Article Text

Statistics from Altmetric.com
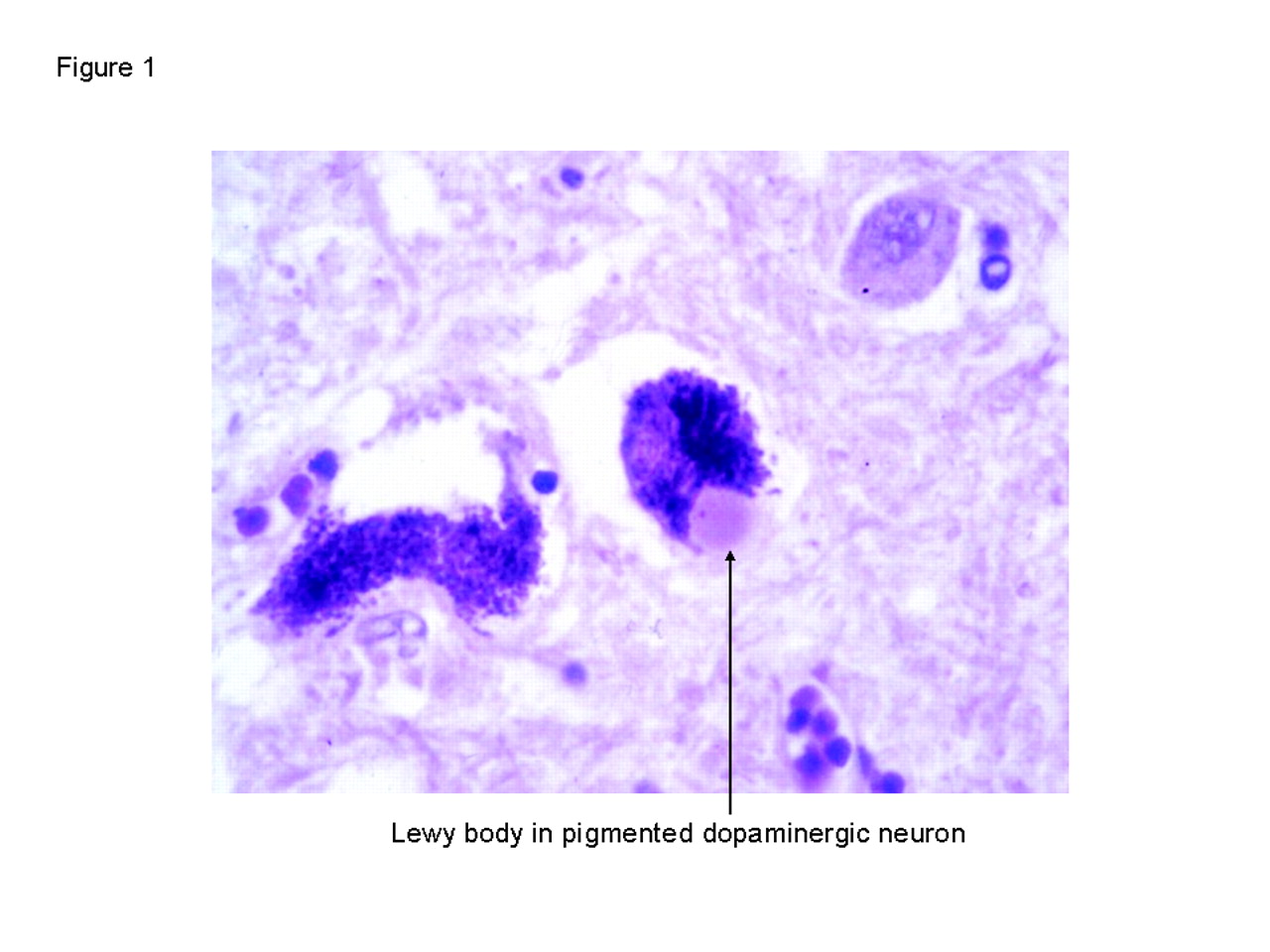
Making the diagnosis of Parkinson’s disease (PD) is a common clinical situation faced by neurologists, geriatricians, and general physicians. In the UK, about 30 to 40 patients are diagnosed with PD every day.1 However, the diagnosis is not always easy. The diagnostic reference standard for idiopathic PD is still histopathology, based on the loss of dopaminergic neurons in the substantia nigra, with Lewy bodies in the surviving neurons (fig 1).2 But clearly any reference standard that requires postmortem examination is not very helpful to a clinician faced with a living patient. Unfortunately, there is no antemortem equivalent of the Lewy body.
