Article Text

Statistics from Altmetric.com
Background
The diagnostic criteria for multiple sclerosis (MS), first developed in the 1950s, have since undergone several revisions, all focused on three main requirements for a diagnosis of MS:
Objective clinical evidence of central nervous system (CNS) involvement.
Evidence of lesions disseminated in time and space.
Exclusion of other conditions that could better explain the clinical and paraclinical findings.
Before the widespread use of MR imaging, the criteria for dissemination in time and space were fulfilled by two attacks involving different parts of the CNS and clinical evidence of two lesions separated in time, or one attack with additional paraclinical evidence of another lesion. In 2001, McDonald et al1 fully integrated the use of MR imaging into the diagnostic schema as an alternative to clinical evidence for dissemination in time and space, allowing an earlier diagnosis of MS. The McDonald criteria were revised in 2005, 2010 and 2017, building on new evidence for the role of MR imaging.2–4 The increasing focus on the importance of early treatment of MS with disease-modifying therapies has meant that a prompt and accurate diagnosis of MS has never been more important.
Previous diagnostic criteria
The 2010 revisions to the McDonald criteria simplified the requirements for dissemination in time and space on MRI and removed neurophysiological and cerebrospinal fluid (CSF) testing from the diagnostic criteria (for relapsing–remitting MS). Dissemination in space on MRI required at least one T2 lesion in at least two of four locations characteristic of MS (periventricular, juxtacortical, infratentorial and spinal cord), and dissemination in time required the simultaneous presence of gadolinium-enhancing and non-enhancing lesions, or a new T2 or gadolinium-enhancing lesion on a follow-up MRI. For the first time, a diagnosis of MS could be made in some patients with clinically isolated syndrome using a single contrast-enhanced MR scan. However, there were two main caveats:
The criteria would be applied only when MS was already the most likely diagnosis: where this was not the case, then both neurophysiological and CSF studies still had a clear role.
The criteria treated symptomatic and asymptomatic lesions differently: only asymptomatic lesions could contribute to dissemination in time and space using MRI.
The main changes in the new diagnostic criteria
The 2017 revision of the McDonald criteria (figure 1) further simplify the diagnostic process in patients with clinically isolated syndrome. The first major change is the reintroduction of CSF oligoclonal bands, which have been shown to predict a second clinical attack following a clinically isolated syndrome in patients with MRI evidence of dissemination in space.5 In a typical patient with clinically isolated syndrome showing dissemination in space, the presence of unmatched CSF oligoclonal bands now permits a diagnosis of MS, even without dissemination in time on MRI or a second attack (figure 2). Moreover, there is no longer a distinction between symptomatic or asymptomatic lesions; both, with the exception of optic nerve lesions, can contribute to the MRI determination of dissemination in time and space. The 2017 criteria also allow for cortical lesions, which are common in MS, to contribute to the determination of MRI dissemination in space. The requirements for the diagnosis of primary progressive MS have not changed compared with past versions, apart from the removal of the distinction between symptomatic and asymptomatic lesions and the inclusion of cortical lesions.

Diagram or visual summary of the last revision of the MS diagnostic criteria. According to the glossary provided by Thompson et al,4 in the figure, the term ’lesion(s)’ refers to ’an area of hyperintensity on a T2-weighted or proton-density weighted MRI scan that is at least 3 mm in long axis’. CIS, clinically isolated syndrome; CNS, central nervous system; CSF, cerebrospinal fluid; DIS, dissemination in space; DIT, dissemination in time; MS, multiple sclerosis; WM, white matter.
