Article Text

Abstract
Guidance and protocols of end-of-life care have been directed towards the care of patients with cancer. It is possible to extrapolate some of these to people with long-term neurological conditions, but there are obvious differences. Neurological conditions have widely different time courses of progression, making the timing of these discussions challenging. The common issues around end-of-life care include knowing when to start discussions, approaching advance planning, managing common symptoms, diagnosing the dying phase, withdrawing life-sustaining treatments, providing support for family and carers and judging how to involve specialist palliative care teams. End-of-life care needs close collaboration between neurology, specialist palliative care and general practice.
- quality of life
- Parkinson-s disease
- motor neuron disease
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Background
Between 2001 and 2014, the number of deaths from neurological conditions in UK increased by 39%.1 Palliative care is defined as ‘an approach that improves the quality of life of patients and their families facing problems associated with life-limiting illness, through the prevention and relief of suffering by means of early identification and impeccable assessment and treatment of pain and other problems, physical, psychosocial and spiritual’.2
General palliative care would be provided by all those caring for patients with life-threatening illness, ensuring good communication with patients and families, shared decision-making, goal setting and symptom management.3
Specialist palliative care would be provided by teams that would have this as their main activity and have received specialist training.3
Neuro-palliative care is a holistic approach to the care of neurological patients with significant disability, complex needs and a potentially shortened lifespan.4
The UK National Service Framework defines a long-term neurological condition as ‘disease of injury or damage to the body’s nervous system (ie, the brain, spinal cord and/or their peripheral nerve connections) which will affect the individual and their family in one way or another for the rest of their life’.5 Neurologists address diagnosis, modification of disease course and management of symptoms for people with long-term neurological conditions such as Parkinson’s disease, multiple sclerosis and motor neurone disease. During the end-of-life phase of conditions, which in the UK is regarded as the expected last year of life, patients and their families, as well as other care providers, often turn to the neurologists for leadership and guidance.6 7 In this article, we discuss supporting people with long-term neurological conditions during the end-of-life phase.
Identifying the end-of-life phase
The time course of progressive neurological conditions varies widely between and within disorders. While the average survival of patients with motor neurone disease is often 2–4 years from diagnosis, those with conditions such as Parkinson’s disease and multiple sclerosis may live for decades with significant symptoms.8 The unpredictable trajectory of neurological conditions presents a special challenge, especially when choosing the appropriate time to start discussions about the end of life. While patients, their family and carers can have an intimate knowledge of changes in a patient’s condition, they expect healthcare professionals to initiate these conversations. Although ‘end of life’ is defined as the expected last year of life, planning and discussions about it should not be restricted to this specific time frame, especially in long-term neurological conditions, as it is impossible to be accurate about when the last 12 months of life begins. Indeed, conversations around future and end-of-life care can be appropriate from the time of the diagnosis, and so professionals should be prepared to have these conversations; a prime example would be conditions where cognitive decline can be expected.
There are no accurate ways to ‘diagnose’ the point at which someone has only 1 year left to live but various clinical indicators and assessment tools can be incorporated into practice. The Gold Standards Framework suggests using the simple ‘surprise’ question devised by Marie Curie: in this, healthcare providers ask themselves, ‘Would you be surprised if this patient died in the coming 6–12 months?’9 If the answer is ‘No’, this is an opportune time to start to plan for end-of-life care. The Supportive and Palliative Care Indicators Tool, the Gold Standards Framework and the UK End-of-Life Programme give overarching and specific clinical indicators relating to identifying people who are entering into end-of-life phase. These could be used to trigger discussions over end of life (box 1).10–12
Indicators of end of life in neurological conditions10–12
Rapid deterioration in mobility.
Increasing dependence for personal care.
Rapid decline in cognitive function.
Loss of speech.
Difficulty in swallowing.
Loss of appetite and weight loss.
Increasing fatigue.
Recurrent aspiration pneumonia.
Respiratory failure.
Awareness about these indicators will promote identification of the end-of-life phase that in turn enables a proactive approach to begin discussions about the patient’s priorities and planning for their care and support during end of life.