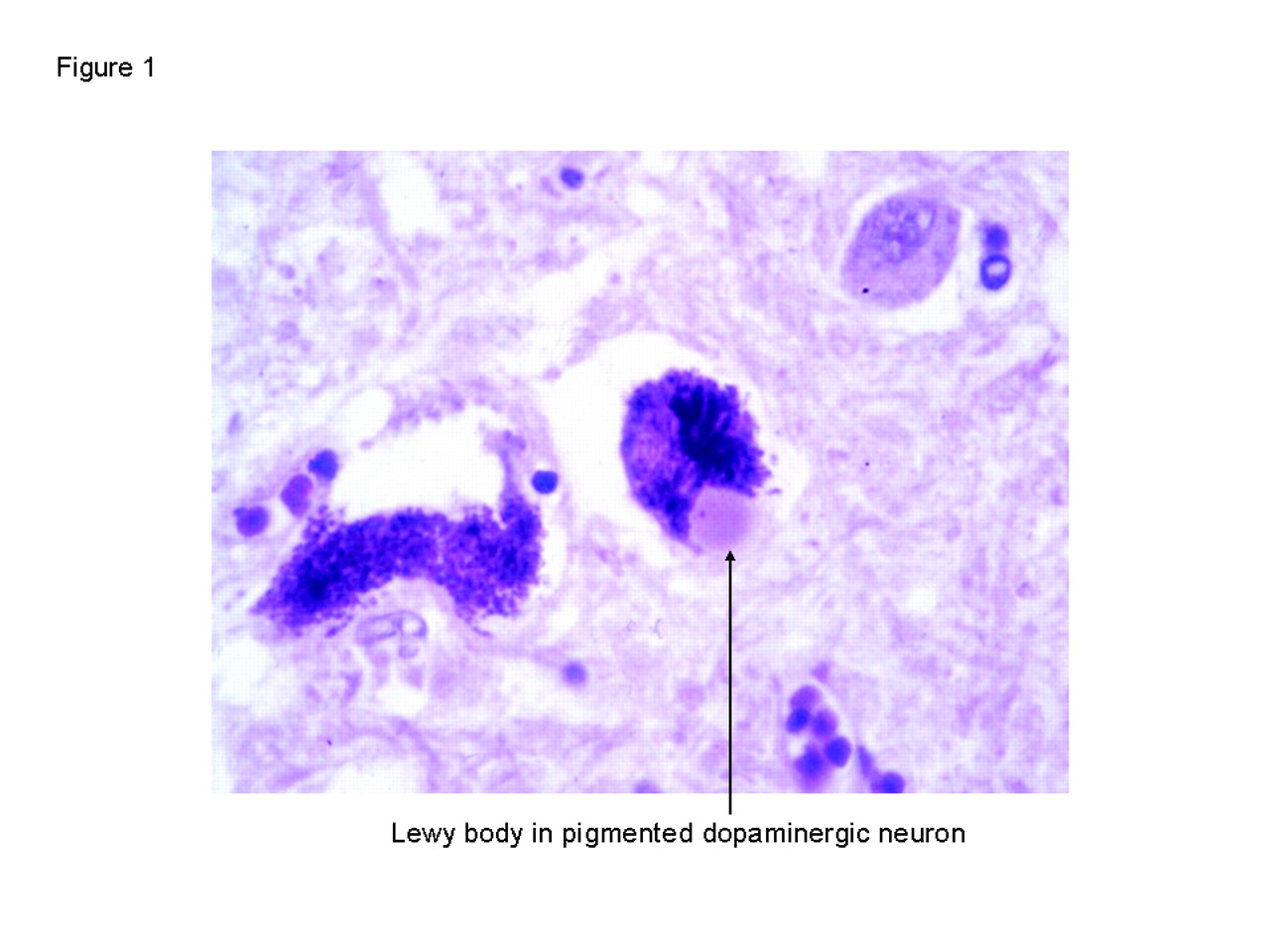
Lewy body (arrow): haematoxylin & eosin stain, original objective magnification ×40 (courtesy of Dr James MacKenzie).
The diagnosis, therefore, remains a clinical one in which laboratory and radiological investigations play only a small part. Clinicians must rely on interpreting a combination of clinical features, their onset, symmetry, progression, and response to treatment. This diagnostic process is subjective and so, unsurprisingly, is liable to error; two hospital based studies in the early 1990s found that only about three quarters of patients with a final clinical diagnosis of PD had it confirmed at postmortem (fewer when the clinical diagnosis at presentation was considered).3,4 Although more recent studies suggest that the accuracy of diagnosis has improved, to perhaps 90% or more,5,6 these came from highly specialised units, which may not be representative of most departments that see parkinsonian patients.
Several attempts have been made to improve diagnostic accuracy by developing better clinical criteria for parkinsonism and PD. Two of the most commonly used are the UK Parkinson’s Disease Society (PDS) Brain Bank criteria,2 and the Gelb criteria7 (see boxes 1 and 2). These may improve the accuracy of the diagnosis of PD, but as criteria become stricter up to 35% of true pathologically proven PD may be excluded.8 Therefore, although strict diagnostic criteria are helpful in research, they are not always appropriate in clinical practice where it is important not to miss patients with definite PD.
