be: reduced level of consciousness 56.5% (n=35), symptoms of septicaemia 51.6% (n=32), respiratory secretions 46.8% (n=29), breathlessness 45.2% (n=28), pain 25.8% (n=16) and delirium 24.2% (n=15). The LCP was used in 33.9% (n=21); it was not used in 40.3% (n=25) cases, and there was missing data in 25.8% (n=16) cases. Bereavement support, in the form of an initial phone call and, if required, face-to-face meetings thereafter, was offered to 100% of carers and taken up by 95.2% (n=59).
Discussion
This is the first study assessing the prevalence and components of the triggers proposed by the NEoLCP expert panel to predict the palliative phase in patients with ANC. This study also assessed if there was evidence to support that dying was recognised in patients with ANC under the SPNS, and managed well. Patients experienced an array of complex physical and social problems and many had significant comorbidities including malignancy, suggesting a multidisciplinary, holistic approach is necessary for this group.
The length of time from diagnosis to death in our sample was consistent with known epidemiological data, implying the findings can be generalised.9–11 Importantly, the median follow-up time under the SPNS was less than 1 year (336 days) indicating that this service is accepting patients at an appropriate time for palliative care to be involved (table 2). Although one MS patient was under the service for 8 years, this individual had complex psychosocial needs requiring episodic palliative care input.
Physical decline was the most common trigger in patients with ANC (217 episodes) followed by significant complex symptoms (178 episodes) (table 3). As expected, the numbers of episodes of swallowing difficulties (110 episodes) were similar to the number of aspiration episodes (90 episodes). The number of non-aspiration infections also had a high frequency (99 episodes). Although cognitive decline and weight loss are typically gradual in nature, they were recorded as ‘episodes of evidence’. Thus, in the case of cognitive decline there were 70 episodes, and 55 episodes of weight loss. The fewer documented episodes of these two triggers may reflect a lack of formal assessment and documentation rather than lack of occurrence. It is increasingly recognised that cognitive impairment is more prevalent and occurs at earlier stages of degenerative neurological conditions than previously thought. Specific and sensitive identification of cognitive impairment may require specialist assessment to detect it in its early stages.12 ,13
Figure 2 demonstrates that as time to death decreased the total number of triggers increased. This may indicate that the triggers characterise the terminal deterioration of the patients in this study and could act as predictors of the palliative phase in ANC. Further data is now required to determine this. The PCA suggested that 76.8% of the data variance could be explained by four components (table 4). Component 1 included decline in physical status, swallowing problems and weight loss. This inter-relationship is logical, as both swallowing and weight loss are also evidence of decline in physical status, however, the key feature seemed to be the rate of decline; thus, component 1 represents ‘rapid physical decline’. Component 2 accounted for 19.8% of variance and included significant complex symptoms and pain. On further consideration, pain in this patient group does represent a significant complex symptom, thus the definition of the component was extended to include pain (‘significant complex symptoms, including pain’). Component 3 represented recurrent infections and cognitive decline. The relationship between these two components is difficult to explain and may be a result of the increased susceptibility to infection of patients with cognitive impairment due to impaired communication, insight and possible compliance to treatment. At this stage, without further data, we can only speculate about this association. Component 4 accounted for 13.7% of the variance and included swallowing and aspiration, which we would expect to be correlated, and together represent ‘risk of aspiration’.
Although our sample met the criteria for PCA, it is too small for this type of analysis to provide a stable component solution;14 ,15 this is reflected in the weak internal reliability with Cronbach's α ranging from 0.4 to 0.6. Nonetheless, the components did measure a large proportion of the variation in the data and the identified components had logical inter-relationships. Our results, therefore, suggest that the triggers may possibly be reduced to four triggers, however, further prospective data are necessary to validate this.
As over half the sample died from aspiration pneumonia or pneumonia (56.5%), this is an important finding in improving the recognition of dying, which occurred in only 72.6% of cases. Recognition that pneumonia could herald a terminal event should act as a prompt to prepare patients and loved ones for dying, and crucially ensure future care and end-of-life wishes are sensitively explored and communicated.3 There are several papers across neurological diagnoses that suggest the gradual progressive nature of such conditions, and the common causes of death can facilitate the recognition of the terminal phase in this patient group.16–18 Educating healthcare professionals with regard to the common causes of death, disease trajectories and triggers in these conditions is crucial to improving the recognition of dying and ACP. In 61.3% of cases, there was evidence of good management of the terminal phase, including regular assessment and management of symptoms, discussion with family members and consideration of psychosocial factors.
In 33.9% of cases, the LCP was used, however, this was not the case in 40.3% of cases. All patients who died in the hospice commenced the LCP. Importantly, it was in the hospital and nursing home setting where this did not occur consistently. There was, however, significant missing data in the assessment of management of the terminal event (30.6%), whether dying was recognised (16.1%) and the use of the LCP (25.8%). This highlights the need for systematic collection of such data for ANC patients in order to better understand the range of problems faced and issues related to clinical management of the dying phase regardless of the place of death. Such data may offer valuable clinical guidance to service providers working with people with ANC.
The duration of the terminal phase was, on average, 8.8 days across all diagnoses; admission to a hospice during the terminal event can, therefore, be considered appropriate. The symptoms experienced by the patients were similar to other patient groups, such as those with cancer, where the necessity of palliative care involvement during the terminal phase is well documented.19 This particular SPNS is achieving a high rate of home (31%) and hospice (24%) deaths compared with the national average.20 Bereavement support was offered in all cases, with a high take-up of 95.2%, which is consistent with the high levels of distress experienced by carers of such patients.2
The limitations of this study are primarily a result of the retrospective collection of data and small sample size. The data used was originally collected for another purpose and not all the relevant information was rigorously documented. Information on each trigger was not assessed in a consistent manner, there is, therefore, the potential of missing data due to poor recording. The data was extracted from narrative clinical note entries, although these accounts did provide rich contextual information.
This study aimed to provide an initial evaluation of the prevalence and components of the triggers recommended by the NEoLCP to indicate that a patient has entered the palliative phase. Although the data collected related to patients already under the care of the SPNS, it has been possible to establish that the triggers are common and increase in frequency as patients approach death. The majority of the variation in the data could be explained by four components. At this stage, with only a small sample and retrospective data, we recommend that data on all eight triggers continue to be collected in order to produce robust validation through prospective studies. However, the four components deduced through the PCA do have face validity, although the relationship between infection and cognitive impairment remains unclear. Future studies should also focus on collecting data relating to the triggers prior to referral to palliative care services, and importantly whether the triggers and components predict survival. Validated measures of early cognitive dysfunction also need to be used.
Our results suggest that through clearly defined referral criteria based on the NEoLCP triggers, patients with ANC can access specialist palliative care services at an appropriate stage of their illness. Prompt identification of the need for palliative care in ANC can ensure that the needs and preferences of those affected are heard and responded to with compassion and respect for the individual behind the disease. Through further validation of the triggers suggested by the NEoLCP, robust referral criteria can be produced; thus enabling this vulnerable group to access timely specialist palliative care, without overwhelming services.
References
Footnotes
-
Competing interests None.
-
Ethics approval NHS research ethics committee approval was not required for this secondary use of anonymised data collected as part of service development in accordance with the National Research Ethics Service guidance. No additional burdens or risk were imposed on participants.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement JH has access to the full dataset.