Article Text

Statistics from Altmetric.com
Case
A 46-year-old woman presented with sudden loss of vision in both eyes, apparent since waking. She also complained of partial hearing loss. The previous evening she had experienced difficulty sleeping due to (long-standing) restless legs and had self-medicated with quinine, taking an accidental overdose of 1.8 g.
On admission, she was alert but unable to perceive light in either eye, and had fixed, dilated pupils. Other than mild bilateral sensorineural hearing loss, the remainder of the neurological examination was normal. She was haemodynamically stable, but her ECG showed QT interval prolongation at 501 ms (normal 350–440); she therefore received intravenous sodium bicarbonate for suspected myocardial toxicity.
Ophthalmological review that day confirmed a visual acuity of no light perception and a bilateral afferent pupillary defect. Fundal examination suggested mild retinal oedema. Given the profound visual loss, we prescribed a 4-week course of oral nimodipine 60 mg 4-hourly, based on limited evidence from case series.1
Progress
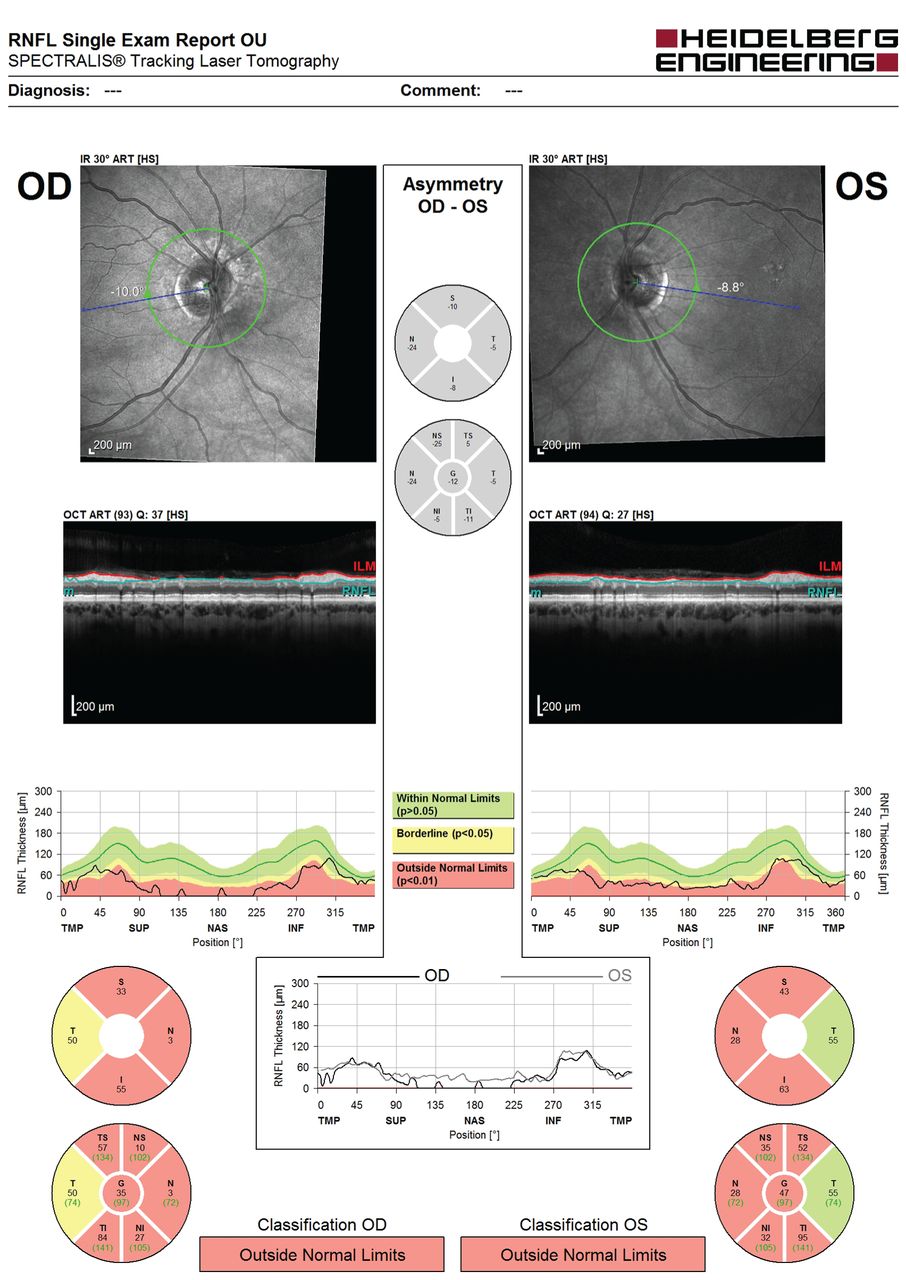
Two days postoverdose, her vision started to return such that she could perceive light. Slit lamp fundus examination was normal at this point. Her sight gradually improved. By 1 month, visual acuity was 6/9 bilaterally, although subjectively her vision was akin to ‘being under water’. Colour vision was profoundly reduced: she could discern the Ishihara control plate only. Her pupils remained persistently dilated with sluggish direct reactions to light. Funduscopy now showed optic disc pallor and retinal vessel attenuation bilaterally (figure 1), with thinning of the nasal retinal nerve fibre layer on optical coherence tomography (figure 2). Visual fields were severely constricted (figure 3A) such that she remained functionally limited. Electrodiagnostic testing at 3 months was consistent with quinine overdose, with reduced electroretinogram amplitude and abnormal flicker response.