BOX 1 UK Parkinson’s Disease Society Brain Bank clinical diagnostic criteria2 for Parkinson’s disease
Step 1: Diagnosis of a parkinsonian syndrome
-
Bradykinesia (slowness of initiation of voluntary movement with progressive reduction in speed and amplitude of repetitive actions)
-
and at least one of the following:
-
- muscular rigidity
-
- 4–6 Hz rest tremor
-
- postural instability not caused by primary visual, vestibular, cerebellar, or proprioceptive dysfunction
Step 2: exclusion criteria for Parkinson’s disease
-
History of repeated strokes with stepwise progression of parkinsonian features
-
History of repeated head injury
-
History of definite encephalitis
-
Oculogyric crises
-
Neuroleptic treatment at onset of symptoms
-
More than one affected relative
-
Sustained remission
-
Strictly unilateral features after three years
-
Supranuclear gaze palsy
-
Cerebellar signs
-
Early severe autonomic involvement
-
Early severe dementia with disturbances of memory, language, and praxis
-
Babinski’s sign
-
Presence of cerebral tumour or communicating hydrocephalus on CT scan
-
Negative response to large doses of levodopa (if malabsorption excluded)
Step 3: Supportive criteria for Parkinson’s disease (three or more required for diagnosis of definite Parkinson’s disease)
-
Unilateral onset
-
Rest tremor present
-
Progressive disorder
-
Persistent asymmetry affecting side of onset most
-
Excellent response (70–100%) to levodopa
-
Severe levodopa induced chorea
-
Levodopa response for five years or more
-
Clinical course of 10 years or more
BOX 2 Gelb criteria7 for Parkinson’s disease
Grouping of clinical features according to diagnostic utility
Group A features: characteristic of PD
-
Resting tremor
-
Bradykinesia
-
Rigidity
-
Asymmetric onset
Group B features: suggestive of alternative diagnoses
-
Features unusual early in the clinical course
- Prominent postural instability in the first three years after symptom onset
- Freezing phenomena in the first three years
- Hallucinations unrelated to medications in the first three years
- Dementia preceding motor symptoms or in the first year
-
Supranuclear gaze palsy (other than restriction of upward gaze) or slowing of vertical saccades
-
Severe, symptomatic dysautonomia unrelated to medications
-
Documentation of a condition known to cause parkinsonism and plausibly connected to the patient’s symptoms (such as suitably located focal brain lesions or neuroleptic use within the past six months)
Proposed diagnostic criteria for Parkinson’s disease
Criteria for POSSiBLe diagnosis of Parkinson’s disease
At least two of the four features in Group A are present; at least one of these is tremor or bradykinesia
and
either none of the features in Group B is present
or symptoms have been present for less than three years, and none of the features in Group B is present to date
and
either substantial and sustained response to levodopa or a dopamine agonist has been documented
or patient has not had an adequate trial of levodopa or dopamine agonist
Criteria for PROBABLE diagnosis of Parkinson’s disease
At least three of the four features in Group A are present
and
none of the features in Group B is present (note: symptom duration of at least three years is needed to meet this requirement)
and
substantial and sustained response to levodopa or a dopamine agonist has been documented
Criteria for DEFINITE diagnosis of Parkinson’s disease
All criteria for POSSIBLE Parkinson’s disease are met
and
histopathological confirmation of the diagnosis is obtained at autopsy
WHY IS IT IMPORTANT TO GET THE DIAGNOSIS RIGHT?
Making the correct diagnosis is important to guide management and predict prognosis for the patients and their families, as well as to ensure accurate conclusions in research studies. And, when more disease-specific therapies eventually become available (particularly neuroprotective agents), early as well as accurate diagnosis will be even more important.
In this article we will outline a practical step-by-step approach to the diagnosis of PD, highlighting some of the pitfalls to be avoided by experienced and inexperienced clinicians alike:
-
The first step is to establish whether or not the patient has a parkinsonian syndrome.
-
If they do, the next step is to clarify the cause, first by identifying atypical features that make PD less likely, and second by identifying supportive features that make PD more likely.
DOES THE PATIENT HAVE PARKINSONISM?
This question is answered by looking for the four cardinal motor features of parkinsonism—bradykinesia, rest tremor, rigidity, and postural instability.
Bradykinesia, or slowness of movement, is recognised on examination by impairment of repetitive movements such as finger or foot tapping. Characteristically, in true bradykinesia, these movements are not only slow, but their speed and amplitude diminish as the patient continues, and the rhythm of the movement is broken up. However, it can be difficult to assess in some patients (for example, those with severe tremor) and it can occasionally be mimicked by cortical deficits of the hand (for example, occasional patients with motor neuron disease are initially labelled parkinsonian).
Parkinsonian tremor is characteristically a low frequency (3–5 Hz) rest tremor of the hands, legs, lips, or jaw, which is usually attenuated when the patient uses the affected body part. There is often an associated postural tremor which occasionally is more prominent than the rest tremor but there is rarely a marked kinetic tremor.9,10 The rest tremor may be exacerbated by mental exertion (for example, mental arithmetic) and the hand tremor may also be prominent when the patient is walking (dependent tremor).
Rigidity is characteristically felt equally throughout the range of passive movement of a body part (like bending a “lead pipe”) and may affect the limbs and the axial muscles. Where tremor-like activity is superimposed on rigidity the term “cogwheel rigidity” is used, although the frequency of cogwheeling (6–9 Hz) is different from the frequency of the rest tremor. Rigidity in a limb may be increased by active movement of the opposite limb (coactivation). Therefore, in a patient with apparently normal tone at rest, significant rigidity may be identified by re-examining tone while the patient performs a repetitive movement of the opposite limb.
Postural instability should only be attributed to parkinsonism if it is unexplained by other medical problems (such as blindness or peripheral neuropathy). It is tested by the pull test for retropulsion in which a sudden backwards pull is applied to the shoulders while the patient is standing. This can be done in various different ways11 but is most valid when performed without warning when more than two corrective steps are considered abnormal.12 But giving no warning can distress patients and we prefer to warn the patient first.
The clinical diagnosis of parkinsonism requires the presence of at least two of the four cardinal features. The UK PDS Brain Bank criteria are more specific, and require the presence of bradykinesia, as well as at least one of the other three features.