How to talk about progressing condition/end-of-life phase
Identifying triggers (from the list above) gives an opportunity to open discussions with the patient and those important to them about their condition. The nature of many neurodegenerative conditions is such that capacity to make decisions can become impaired, and so early discussions give the patient a better chance to be included in decisions about their end-of-life care. The prognosis may guide the urgency of discussions but not everyone wants to engage in considering the future or wants to know about their expected prognosis. We must therefore explore the patient’s readiness for these discussions sensitively.
There are many techniques for talking about these challenging issues. Open questions allow clinicians to assess the person’s current understanding and to try to gauge whether they are ready for further conversations. Structuring consultations may help and there are many communication tools to support this: one example is the REMAP model (table 1).13
REMAP model for end-of-life communication13
These conversations can be difficult, and patients and carers need support during the process. It may be necessary to arrange further reviews, maybe with a nurse specialist or members of the wider multidisciplinary team. No matter how thorough the conversations are, the patient needs a point of contact to call for further information and additional support.
Although these discussions should be individualised, there are some key things to explore: milestones in disease progression, the shifting focus from disease-modifying treatments towards management of symptoms and advance care planning.
How to begin planning end-of-life care
Having recognised that the patient may be in the end-of-life phase (ie, the last year of life), healthcare professionals should sensitively offer opportunities to consider planning for future care, including at the end of life. For some patients, it may be more effective and acceptable to start with planning for the short term (next week/next month), before leading on to the end-of-life discussions. These conversations are often evolving discussions, which therefore are unlikely to take place in one sitting or one clinic appointment. Promptly communicating the content of any initial conversations to other people supporting that person can allow them also to progress discussions. When someone is identified as likely being in their last year of life, the general practitioner needs to be informed to ensure that the patient is added to any local registers.
An overarching goal of all discussions, no matter who has prompted them, is to understand better what matters to that individual; knowing what they most value and what they most fear forms a useful framework for care planning. This is the model used in Recommended Summary Plan for Emergency Care and Treatment approach.14
People do not always know what services and supports are available to them. They may have a preference over their desired place of death; where possible, it is important to share their views with those with whom they live. Hospital-based teams may not be familiar with community services, especially if a patient has come to a tertiary clinic, therefore it is important to involve primary care and other local services in these discussions.
Options for advance care planning