Fundus photographs showing pale discs and retinal vessel attenuation. The patient’s fundus appearance was unremarkable in the early stages; the changes seen here were seen from 1 month postoverdose and are secondary to the widespread quinine-induced retinal toxicity. These photographs were taken at 6 months, at which point there had been some recovery of the visual function but no further change to the funduscopic appearance.
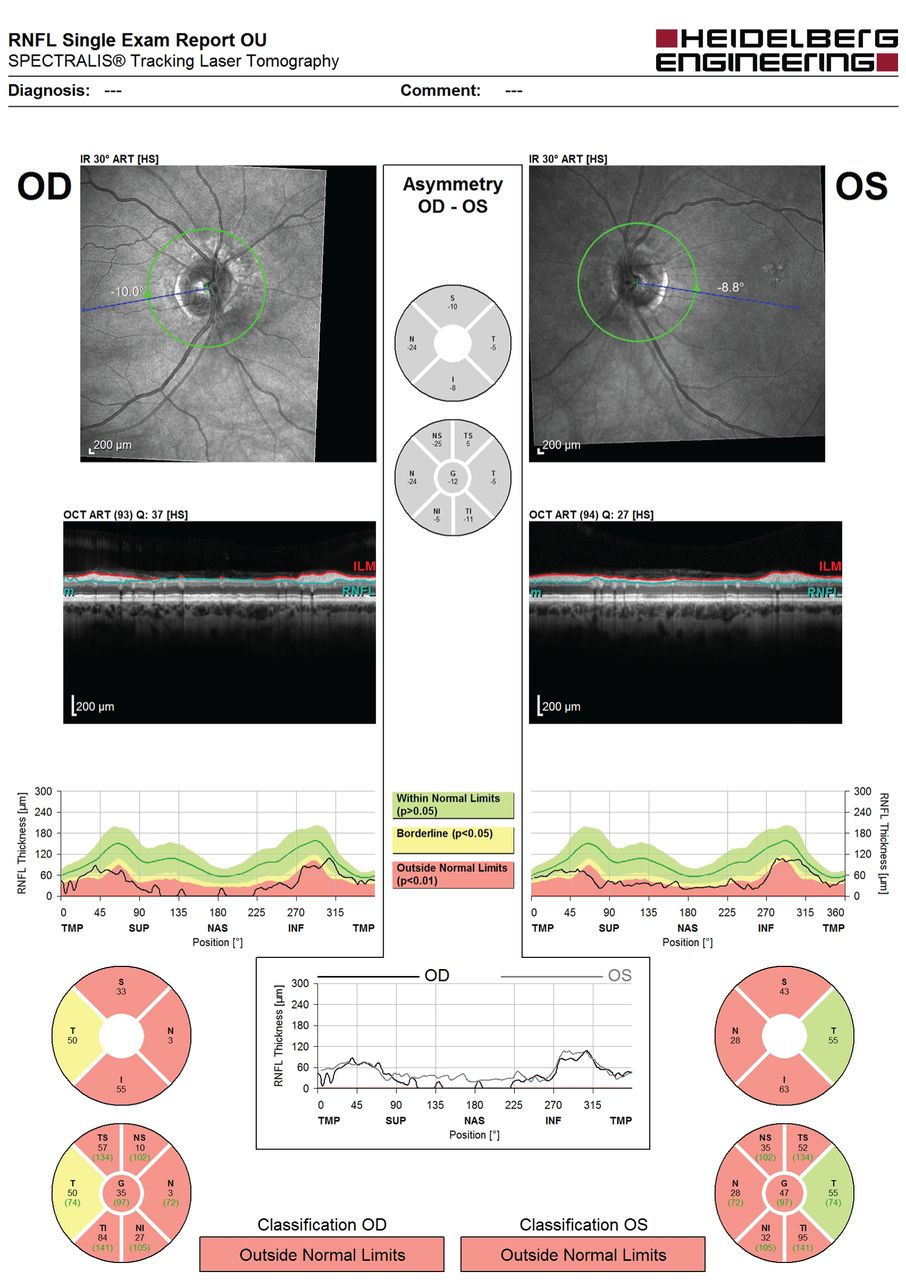
Optical coherence tomography showing thinning of the retinal nerve fibre layer (RNFL) 1 month postquinine overdose. OU, oculus uterque (both eyes); OD, oculus dexter (right eye); OS, oculus sinister (left eye).

{kind=link}
{kind=link}
{kind=link}
Humphrey perimetry (SITA-Standard 24–2): (A) 1 month postquinine overdose, showing marked constriction of the visual field; (B) 6 months postquinine overdose, showing clear improvement of the visual field defects.
Over 6 months, her visual fields expanded significantly (figure 3B), reflecting partial recovery of retinal function following quinine toxicity.
Discussion
Acute quinine toxicity produces a well-recognised constellation of clinical effects, known as cinchonism. This case demonstrated visual and hearing loss as well as signs of cardiac instability. In addition, cinchonism may comprise tinnitus, dizziness, headache, seizures and vomiting. Quinine is believed to be directly toxic to the inner retina2 and, while the natural history is of some recovery over days to weeks, residual visual field constriction is common and the vision may remain poor.
There is no high-quality evidence for any treatment for quinine-related blindness. However, due to the arteriolar constriction seen in some, there have been several case reports of treatment to alleviate vasospasm with agents such as nimodipine.1 While the retinal vasculature was unremarkable at initial assessment, we prescribed nimodipine based on the very poor level of vision and good safety profile of the medication.