CONDITIONS MIMICKING PARKINSONISM
Two groups of non-parkinsonian syndromes may be confused with parkinsonism:
-
tremor disorders (most commonly essential tremor)
-
primary gait disorders (most commonly the higher level gait disorder often presumed to be secondary to cerebrovascular disease).
Essential tremor
Diagnostic confusion between parkinsonism and essential tremor may arise for two reasons. Firstly, although essential tremor is characterised by a tremor that is exacerbated by posture-holding and action, these patients may also have a tremor at rest,13,14 whereas parkinsonian patients may also have a postural tremor.
Secondly, although the other cardinal features may be discriminating, some essential tremor patients do have mild rigidity,15 whereas some patients with early PD may present with an isolated rest or postural tremor without any other features of parkinsonism. A recent study described 13 patients with a late onset, markedly asymmetrical postural tremor that was diagnosed initially as essential tremor but who went on after many years to develop typical PD according to UK PDS Brain Bank criteria.16
In practical terms, confusion is usually avoided by observing whether the tremor is worse at rest or with posture or action (patients with PD rarely spill a glass of water when asked to take a drink), and careful examination for the other features of parkinsonism. Additionally, a tremor of the head (as opposed to the jaw) suggests a non-parkinsonian tremor. Finally, caution should be applied when diagnosing essential tremor in a patient where the postural tremor is unilateral. When in doubt, follow up is crucial as those with PD will eventually progress to develop clear parkinsonian features.
Higher level gait disorders
Higher level gait disorders, which can be idiopathic or associated with conditions such as cerebrovascular disease or normal pressure hydrocephalus, may be misdiagnosed as parkinsonism.17–19 Although it may share certain features with a parkinsonian gait (for example, a short shuffling stride with gait freezing and postural instability), a higher level gait abnormality often has a broad base rather than the typical narrow base of parkinsonism, and there are no other cardinal features of parkinsonism. In particular, patients do not have lower limb bradykinesia so that, despite a severe disturbance of gait, they will usually be able to move their legs normally when they are not weight bearing (for example, imitating a cycling motion). It is, therefore, inappropriate to say that they have lower-half parkinsonism (this should be reserved for those who fulfil the criteria for parkinsonism, many of whom will have vascular parkinsonism—see later). The diagnosis of PD should never be made on the basis of a parkinsonian-type gait alone.
Problems making the diagnosis in the frail elderly
The combination of increasing frailty and comorbidity can make the diagnosis of parkinsonism difficult in older people. Indeed, subtle extrapyramidal signs, which do not meet the criteria for full parkinsonism, have been reported in about one third of people aged over 65 years.20–22 These signs are not unimportant, because they are associated with functional disability,20 dementia,23 and increased mortality.20,22 Although some of these people may be in the early phase of PD, this is unlikely to be the case in the majority (unless postmortem series have dramatically underestimated the prevalence of Lewy body pathology in the elderly). However, these subtle signs in so many people do make the diagnosis of parkinsonism more difficult in older people. Clues to the correct diagnosis are to differentiate true bradykinesia from simple slowness, and to interpret the examination findings in the context of a person’s age, general condition, and any comorbidities.
The diagnosis of PD should never be made on the basis of a parkinsonian-type gait alone
DOES THE PARKINSONIAN PATIENT HAVE PARKINSON’S DISEASE?
Once the patient is confirmed to have parkinsonism, the next stage is to decide whether he or she has PD—or not. The UK PDS Brain Bank criteria recommend two steps: firstly to identify any atypical features that make the diagnosis of PD unlikely (table 1), and secondly to identify supportive features that make the diagnosis of PD more likely (table 2).
Features suggestive of diagnoses other than Parkinson’s disease
Features suggestive of Parkinson’s disease
CAUSES OF PARKINSONISM NOT DUE TO PARKINSON’S DISEASE, AND FEATURES THAT SUGGEST THEIR DIAGNOSIS
Drug induced parkinsonism
Many drugs can cause parkinsonism, most commonly antipsychotics and anti-emetics, more rarely others such as methyldopa, calcium antagonists, and sodium valproate. Before making the diagnosis of PD, therefore, it is important to check the patient’s medication (both current and previous). If the patient is on a relevant drug, it should be stopped where possible, and the patient followed up. Drug induced parkinsonism can take several months to resolve after the drug is stopped (box 3). And even if the symptoms do improve, follow up has shown that a few of these patients will later develop PD, suggesting that the drug had unmasked subclinical PD.24 If the drug cannot be stopped, it can be very difficult to distinguish drug induced parkinsonism from idiopathic PD, although drug induced parkinsonism may be more likely to be bilateral and symmetrical at onset.25 In this situation, functional imaging with a dopamine transporter ligand (see below) may be useful, because patients with pure drug induced parkinsonism have normal scans.26
BOX 3 Case summary: drug-induced parkinsonian
An elderly lady presented with a “shuffling” gait. She was taking trazodone for depression, as well as sodium valproate 400 mg twice daily and prochlorperazine 5 mg three times daily for chronic migraine. On examination she had reduced facial expression as well as mild rigidity and bradykinesia in her arms and legs. There was no tremor. Her gait was abnormal with a short stride, narrow base, and reduced arm swing bilaterally. She had retropulsion on the pull test, and would have fallen if not supported.
Her prochlorperazine and sodium valproate were both stopped. At review two months later she was no better, and so an FP-CIT scan was arranged. This was normal, supporting the clinical impression of drug induced parkinsonism. Five months later she was much improved with normal facial expression, and no rigidity or upper limb bradykinesia. Although her gait remained a little slow, it was otherwise normal and there was no retropulsion.