{kind=link}
{kind=link}
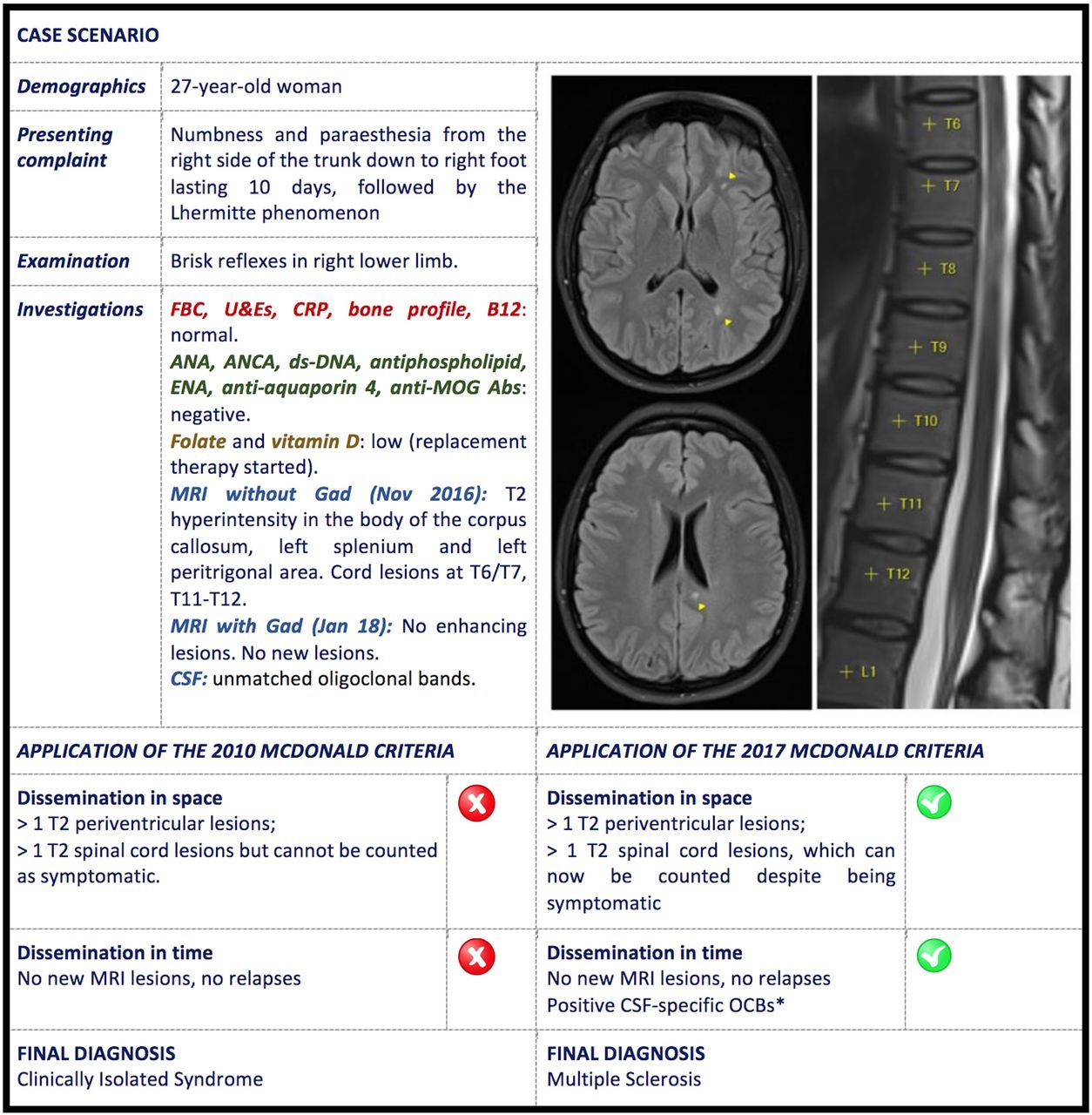
Adapted clinical case showing different diagnostic outcomes after the application of the old and the new diagnostic criteria. *The presence of CSF-specific OCBs does not conclusively demonstrate dissemination in time per se but can substitute for the requirement for demonstration of this measure. CSF, cerebrospinal fluid; Gad, gadolinium; OCBs, oligoclonal bands.