Due to the narrow therapeutic range of quinine, visual effects can also rarely occur at normal doses. Furthermore, as quinine is a commonly prescribed medication, it is not always readily identified as the culprit. It should be suspected particularly in the presence of fixed, dilated pupils and other features of cinchonism.
Acknowledgments
We thank the medical photography staff at the Princess Alexandra Eye Pavilion for their help.
Footnotes
Contributors HNH and AJT saw the patient and discussed the content of the manuscript, which was then drafted by HNH and edited by AJT.
Competing interests None declared.
Patient consent Obtained.
Provenance and peer review Not commissioned; externally peer reviewed. This paper was reviewed by Neil Anderson, Auckland, New Zealand.
Other content recommended for you
- Factors affecting the diagnostic performance of circumpapillary retinal nerve fibre layer measurement in glaucoma
- Detection and characterisation of optic nerve and retinal changes in primary congenital glaucoma using hand-held optical coherence tomography
- Relatively spared central multifocal electroretinogram responses in acute quinine toxicity
- Compensation of retinal nerve fibre layer thickness as assessed using optical coherence tomography based on anatomical confounders
- The effect of myopic optic disc tilt on measurement of spectral-domain optical coherence tomography parameters
- One-year follow-up of macular ganglion cell layer and peripapillary retinal nerve fibre layer thickness changes after panretinal photocoagulation
- Effect of partial posterior vitreous detachment on spectral-domain optical coherence tomography retinal nerve fibre layer thickness measurements
- Glaucoma diagnostic value of the total macular thickness and ganglion cell-inner plexiform layer thickness according to optic disc area
- The effect of head tilt on the measurements of retinal nerve fibre layer and macular thickness by spectral-domain optical coherence tomography
- Risk factors for progressive axonal degeneration of the retinal nerve fibre layer in multiple sclerosis patients