Clinical impression
Moderately severe symmetrical parkinsonian syndrome without tremor.
Diagnosis
Probably drug induced parkinsonism but will continue to be followed up.
Learning points
-
The effects of drug induced parkinsonism may persist for several months after stopping the drug.
-
An FP-CIT scan may help differentiate between drug induced parkinsonism and parkinsonism associated with degeneration of the striatonigral neurons.
Vascular parkinsonism
Basal ganglia infarcts rarely cause parkinsonism, but diffuse cerebrovascular disease does. These patients often have vascular risk factors and previous strokes or transient ischaemic attacks, and on examination may have upper motor neuron signs and cognitive deficits. The parkinsonism may be symmetrical and more prominent in the lower compared to the upper body, and lacks the typical rest tremor. There may also be a severe gait disorder with a broad (as opposed to a narrow) base, early gait freezing and postural instability, a poor response to levodopa, and rapid or stepwise progression.19,27,28
Progressive supranuclear palsy (Steele-Richardson-Olzewski syndrome)
As suggested by its name, progressive supranuclear palsy (PSP) is characterised by a supranuclear gaze palsy with hypometric or slow saccades, particularly on downgaze (causing symptoms such as difficulty going downstairs or looking at a watch). However, in the early stages, these abnormalities are often absent,29 and occasionally they do not develop at all. Other features that should prompt the clinician to consider this diagnosis are eyelid dystonia (difficulty with eye opening), early gait disturbance with falls (particularly backwards) in the first year, pseudobulbar dysarthria, and symmetry of the parkinsonian features. Additionally, although PSP patients may have tremor, it is often bilateral and postural rather than the typical resting tremor. As the disease progresses, a poor or unsustained response to levodopa, fast progression (symptom onset to death about six years), and the development of cognitive dysfunction are all suggestive of PSP.29,30 However, it has recently been observed that approximately one third of cases of pathologically proven PSP may be clinically very similar to PD31 and can only be diagnosed accurately at postmortem.
Multiple system atrophy (Shy-Drager syndrome, striatonigral degeneration)
The presence of early severe autonomic dysfunction (such as urinary incontinence, severe constipation, symptomatic postural hypotension, erectile dysfunction, and cold dusky extremities) should suggest this diagnosis (box 4).32 Other useful pointers include cerebellar and upper motor neuron signs, stridor due to laryngeal dystonia, a characteristic high pitched dysarthria, and severe antecollis (chin on the chest). The tremor in multiple system atrophy (MSA) can be a typical parkinsonian rest tremor but is more often a jerky postural tremor.33 As in PSP, MSA progresses more quickly than PD (symptom onset to death about seven years), but unlike PSP many patients respond well (at least initially) to levodopa.7
BOX 4 Case summary: probable multiple system atrophy
A man in his 50s presented with three months of progressive upper limb tremor, shuffling gait, postural dizziness, and pain in his neck and shoulders when standing. For several years, he had had vivid dreams, which he acted out in his sleep. On examination, he had a typical parkinsonian rest tremor in the left hand, mild bilateral rigidity and bradykinesia, and reduced arm swing bilaterally on walking. There was a marked postural drop in his blood pressure (from 130/90 to 90/70), but no other atypical features of PD. Over two years of follow up, he developed other features of autonomic dysfunction including urinary frequency, severe constipation, erectile problems, and cold extremities. His parkinsonism progressed with spread of the tremor to the other side and to the legs, and worsening of the rigidity and bradykinesia. Levodopa was started cautiously (in view of the postural hypotension) with a good response.
Clinical impression
Rapidly progressive asymmetrical parkinsonian syndrome with severe autonomic dysfunction, and REM sleep behaviour disorder.
Diagnosis
Probably multiple system atrophy, in view of the prominent early autonomic dysfunction, although PD remains a possibility. The patient and his wife have both given provisional consent to postmortem to confirm the diagnosis.
Learning points
-
Although autonomic dysfunction commonly occurs late in PD, severe dysfunction early in the disease is more suggestive of multiple system atrophy.
-
Pain in the neck and shoulders on standing may be a symptom of postural hypotension
-
REM sleep behaviour disorder is associated with parkinsonian disorders, and may predate their onset by several years.
-
Many patients with multiple system atrophy have a good response to levodopa.
-
Always consider asking the patient about a postmortem, as the diagnosis of a parkinsonian disorder is rarely certain during life.
If dementia predates the onset of parkinsonism or occurs soon after its onset (typically within a year), the diagnosis is DLB but if someone who has had typical PD for several years develops dementia, the diagnosis is PD dementia
Fragile X tremor ataxia syndrome
A syndrome of late onset intention tremor, ataxia, and parkinsonism has recently been described in those who carry the fragile X premutation.34 Although this may resemble MSA, the ataxia and intention tremor predominate to the extent that it is not usually confused with PD.