Commentary
MR imaging can demonstrate dissemination in time and space, which are at the core of MS diagnosis, and the revised criteria now recognise cortical involvement in MS while also simplifying the MRI dissemination in time and space requirements. However, MRI lesions similar to those found in MS can occur in other disorders, and MRI criteria should not be applied in patients with atypical clinical presentations.6 If there is doubt regarding the nature of symptoms or signs, patients require further evaluation.7 The 2017 criteria should be applied with caution in geographical areas that have a lower incidence of MS, in younger children and older adults, and those with comorbidities (eg, migraine or small vessel disease) in order to avoid misdiagnosis. Particular attention is necessary to rule out neuromyelitis optica spectrum disorder, especially in African–American, Asian, Latin American and paediatric populations, where this disease is relatively more common. There remains further scope for the current 2017 diagnostic criteria to be refined further. For example, despite the specificity of cortical lesions for MS, they still cannot be detected as easily as white matter lesions using MRI techniques available clinically. The visual system is also often involved in MS, yet the role of optic nerve MRI, visual evoked potentials or optical coherence tomography in fulfilling dissemination in time and space remains uncertain. Moreover, the incidental finding of white matter lesions on MRI that fulfil MS radiological diagnostic criteria (termed a radiologically isolated syndrome) remains a cause of clinical uncertainty that the 2017 criteria have not resolved.8
Changes in MS diagnostic criteria have also raised questions about the use of disease-modifying therapies following a clinically isolated syndrome. The evidence for using these following a clinically isolated syndrome comes from clinical trials that used pre-2010 diagnostic criteria, that is, where a significant proportion of those enrolled in studies would now fulfil the diagnostic criteria for MS, and so it is unclear if their efficacy would be the same in people now classified as having a clinically isolated syndrome rather than MS. This point has recently been a matter of discussion for the National Institute for Health and Care Excellence.9
In conclusion, the new diagnostic criteria can be applied easily and allow for a more streamlined diagnosis of MS. However, they do not replace physicianly judgement and should never be applied without careful clinical evaluation.
Footnotes
Contributors FDA and SAT were involved in the conception and design of the article, drafting, revision and final approval of the manuscript for publication. WJB and DTC were involved in the conception and revision of the manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors. DTC and SAT are supported by the National Institute for Health Research University College London Hospitals Biomedical Research Centre.
Competing interests WJB reports personal fees from Roche and personal fees from Merck Serono, outside the submitted work. DTC has received, within the last 2 years, honoraria (paid to his employer) from Excemed for faculty-led education work, and meeting expenses from Novartis and Société des Neurosciences, outside the submitted work. SAT reports a personal fee from Roche, a personal fee and non-financial support from Novartis, a personal fee from Merck Serono, personal fees and non-financial support from Teva, and non-financial support from Biogen, all outside the submitted work.
Patient consent Obtained.
Provenance and peer review Commissioned; externally peer reviewed by Alasdair Coles, Cambridge, UK.
Read the full text or download the PDF:
Other content recommended for you
- Spinal cord MRI in clinically isolated optic neuritis
- Imaging in multiple sclerosis
- Multiple sclerosis
- Modification of MRI criteria for multiple sclerosis in patients with clinically isolated syndromes
- Prognostication and contemporary management of clinically isolated syndrome
- Prediction of conversion from clinically isolated syndrome to clinically definite multiple sclerosis according to baseline MRI findings: comparison of revised McDonald criteria and Swanton modified criteria
- Application of the 2012 revised diagnostic definitions for paediatric multiple sclerosis and immune-mediated central nervous system demyelination disorders
- Tumefactive demyelination: an approach to diagnosis and management
- CNS inflammatory demyelinating disorders: MS, NMOSD and MOG antibody associated disease
- MRI only conversion to multiple sclerosis following a clinically isolated syndrome