The outputs that may arise from these discussions are often covered in the ‘catch-all’ term ‘advance care plan’, which may include both legally binding and legally non-binding elements (table 2). For those who lack capacity to discuss their treatment plans, it is necessary to involve a lasting power of attorney, where they have been appointed. Decisions that are made through a best interests process should involve any appropriate family/friends, although the decision ultimately lies with the lead clinician. In the absence of family or friends, an independent mental capacity advocate should be arranged (figure 1).
Advance care plans/processes
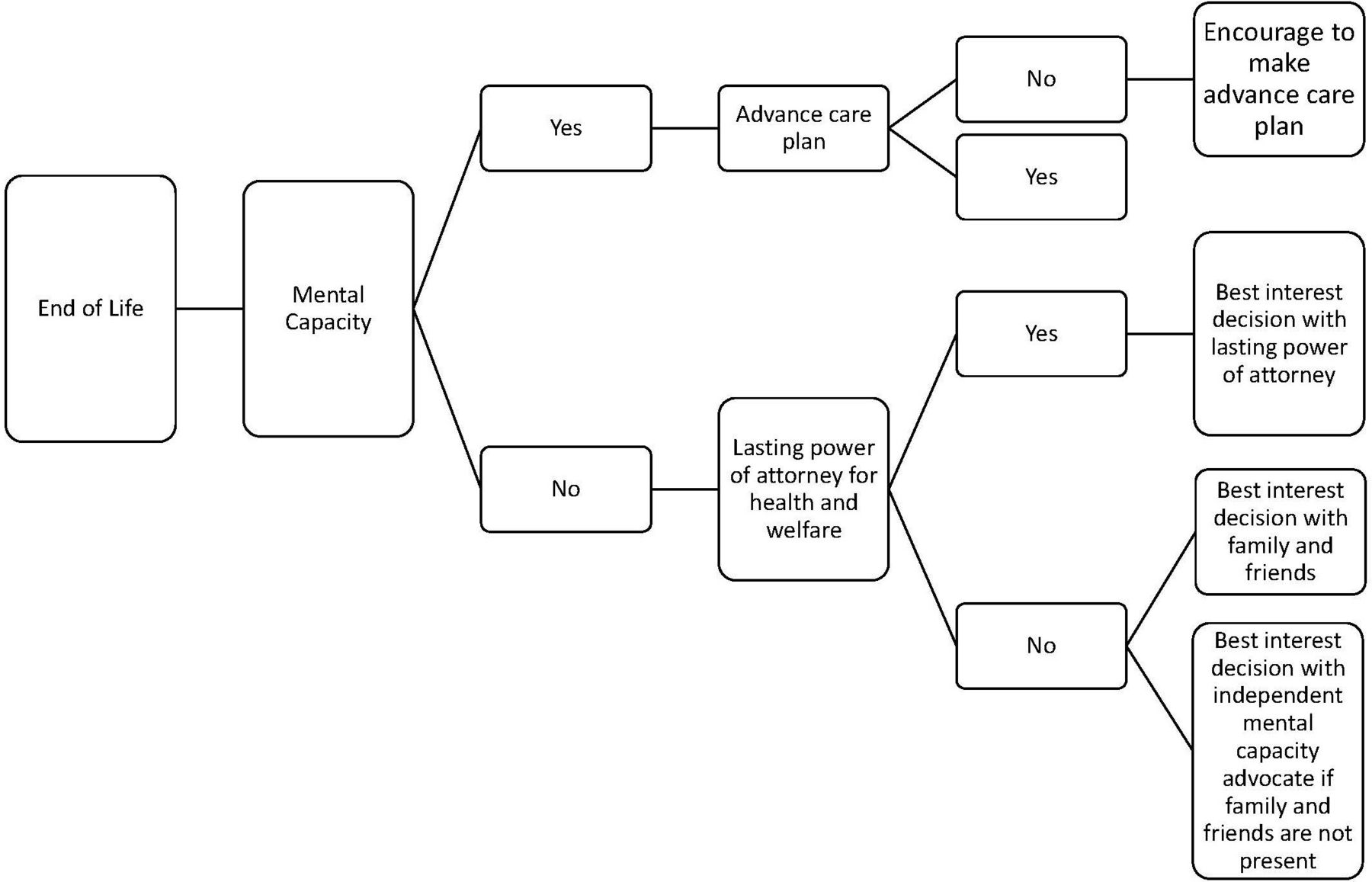
Advance care planning: the process.
The treating team should explore whether any advance care plans are already in place, particularly those that are legally binding. These can be used to inform discussions and decision-making when the patient loses the capacity. By having a better understanding of a patient’s preferences and goals, clinicians can ensure decision-making is guided by the patient’s priorities, for example, how much value to place on quality of life versus life-sustaining treatment. Any advance care plans should ideally be accessible to all care teams, including ambulance services, the local emergency department and general practitioners. There will be different ways to add such alerts in all areas, often through electronic patient record systems such as Summary care record or Electronic Palliative Care Co-ordination Systems, although there can still be a heavy reliance on people seeing the paper copy.15 Knowledge of systems being used locally can be sought from general practitioners and specialist palliative care teams.
Requests for euthanasia and assisted suicide
People may wish to discuss an assisted death when addressing future care planning. Euthanasia (where a clinician administers medication with the intention of causing death) and physician-assisted suicide (where a clinician provides medication for self-administration by the patient that will result in death) are both currently illegal in the UK.16 These processes are legal in a small but growing number of countries. An expression of a desire to hasten death is often a cry for help and a desire to regain some control. Where patients make such requests, clinicians should always undertake a holistic assessment of any physical/emotional/psychological and emotional suffering and address these where possible, including assessing for and treating depression. A referral to specialist palliative care services for additional support may be indicated, allowing further discussion about an individual’s needs and priorities. Patients need an honest and open discussion with someone who has capacity about the options that are open to them wherever they live. In the UK, this might include completion of an advance decision to refuse treatment (or regional equivalent) and the option to withdraw life-sustaining treatments. The British Medical Association has produced guidance on how to respond to a patient request for assisted dying.17 The House of Lords has been debating changes in the law around physician-assisted suicide and euthanasia, and so guidance may change in the coming years.
Withdrawing life-sustaining treatments
Withdrawal of treatments often poses complex ethical dilemmas. Ethically and legally withholding of treatments and withdrawal of treatments are usually seen as being the same. In these situations, it can be very helpful to involve the specialist palliative care team. In neurodegenerative conditions, the most common treatments that can be withdrawn are non-invasive ventilation or artificial nutrition/hydration.