Corticobasal degeneration
This is characterised by a combination of atypical parkinsonism and higher cortical dysfunction, although one of these often dominates the clinical picture. Although the motor dysfunction is often markedly asymmetrical (like PD), there are usually features of cortical dysfunction not seen in PD such as dyspraxia, myoclonus, or cortical sensory loss, which when severe may lead to an “alien limb”. The higher cortical dysfunction may present as dementia or dysphasia.35
Dementia with associated parkinsonism
Dementia with Lewy bodies (DLB) is characterised by parkinsonism associated with early dementia. It has clinical and pathological similarities to PD, and both may simply be part of a spectrum of Lewy body disease since many patients with PD develop dementia over time. Currently the diagnostic distinction between DLB and PD dementia is made on temporal grounds: if dementia predates the onset of parkinsonism or occurs soon after its onset (typically within a year), the diagnosis is DLB but if someone who has had typical PD for several years develops dementia, the diagnosis is PD dementia.36 In both, the dementia is characterised by frontal and visuospatial dysfunction (with initially relatively spared memory) and shows marked fluctuation. Recurrent visual hallucinations (often of people or animals) are common. The associated parkinsonism in DLB can be indistinguishable from that of PD, but sometimes it is more axial with prominent postural instability and less obvious tremor. The diagnostic criteria also include several suggestive (for example, marked sensitivity to neuroleptic medication) and supportive features (for example, unexplained blackouts).36
Other dementia disorders, such as Alzheimer’s disease and frontotemporal dementia, can be associated with parkinsonian features (mainly rigidity and bradykinesia), especially late in the disease course.37 A resting tremor, however, is rare37 and should prompt reevaluation of the diagnosis. The clinical assessment of these patients may be difficult due to lack of cooperation and because they may be on antidopaminergic drugs such as phenothiazines or atypical antipsychotics to manage their behaviour. Moreover, because PD is relatively common in older people, some patients with Alzheimer’s disease may go on to develop coexistent PD, although the presence of dementia would prevent them from being classified as such by existing research criteria
Structural lesions
Structural lesions of the basal ganglia (such as tumours or infarcts) can rarely cause contralateral parkinsonism. Hydrocephalus (including normal pressure hydrocephalus) can cause symmetrical parkinsonism usually without rest tremor.38,39 Therefore, atypical features such as raised intracranial pressure, cognitive problems, a bizarre gait, or persisting, strictly unilateral symptoms and signs suggest the need for structural imaging of the brain.
Functional parkinsonism
Functional or “psychogenic” parkinsonism is well recognised but rare.40 Clues to the functional nature of a movement disorder are an abrupt onset, distractability and inconsistency, selective disability, entrainment of tremor, and a previous history of psychogenic illness.41 If there is doubt about this diagnosis, careful follow up and functional imaging (see below) may resolve the uncertainty.
Young onset parkinsonism
In recent years, several genetic mutations causing parkinsonism have been identified particularly, although not exclusively, in those with young onset (under 40 years) disease. The syndromes may resemble sporadic idiopathic PD both clinically and pathologically. A detailed review of the genetics of PD is beyond the scope of this article (see Morris42) as is the discussion of whether such genetic syndromes should be called PD at all. However, young age of onset and a family history of parkinsonism are clues to an inherited form of PD (although there may be no family history in autosomal recessive cases), while certain clinical features may also be helpful such as early leg dystonia in those with parkin mutations.43
Other conditions to be considered in patients with young onset parkinsonism are Wilson’s disease, Huntington’s disease, and dopa-responsive dystonia.
CHARACTERISTIC FEATURES SUGGESTIVE OF PARKINSON’S DISEASE
Certain clinical characteristics support the diagnosis of PD in a parkinsonian patient:
-
The onset of PD is asymmetrical (often unilateral) in approximately 75% of patients7 and it often remains asymmetrical as the disease progresses.
-
A rest tremor is the commonest initial symptom (in approximately 70% of patients).44 It usually affects the hand, but a typical tremor in the leg is particularly suggestive of PD.
-
Initially the gait may be fairly normal, perhaps just with reduced arm swing on the affected side, but as the disease progresses the gait becomes increasingly abnormal with short shuffling steps, a narrow base and flexed posture.
-
The motor features (especially the rigidity and bradykinesia) of PD respond well to levodopa or dopamine agonists in 90% of pathologically proven cases.45 A small number of people with early PD respond so well to treatment that they have no residual signs, which makes diagnosis difficult if they are first seen on treatment. In this situation, reducing the dose will often clarify the situation. Most patients with early PD notice significant benefit from relatively small doses of levodopa (for example, 300 mg per day) but a few patients need much higher doses. In general, patients should not be regarded as definite non-responders to treatment unless they have tried up to 1000 mg levodopa per day although many develop adverse effects before this dose. Moreover, because dopaminergic treatment can take several months to reach its maximum effect, some patients do not recognise a response until they are taken off treatment because of the mistaken belief that it has not been effective. The gradual build up of a beneficial effect is one of the reasons that acute challenge with levodopa or apomorphine is not recommended as a diagnostic test.46 It also carries some risk (for example, significant hypotension) and can be positive in other parkinsonian disorders (for example, MSA). Some response to dopaminergic treatment is maintained throughout the course of the disease although in patients with very advanced disease this may not result in worthwhile functional improvement.
-
With time, drug related complications, such as dyskinesias, motor fluctuations, and visual hallucinations, are more likely to occur in PD than in other causes of parkinsonism (except dementia with Lewy bodies).
-
The disease progresses slowly over years (median survival is over 10 years from onset) with gradual worsening of the motor features; rapid progression should prompt consideration of an alternative diagnosis.
-
Patients with PD rarely need a wheelchair within three years of onset unless they have other comorbidity.
-
Late features of PD, typically occurring after several years, include postural instability with falls, autonomic dysfunction, and dementia.
Most patients with early PD notice significant benefit from relatively small doses of levodopa
INVESTIGATIONS
Structural imaging
Structural imaging of the brain with CT or MR rarely leads to a definitive diagnosis in parkinsonian patients. Most patients with parkinsonism do not require brain imaging at all. MRI can show evidence of widespread cerebrovascular disease affecting the subcortical white matter or the basal ganglia which may support a diagnosis of vascular parkinsonism, but it must be remembered that “vascular” changes on MRI are common in elderly people without parkinsonism. Although certain MRI appearances have been reported in atypical parkinsonian syndromes,47,48 it is unclear how sensitive and specific these are, particularly in early disease when confusion with PD is most likely.
Functional imaging
Functional radio-isotope imaging techniques such as positron emission tomography (PET) and single photon emission tomography (SPECT) are increasingly being used in parkinsonian syndromes to assist in diagnosis. In the UK, PET is not widely available, but SPECT imaging with a dopamine transporter ligand such as FP-CIT is (costing about £450 per scan). By imaging the binding of this ligand to dopamine transporters on presynaptic nigrostriatal neurones, SPECT can help differentiate parkinsonian syndromes where there is degeneration of these presynaptic neurones (PD, DLB, MSA, PSP, corticobasal degeneration) from syndromes where there is no such degeneration (box 3) (table 3).26
Functional imaging in the differential diagnosis of parkinsonian syndromes
Patients with PD rarely need a wheelchair within three years of onset unless they have other comorbidity
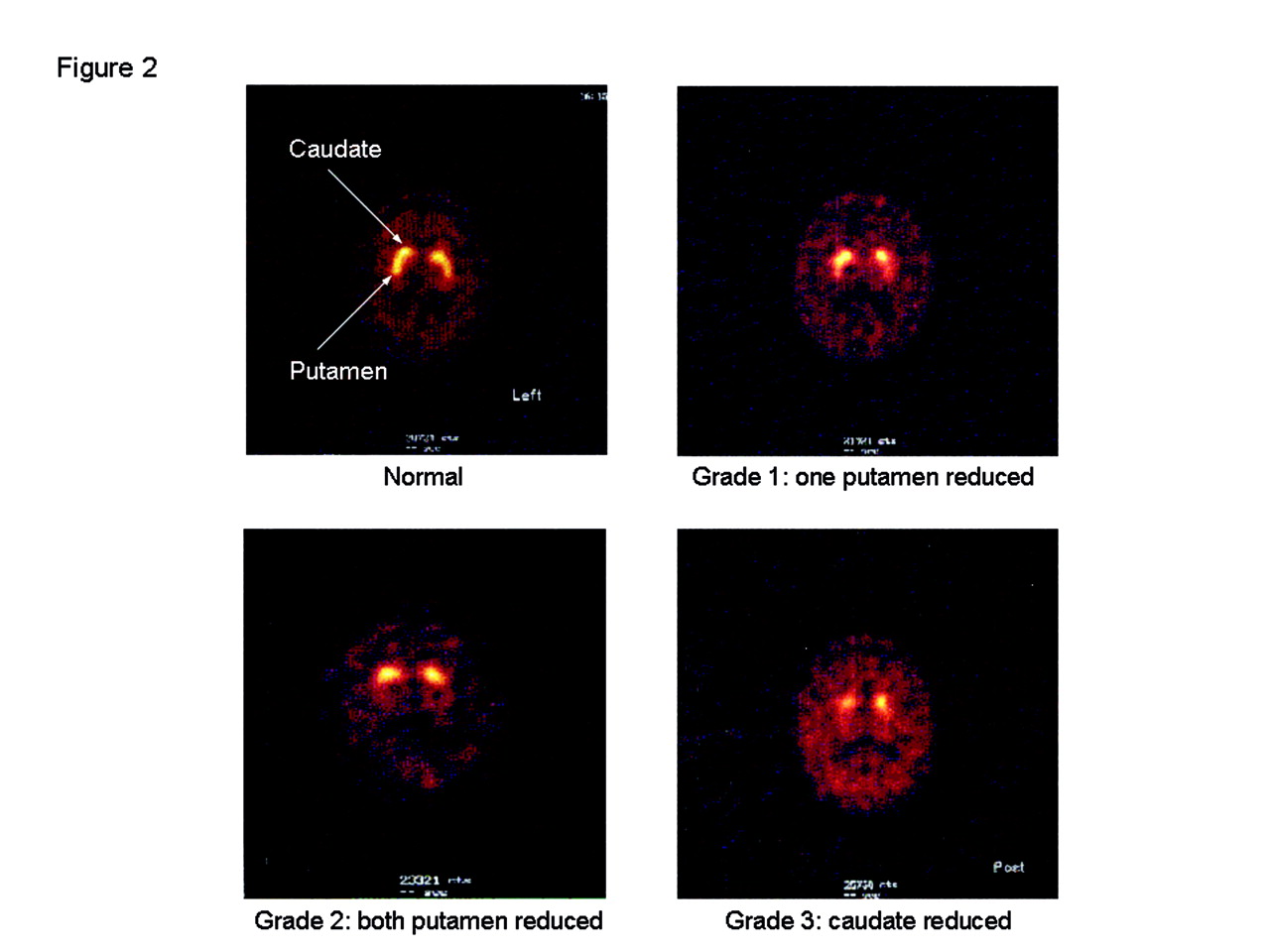
Scans are graded visually depending on the severity of cell loss (fig 2). The scans of patients with parkinsonism associated with presynaptic neuronal degeneration should be abnormal with lower ligand binding and, therefore, less bright uptake on the scan (grades 1 to 3 in fig 2). Typically, in early unilateral PD there is selective loss of nigrostriatal neurons to the putamen on the side contralateral to the clinically affected limb (grade 1 scan). With progression, the degeneration affects both putamen (grade 2) when the clinical signs will often be bilateral before going on to affect the caudate nuclei as well (grade 3), again often with lower uptake contralateral to the clinically worse side. Vascular disease can give atypical scan appearances which do not fit with this pattern (for example, focal loss of uptake in one caudate but not the putamen due to focal infarction).26 Patients with non-parkinsonian syndromes (such as essential tremor) or parkinsonism where there is no presynaptic neuronal degeneration (for example, drug induced) should have normal scans.