Patients with capacity can request withdrawal of these treatments at any time. A patient may have documented in an advance decision to refuse treatment the point at which they would no longer wish for life-sustaining measures to be continued. With someone lacking capacity, if they have an appointed lasting power of attorney for health and welfare, the attorney(s) can request withdrawal on their behalf. Where someone lacks capacity but has no appointed lasting power of attorney, decisions would be made using a best interests approach.
If withdrawal is agreed to be the right approach, planning for the event should be undertaken promptly; this will probably be led by specialist palliative care and specialist respiratory teams. Neurology services may not be the lead but are likely to be part of multidisciplinary team discussions, particularly with a best interests decision.
Guidelines on supporting withdrawal of ventilation and nutrition/hydration can provide information on the use of medications to ensure comfort.18–20
It is important to plan support for the multidisciplinary team before, during and after any withdrawal of treatment, with an opportunity to discuss the ethical dilemmas and clarify the legalities of the process. If there is still uncertainty around a decision, local ethical committees may be able to provide an independent review.
How to manage symptoms in a dying person
People with neurodegenerative conditions can deteriorate and die suddenly, sometimes in their sleep. The potential for sudden and therefore unpredicted, if not unexpected death, reinforces the importance of advance care planning to avoid inappropriate or unwanted interventions, such as attempted cardiopulmonary resuscitation. A more predictable decline is also possible. Box 1 highlights some of the indicators to look for.
In the event of diagnosing dying as imminent, likely within days to weeks, enacting any agreed care guidance can support next steps. The neurologist’s role here may be to confirm the assessment of primary care or other teams, and to provide medication advice, rather than seeing a patient if they are being cared for outside of the acute hospital. National Institute for Health and Care Excellence (NICE) guidance encourages open communication with a patient and those important to them; such communication is important in guiding people through changes and helping them to understand what will probably happen and what ‘expected dying’ might look like.21
Anticipatory prescribing for the dying phase is largely a standardised process for any health condition and local guidance will usually be available. This includes recommending medications by subcutaneous injection—recognising that the oral route is often lost—for common symptoms such as pain, breathlessness, agitation, secretions and nausea.22 If the patient can no longer take their usual medications for spasticity or pain, it is important to consider using other preparations to try to minimise their burden. For more complex medication regimens, it is best to liaise with specialist palliative care teams; there may also be disease-specific medication considerations (table 3).
Management of Parkinson’s disease and seizures during end of life
Hydration and nutrition can be a hugely concerning issue for families. When someone who would usually take food/fluid orally is dying, their desire to eat and drink naturally diminishes as they deteriorate. It is important to reassure those important to the person that the patient is not starving or dehydrating to death. If there are concerns around symptoms of dry mouth or thirst, it can be worth considering a trial of subcutaneous fluids with careful review of response and stopping after 48 hours if there is no benefit. Routine mouth care is widely recognised as a crucial part of care of the dying and should be encouraged, as well as offering sips of fluid as appropriate.
For people who are artificially fed/hydrated, it can be difficult to change regimens, even if dying is recognised. It is important to discuss the usual processes as above and to try to mirror these by reducing and sometimes stopping enteral regimens. It is important to reinforce that this is not causing that person to starve/dehydrate or even causing them to die, because the dying process is already happening.
It is important to address spiritual and religious needs appropriately; ideally these will already be known. Families/carers, including informal carers who may have known a patient for a long time, should be offered access to appropriate emotional support. The death of a person with a longstanding neurodegenerative condition can mean a loss of their caring role, possibly their income and even where they live, and so the process of bereavement can be complex.
How to involve specialist palliative care services
Most patients’ end-of-life care can be managed by primary care teams and an important first step is to work in partnership with primary care services.
People often associate specialist palliative care only with death and dying but it is also about supporting and improving quality of life through planning and symptoms management. The involvement of specialist palliative care in neurodegenerative conditions will be guided by the patient’s needs; they do not need to be dying or even in the last year of their life to benefit from specialist palliative care input and timely discussions with local teams can be very helpful. They may already form part of multidisciplinary team clinics, where their introduction is seen as part of the routine care. Referrals to specialist palliative care could be considered in two circumstances.
Referrals for brief targeted palliative care interventions
Specialist palliative care teams can provide input for distressing physical symptoms such as pain, breathlessness, drooling and constipation that usual measures are not improving.7 23 24 They may offer assessment and advice; ongoing care can then continue with the neurology team with further referrals made as required (figure 2). They can help in managing challenging ethical dilemmas or complex needs of the patient and/or family. For example, in motor neurone disease, early referral to specialist palliative care may be useful to discuss interventions, such as gastrostomy or ventilatory support (figure 2).

Brief targeted specialist palliative care intervention.
Referrals for end-of-life care intervention
Patients who are approaching the end of life can benefit from palliative care interventions for the following23–26:
To address complex/unmet physical, psychosocial and spiritual needs.
For referral to local hospice services that may have inpatient and day hospice/family support/bereavement services.
For withdrawal of life-sustaining interventions.
Figure 3 shows a model incorporating neurology and specialist palliative care in managing long-term neurological conditions.

{kind=link}
{kind=link}
{kind=link}
A model incorporating neurology and specialist palliative care in the management of long-term neurological conditions.
Conclusions
All the inherent uncertainties of progressive neurological conditions make management of end-of-life care complex. Neurologists play an important role in helping patients, families and other healthcare professionals to navigate the end-of-life phase. Collaboration with specialist palliative care teams can help with advance care planning, managing refractory symptoms, withdrawing life-sustaining treatments, dealing with psychological and spiritual issues, and supporting families who are struggling to cope.
Table 4 provides hyperlinks for web-based learning resources on this topic.
Web-based resources on end-of-life care
Key points
Clinicians should support patients and family to explore advance care planning in a timely fashion, especially if the disease risks them losing mental capacity to make decisions.
Clinicians should try to understand a person’s priorities to focus care and ensure that unwanted or inappropriate treatments are not offered; this might include avoiding hospital admission if this is their preference.
Brief, targeted involvement of specialist palliative care teams can help in managing refractory symptoms, even well before the end-of-life phase.
Psychological and spiritual issues may greatly impact quality of life at the end of life.
Families and carers should be offered support throughout their loved one’s illness, including into bereavement.
Further reading
Oliver DJ, Borasio GD, Caraceni A, et al. A consensus review on the development of palliative care for patients with chronic and progressive neurological disease. Eur J Neurol 2016;23:30–8.
Faull C, Oliver D. Withdrawal of ventilation at the request of a patient with motor neuron disease: guidance for professionals. BMJ Supp Pall Care 2016;6:144–6.
Wilbin L, Lee M, Burn D. Palliative care and its emerging role in Multiple system atrophy and progressive supranuclear palsy. Parkinsonism and Related Disorders 2017;34:7–14.
Hobson EV, McDermott CJ. Supportive and symptomatic management of amyotrophic lateral sclerosis. Nat Rev Neurol 2016;12:526–38.
Data availability statement
Data sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statements
Patient consent for publication
Ethics approval
Not applicable.
Footnotes
Twitter @drestherhobson
Contributors All authors contributed to the concept, literature review, drafting and reviewing of this article.
Funding This review was supported by the NIHR Sheffield Biomedical Research Centre (BRC)/NIHR Sheffield Clinical Research Facility (CRF).
Disclaimer The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health and Social Care (DHSC).
Competing interests None declared.
Provenance and peer review Commissioned. Externally peer reviewed by Kevin Talbot, Oxford, UK, and Annabel Howell, Melrose Scottish Borders, UK.
Other content recommended for you
- Rehabilitation medicine in palliative care of chronic neurological conditions
- An introduction to advance care planning in practice
- Lesley's story: a case report, and discussion of challenges faced in end-of-life care for progressive neurological disease
- Improving electronic information sharing for palliative care patients
- Assisted ventilation in motor neurone disease during inpatient palliative care: barriers and utilisation
- Coordinate My Care: a clinical service that coordinates care, giving patients choice and improving quality of life
- Electronic palliative care coordination systems (EPaCCS): a systematic review
- Building on sand: digital technologies for care coordination and advance care planning
- Crash course in EPaCCS (Electronic Palliative Care Coordination Systems): 8 years of successes and failures in patient data sharing to learn from
- Care of the dying patient in the community