{kind=link}
{kind=link}
Visual grading of FP-CIT scans (courtesy of Dr Alison Murray).
Although there is growing consensus that FP-CIT SPECT can be helpful in certain clinical situations, there are few high quality studies that give reliable data on its sensitivity and specificity. Reported sensitivities (87–98%) and specificities (80–100%) are high—but not perfect—for differentiating between parkinsonism with presynaptic degeneration and non-degenerative syndromes, but these figures may be overly optimistic. The studies have often been small, used patients with established disease where there was no diagnostic uncertainty rather than early patients in whom the diagnosis is uncertain (that is, those in whom the test will be most helpful in clinical practice), and incorporated the results of the scan itself into the reference standard (incorporation bias). The ideal reference standard (histopathology) is not practical and clinical diagnosis is prone to error even with strict research criteria, particularly if patients are only followed up for a few months, as is usually the case in such studies.
The lack of a good reference standard makes interpretation of diagnostic studies difficult. For example, in three recent studies 4–14% of patients diagnosed with PD by experienced neurologists had normal PET or SPECT scans.[49] Was this because the clinical diagnosis was wrong or did the scans give false negative results? Finally, clinicians who choose to use FP-CIT SPECT must be aware of what it cannot do—namely distinguish between the different parkinsonian syndromes that are associated with striatonigral degeneration. Hence, it cannot easily tell PD from DLB, MSA, PSP, or corticobasal degeneration. For all of these reasons, at present functional imaging cannot and should not be relied on as a substitute for careful, experienced clinical assessment and follow up.
OTHER DIAGNOSTIC TECHNIQUES
Olfactory function has been proposed as a useful diagnostic sign, because it has been shown (albeit in small studies) to be impaired in about 80% of early PD patients but only 15% of normal controls and those with other forms of parkinsonism such as vascular parkinsonism, MSA, PSP, and corticobasal degeneration.50–52 However, this level of sensitivity and specificity may not be high enough to be helpful in clinical practice, and its value in patients in whom the diagnosis is uncertain has not been tested. It also takes time to perform—the most widely used and best validated test requires the identification of 40 smells, but it can be self-administered. Although olfactory testing is not widely used at present, there may be merit in comparing it formally with FP-CIT SPECT in patients with uncertain diagnoses because it may be just as good as SPECT but cheaper and safer.
CONCLUSIONS
The diagnosis of PD and other parkinsonian syndromes remains clinical. Although frequently straightforward, the process can be difficult and, therefore, requires an experienced clinician and time to establish the pattern of progression and response to treatment. Newer imaging techniques can help the diagnostic process in certain situations but definitive confirmation of the diagnosis still requires postmortem examination.
Functional imaging cannot and should not be relied on as a substitute for careful, experienced clinical assessment and follow up
PRACTICE POINTS
-
Confirm whether or not the patient is parkinsonian.
-
Look for atypical features that make the diagnosis of PD less likely (table 1).
-
Look for typical features that make the diagnosis of PD more likely (table 2).
-
Consider whether functional imaging may be useful (table 3) but be aware of its limitations.
-
Consider whether any other investigations are appropriate (such as structural imaging of the brain).
-
If in doubt keep an open mind and follow the patient up—the diagnosis may become clear with time.
-
If parkinsonian features are troublesome, consider a trial of dopaminergic therapy (the response may help clarify the diagnosis, and you may make the patient better even if the diagnosis eventually turns out not to be PD).
-
Consider asking for a postmortem to confirm or refute your clinical diagnosis.
Acknowledgments
This article was reviewed by Dr Richard Davenport, Edinburgh, UK.
REFERENCES
Other content recommended for you
- Improving the diagnostic accuracy in parkinsonism: a three-pronged approach
- The role of DAT-SPECT in movement disorders
- Parkinson's disease: chameleons and mimics
- A 15-year population-based cohort study of the incidence of Parkinson's disease and dementia with Lewy bodies in an elderly French cohort
- Changes in diagnosis with follow-up in an incident cohort of patients with parkinsonism
- How useful is [123I]β-CIT SPECT in clinical practice?
- Clinical utility of dopamine transporter single photon emission CT (DaT-SPECT) with (123I) ioflupane in diagnosis of parkinsonian syndromes
- Systematic clinical approach for diagnosing upper limb tremor
- Visual hallucinations in the differential diagnosis of parkinsonism
- How valid is the clinical diagnosis of Parkinson's disease in the community?